
Abstract
Summary: Hypertensive encephalopathy rarely presents with predominant involvement of the brain stem and relative sparing of the supratentorial regions. We describe the MR imaging features in a patient with reversible brain stem hypertensive encephalopathy. Extensive hyperintensity was predominantly seen in brain stem regions on fluid-attenuated inversion-recovery and T2-weighted images. These lesions showed an increased apparent diffusion coefficient with the use of line scan diffusion-weighted imaging. The clinical findings and MR imaging abnormalities resolved with control of hypertension.
Hypertensive encephalopathy is a serious condition manifested by headache, visual disturbances, altered mental status, seizures, and focal neurologic signs (1, 2). This condition is a medical emergency caused by a sudden increase in arterial blood pressure. If untreated, hypertensive encephalopathy may rapidly lead to coma and death (3).
The typical MR imaging finding in hypertensive encephalopathy is T2 hyperintensity, predominantly within the cortex and subcortical white matter of the occipital lobes bilaterally, although not with perfect symmetry (4, 5). It has been recognized that quantitative assessment of diffusion changes can help identify vasogenic edema in this condition (6), which is potentially reversible if appropriately managed. Although the combination of typical MR findings and clinical evidence of hypertension may easily suggest the diagnosis of hypertensive encephalopathy, unusual MR findings with predominant brain stem involvement pose a diagnostic dilemma (7, 8). In the case presented here, we demonstrate the MR findings of brain stem hypertensive encephalopathy and emphasize the diagnostic value of diffusion-weighted imaging (DWI).
Case Report
A 67-year-old man presented with diffuse weakness, generalized edema, and visual disturbances. His medical history included poorly controlled hypertension and diabetes mellitus. On neurologic examination, he was drowsy but able to follow simple commands. Hemiparesis was not found. Physical examination revealed blood pressure of 230/122 mm Hg. Funduscopic examination showed findings of severe hypertensive and diabetic retinopathy. The blood creatinine level was elevated (3.6 mg/dL; normal, 0.4–1.4 mg/dL). Blood electrolyte levels were normal.
MR imaging was performed by using a 1.5-T system. Extensive hyperintensity was observed in the brain stem and dentate nucleus on T2-weighted and fast fluid-attenuated inversion-recovery (FLAIR) images (Fig 1A and B). On MR images, the pons was seen to be swollen. Periventricular hyperintensities were also observed, but no abnormalities were found in the cortical and subcortical regions of the cerebrum (Fig 1C). At that time, the differential diagnosis included acute infarction, osmotic myelinolysis, and brain tumors such as gliomas, encephalitis, and hypertensive encephalopathy.
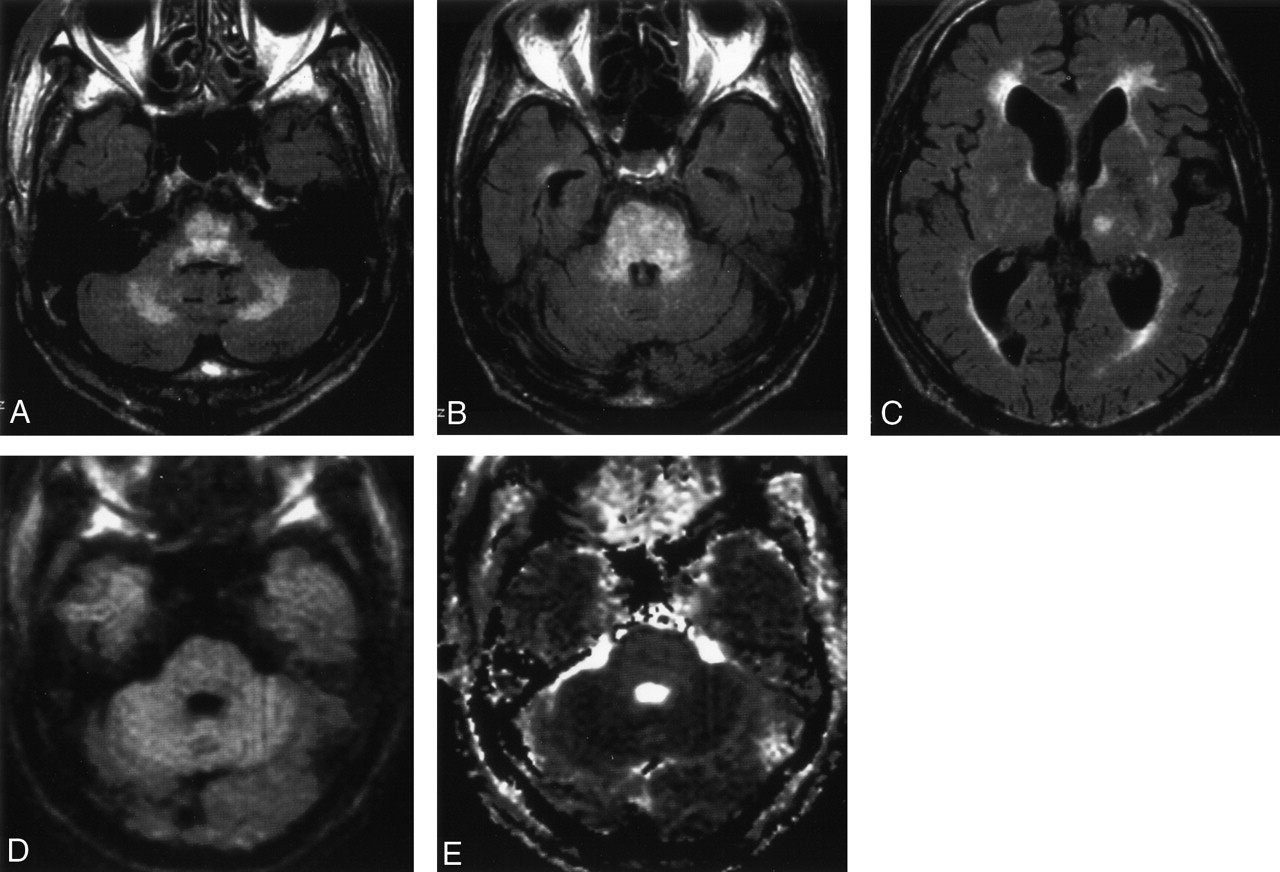
Initial MR images obtained in a 67-year-old man with hypertension.
A, B, Fast FLAIR images show an extensive brain stem lesion. The dentate nucleus is also involved.
C, Fast FLAIR image shows periventricular hyperintensities.
D, Trace LSDWI (b = 1000 s/mm2) shows isointensity in the brain stem.
E, Corresponding ADC map shows increased diffusion in the brain stem lesions (1.04 ± 0.04 × 10−3 mm2/s), indicating vasogenic edema.
Line scan diffusion-weighted imaging (LSDWI) was also performed for the brain stem lesions (Fig 1D). The LSDWI technique has been described elsewhere (9, 10). The b values used were five and 1000 s/mm2 as the maximum b value applied along the three orthogonal directions. The other parameters for LSDWI were as follows: TR/TE/NEX, 2376/57.7/1; field of view, 24 × 18 cm; effective section thickness/gap, 5/1 mm; and acquisition matrix, 128 × 128. The total imaging time was 2 minutes 27 seconds for five images. Apparent diffusion coefficient (ADC) maps were generated and displayed on a console. ADC values were calculated for the quantitative assessment of diffusion. The ADC maps showed increased diffusion in the brain stem lesions (Fig 1E), and the ADC value (mean ± SD) was 1.04 ± 0.04 × 10−3 mm2/s. From the results of the increased diffusion in the lesions, acute infarction of the brain stem was readily ruled out. The relative paucity of neurologic symptoms and normal blood electrolyte levels made tumor, encephalitis, and osmotic myelinolysis unlikely, although they could not be completely ruled out. The very high blood pressure and increased diffusion favored a clinical diagnosis of brain stem hypertensive encephalopathy.
Treatment was initiated with antihypertensive medication, and hemodialysis was subsequently performed. The patient’s blood pressure was reduced to 150/80 mm Hg, followed by a decrease in drowsiness. Follow-up MR imaging was performed 2 weeks after the initial MR examination. MR images showed complete resolution of the brain stem and cerebellar lesions, and periventricular hyperintensities decreased to some degree (Fig 2A–C). The ADC maps appeared almost normal in the brain stem (Fig 2D). The ADC values of the brain stem were normalized to 0.84 ± 0.02 × 10−3 mm2/s.
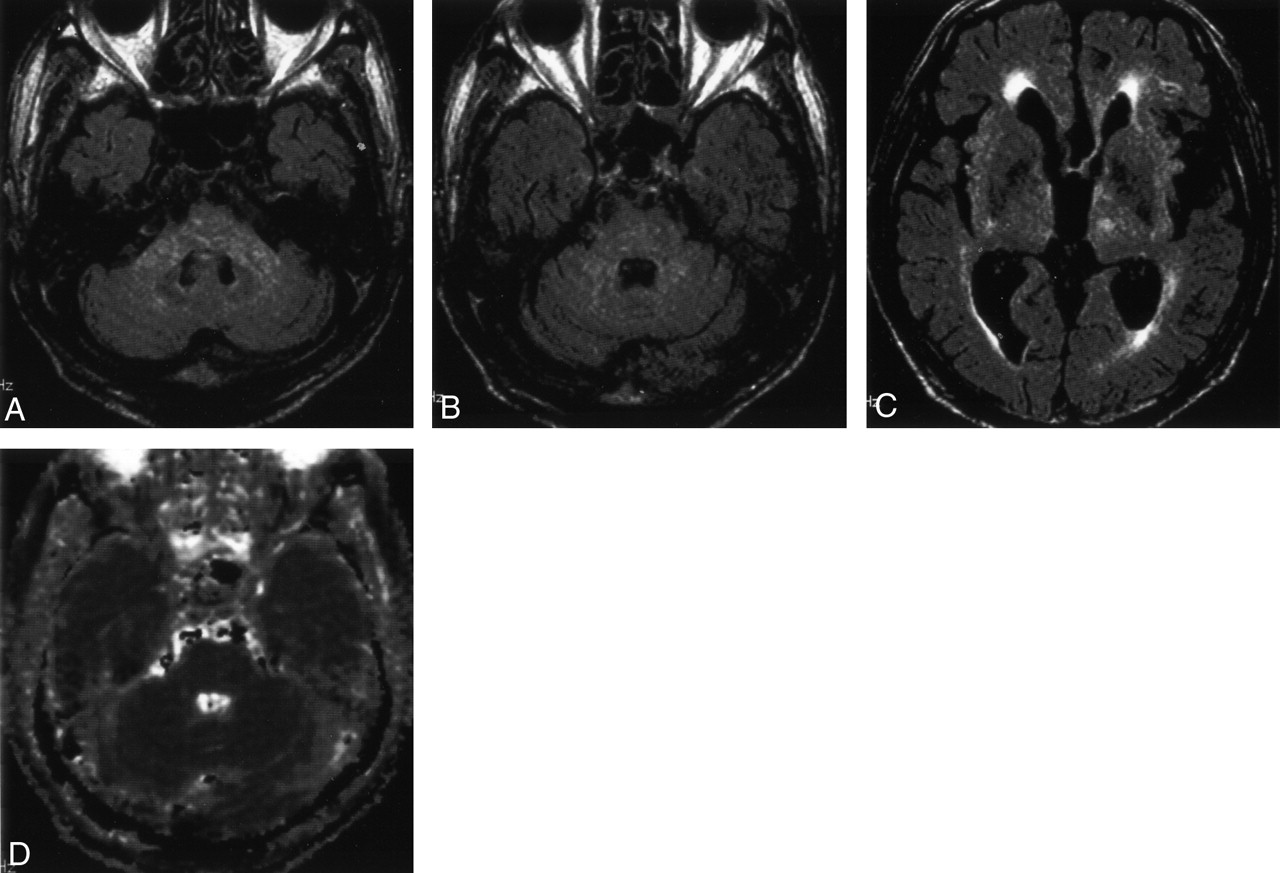
Follow-up MR images 2 weeks after initial MR imaging.
A and B, Fast FLAIR images show complete resolution of the brain stem and cerebellar lesions.
C, Fast FLAIR image shows that the periventricular hyperintensities decrease to some degree.
D, ADC map appears normal. The ADC of the brain stem is 0.84 ± 0.02 × 10−3 mm2/s.
Discussion
The clinical features of the case presented here were strongly suggestive of hypertensive encephalopathy, with drowsiness associated with severe hypertension and subsequent improvement after a reduction in blood pressure. The MR imaging findings were unusual in our patient with hypertensive encephalopathy, because the predominant involvement of posterior cerebral regions is recognized to be a hallmark of this disease (4, 5). Despite the emphasis on posterior supratentorial lesions, associated involvement of the brain stem and cerebellum is not rare. In one study of 36 patients with hypertensive encephalopathy (11), 32 patients had supratentorial lesions, whereas 15 had brain stem lesions and 11 had cerebellar lesions. Although predominant brain stem lesions, as seen in our case, are uncommon in hypertensive encephalopathy, a few cases with predominant involvement of the brain stem have been reported (12–16).
It has been proposed that the characteristic appearance of lesions within the posterior circulation results from regional differences in the distribution of intracranial adrenergic receptors (17). Vessels in posterior circulation have a sparse sympathetic innervation and are therefore poorly equipped to initiate protective vasoconstriction in response to a sudden increase in arterial blood pressure, resulting in disruption of blood-brain barrier and passive extravasation of fluid into the interstitium. Kumai et al (16) suggested that severe acceleration of hypertension is required, particularly for hypertensive brain stem encephalopathy based on the analysis of mean arterial pressures and the locations of brain edema. Before reaching that level of high arterial pressure, however, posterior supratentorial regions also appear to be involved and should be demonstrated as abnormal on MR images. To our knowledge, there is no clear explanation for the prominence of brain stem changes compared with the other brain territories, especially in occipital lobes.
Schwartz et al (6) reported that DWI was reliable in distinguishing vasogenic edema in hypertensive encephalopathy from cytotoxic edema in the setting of cerebral ischemia, because increased diffusion was observed in the reversible occipital lesions. Moreover, it was similarly reported that increased diffusion was observed in reversible lesions in eclampsia/pre-eclampsia (18), cyclosporin-A neurotoxicity (19), and tacrolimus neurotoxicity (20), that is, the so-called posterior reversible encephalopathy syndrome(PRES), whereas decreased diffusion was seen in irreversible lesions in cases of complicated PRES (18, 20). On the basis of these findings, an increased ADC in brain stem lesions would reasonably be expected in reversible brain stem hypertensive encephalopathy, as in our case.
To the best of our knowledge, only a single case of brain stem hypertensive encephalopathy quantitatively evaluated by DWI has been reported (15). According to that report, the patient showed a high ADC (suggestive of vasogenic edema) on the left side of the pons and a low ADC (suggestive of cytotoxic edema) on the right side, and her clinical symptom of left hemiparesis appeared to correspond to the low ADC in the right side of the pons. In our case, the ADC was elevated in all of the lesions, which suggests that they all represented vasogenic edema and the patient might therefore have presented with no weakness of the extremities. These findings suggest that DWI may be helpful in predicting the reversibility or irreversibility of affected tissues and the clinical outcome in patients with brain stem hypertensive encephalopathy.
We used LSDWI to quantify diffusion in the lesions in a patient with brain stem hypertensive encephalopathy. Compared with echo-planar DWI, LSDWI is superior for imaging structures in the posterior fossa such as the brain stem because it is inherently less sensitive to magnetic susceptibility artifacts (9, 10). Thus, LSDWI is judged to be more suitable for the evaluation of diffusion in brain stem lesions.
If the lesions are limited to the brain stem, the differential diagnosis based on MR imaging findings includes glioma, acute infarction, osmotic myelinolysis, encephalitis, and vasculitis such as neuro-Behçet’s disease. Among these conditions, the identification of acute infarction is especially critical in an emergent clinical setting. Clinical symptoms are generally mild in brain stem hypertensive encephalopathy, such as mild headache, gait unsteadiness, drowsiness, and mild hemiparesis, even when the entire brain stem shows swelling and abnormal signal intensities at MR imaging (12–16). Therefore, such marked “clinicoradiologic dissociation” may rule out major brain stem infarction. On the other hand, it is possible that the patient may present coma with hypoattenuation throughout the brain stem observed at CT, leading to a clinical diagnosis of catastrophic brain stem infarction. Even in these patients, if ADC maps confirm vasogenic edema, clinical recovery can be expected with appropriate treatment (8). Thus, quantitative diffusion assessment may contribute greatly to reaching the correct diagnosis and instituting appropriate treatment without delay.
References
- Received August 24, 2003.
- Accepted after revision September 22, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}