Article Text

Statistics from Altmetric.com
Acute haemorrhagic leukoencephalitis was first described as a pathological entity by Hurst in 1941.1 It is a rare acute inflammatory myelinopathy of the CNS characterised by progressive loss of consciousness leading to coma accompanied by focal neurological dysfunction. It is now generally accepted that acute haemorrhagic leukoencephalitis is the severe end of the range of acute disseminated encephalomyelitis.2
A 34 year old man presented with rapidly progressive dysphasia, right hemiparesis, and deteriorating level of consciousness over 24 hours after a flu-like illness in the preceding week. He had no history of any other relevant previous illnesses, travel, or immunisation and was not taking any medication.
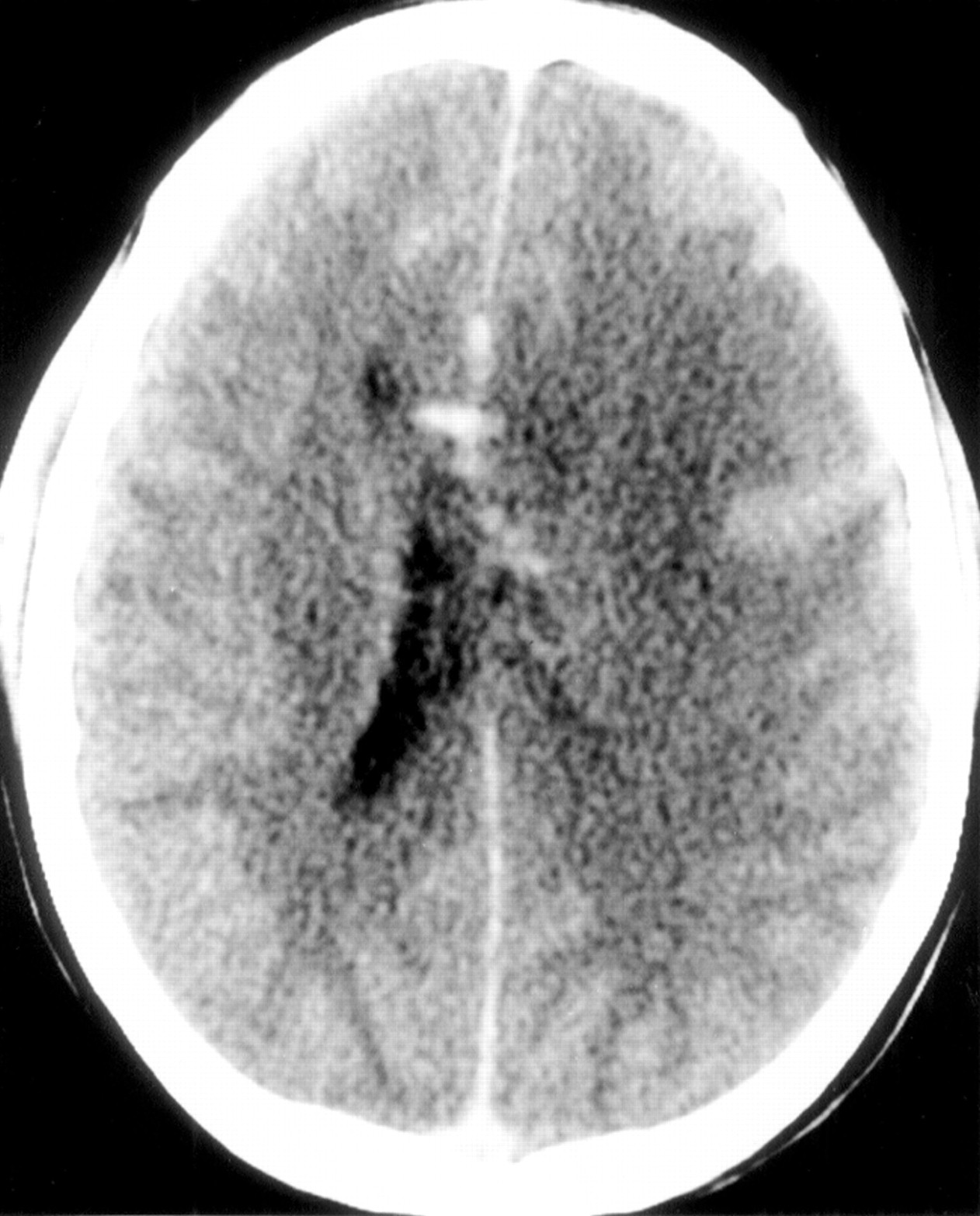
On initial examination he was febrile at 38°C. He had an expressive dysphasia, was drowsy, and had mild neck stiffness. A right central facial weakness was present and a gag reflex was absent. He moved his left arm and leg to command but only flexed his right arm and leg to painful stimuli. Computerised tomography of the brain showed left frontoparietal oedema with mass effect causing effacement of the sulci and the frontal horn of the lateral ventricle and 5 mm midline shift (fig 1).
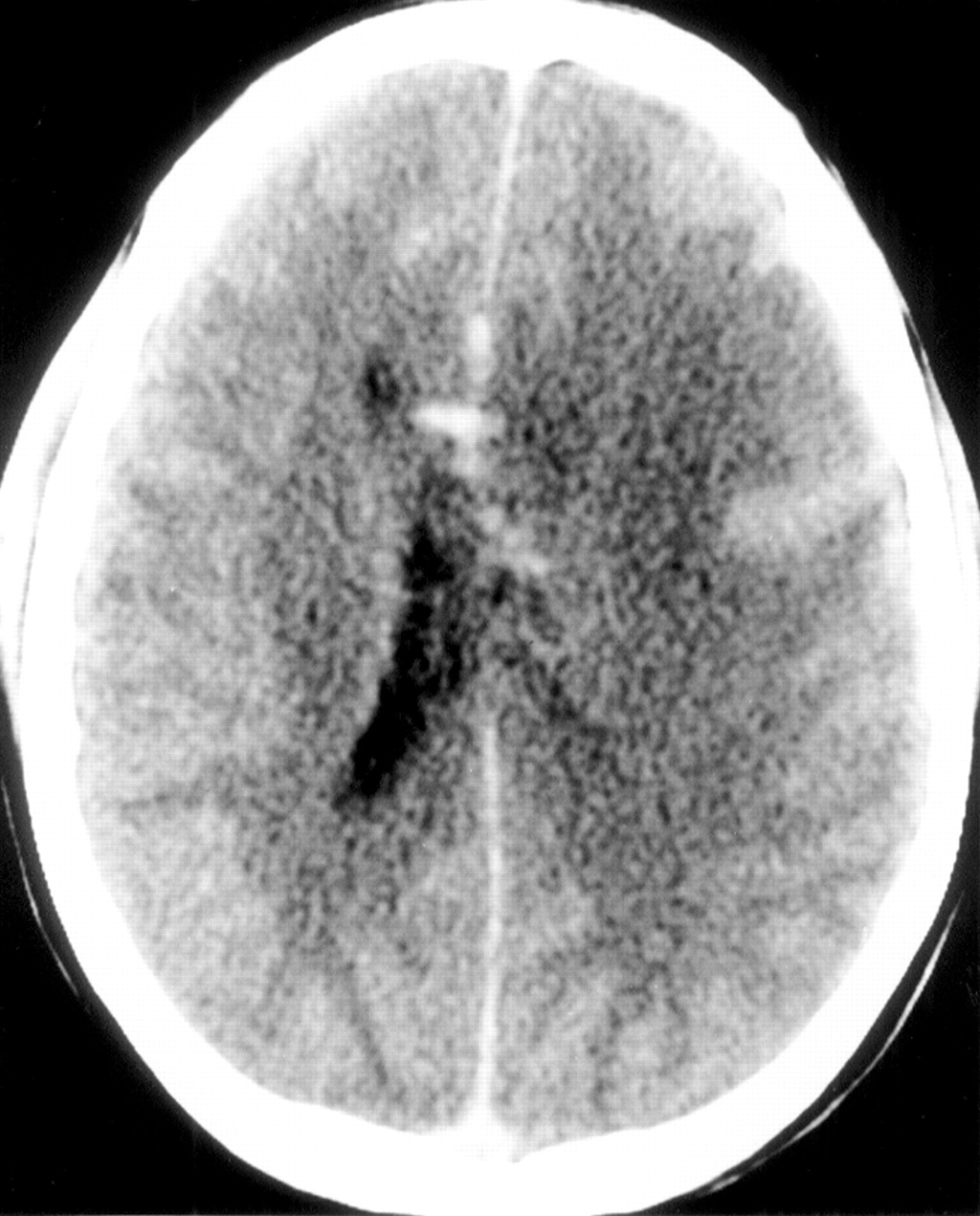
Brain CT showing left hemispheric oedema with mass effect and midline shift. There is no contrast enhancement to suggest an abscess.
There was further deterioration in his consciousness over the next several hours leading to intubation and transfer to the intensive care unit with a presumptive differential diagnosis of viral encephalitis, bacterial cerebritis, or acute disseminated encephalomyelitis. Treatment with acyclovir, ceftriaxone, flucloxacillin, phenytoin, and dexamethasone was commenced. Cerebrospinal fluid from ventricular puncture showed 25 000 red blood cells/mm3, 53 white blood cells/mm3 (72% polymorphonuclear cells, 24% lymphocytes, 4% monocytes), 1257 mg/l protein, and 6 mmol/l glucose. Gram stain, bacterial cultures, and cryptococcal antigen were negative.
On day two of the hospital admission he developed signs of increasing cerebral oedema and his intracranial pressure was 90 mm Hg (normal 15 mm Hg). Medical therapy to lower intracranial pressure was started with hyperventilation, mannitol, and lignocaine. Despite these measures the pressure remained high with haemodynamic instability. Consequently, a partial left frontal lobectomy was performed without replacement of the bone flap on day 3.
Because of his deterioration on broad spectrum antibiotics and acyclovir along with the antecedent flu-like illness, a presumptive diagnosis of acute haemorrhagic leukoencephalitis was made and 1000 mg methylprednisolone daily for three days was given. Subsequently, histology of the brain biopsy confirmed the clinical diagnosis (fig 2). Immunoperoxidase for herpes simplex virus was negative. Polymerase chain reaction amplification of herpes simplex type 1 DNA on brain tissue and in CSF was negative.

{kind=link}
{kind=link}
Luxol fast blue stain for myelin showing perivenous demyelination and punctate haemorrhages (original magnification ×10).
Intravenous immunoglobulin was given at a dose of 30 g daily for five days initially but the patient remained in coma. Plasmapheresis (five 2 l exchanges on alternate days) and 100 mg/day cyclophosphamide were commenced on day 9. Methylprednisolone was given at a dose of 1000 mg daily for a further five days followed by a reducing course of steroid.
First signs of recovery were noted on day 14 when he opened his eyes and moved his left hand to command. He was extubated on day 17. Steady neurological recovery continued and he was walking with assistance and speaking by day 30. Cyclophosphamide and steroids were ceased on day 40 and 50 respectively. At four months a cranioplasty was performed. At nine months he is back at work as an accountant and sailing competitively with minimal neurological deficit.
Aggressive treatment of patients with acute haemorrhagic leukoencephalitis may lead to a favourable outcome despite the presence of severe neurological disability at the beginning of the illness.3-5 Recognition of acute haemorrhagic leukoencephalitis may be difficult but there are several useful clinical signals: (a) the antecedent flu-like illness, (b) early changes on brain CT,6(c) the presence of red cells and a neutrophil pleocytosis in the CSF, and (d) deterioration despite broad spectrum antibiotics and antiviral therapy. Brain biopsy, however, is essential for diagnosis.
Management consists of early diagnosis, aggressive control of raised intracranial pressure in intensive care, and immunosuppressive therapy with a combination of corticosteroids, plasmapheresis, and cyclophos- phamide. Immunosuppressive treatment for acute haemorrhagic leukoencephalitis is based on the assumption that it is an autoimmune disorder. The strongest evidence for this comes from its similarity to experimental allergic encephalomyelitis and in humans with acute disseminated encephalomyelitis there is evidence of activation of autoreactive T cells against myelin basic protein.7 8 Of the immunological therapies that have been reported to be effective it is not clear which is superior or which combination is best. Nonetheless, in a severely disabled patient it would seem prudent to maximise treatment.