
Abstract
SUMMARY: We present a case of Klippel-Feil syndrome and Sprengel deformity with a bovine aortic arch and an aberrant course of the left subclavian artery in a 14-year-old boy. CT and MR imaging of the neck and upper thorax demonstrated a cervical osseous segmentation anomaly, a left common carotid artery originating from the innominate artery, and a left subclavian artery coursing through the intraspinal space at the C6 through T1 level. Possible embryonic mechanisms and clinical significance of this variant are reviewed.
Klippel-Feil syndrome (KFS) is a heterogeneous entity that includes a large vascular variability. Exact evaluation of supra-aortic vessels before orthopedic correction has, therefore, been strongly recommended. Sprengel deformity (SD) has been readily associated with KFS, and both anomalies share many developmental and embryologic steps. In this setting, abnormal development of the fetal aortic arch and the vertebral or subclavian artery or both has been implicated as a causative factor in both syndromes. Nevertheless, an association between KFS, SD, and an aberrant intraspinal course of the left subclavian artery has, to the best of our knowledge, never been described. This variation, if not duly recognized, may have devastating consequences during surgery. Chronic intraspinal pulsation of this vessel, on the other hand, may eventually lead to myelopathic changes due to its proximity to the cervical spinal cord.
Case Report
A 14-year-old boy with known KFS clinically presented with repetitive episodes of severe occipital headache, vertigo, and nausea combined with neck and shoulder discomfort, which lasted for weeks. Clinical examination showed a markedly reduced vertebral range of motion. An SD and fusion of the left ribs 1–3 were known. Sonography demonstrated a prominent right vertebral artery without stenosis. Blood pressure was normal. Contrast-enhanced CT of the head, neck, and upper thorax was performed to exclude cranial abnormalities and cervical fracture.
Findings of cranial CT were normal. Fusion of the left side of the odontoid process and the lateral mass of C2 with the lateral mass of C1 and a bifid anterior and posterior C1 arch were noted. Multisegmental left-sided hemivertebral fusions were present at the levels C5 through T3 with a bifid spinous process, which led to a right-sided cervicothoracic angulation and scoliosis.
Vessel status revealed a so-called bovine aortic arch variant. The first branch of the aortic arch was a common trunk, comprising the innominate artery and the left common carotid artery (Fig 1A). The second branch was the left subclavian artery. The first segment of this vessel showed a posterior course, entering the spinal canal at T1 (Fig 1A, -B) with a horizontal course through the left epidural space, exiting posteriorly through an osseous defect of the left posterior arch at the same level (Fig 2A, -B) before resuming its normal trajectory within the supraclavicular space. The left vertebral artery originated from the left subclavian artery just before its intraspinal penetrance and showed a normal cranial continuation after entering the left transverse foramen at the level of C6. The U-shaped loop of the subclavian artery due to its intraspinal course was clearly depicted. There was no spinal canal stenosis or displacement of the cervical cord (Fig 2B). On a follow-up MR imaging, vascular anomalies were confirmed but the spinal cord itself revealed no signal-intensity anomaly, hemorrhagic changes, or evidence of myelopathy.

A and B, Volume rendering reconstructions with anteroposterior view (A) and left-lateral view (B) showing a bovine aortic arch variant (white arrow) and a U-shaped dorsal running loop of the left subclavian artery. The posterior course of the proximal part of the left subclavian artery entering the intraspinal space through the left-sided fused vertebrae at the T1 level with the same-level dorsal exiting is clearly seen.
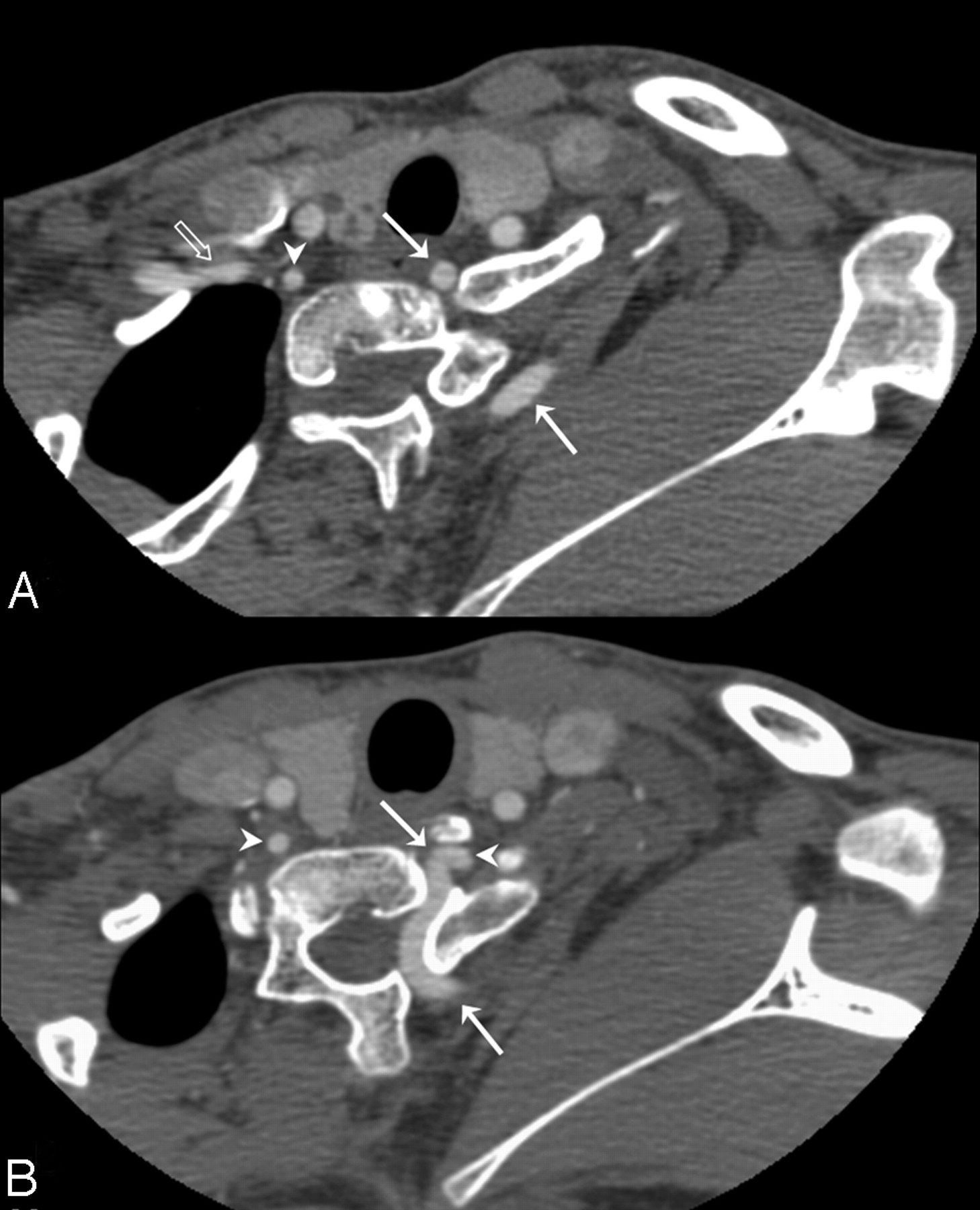
A and B, Axial multisection CT reference images. Arrowheads point to the vertebral artery of the right and left side. The transparent arrow shows the right subclavian artery. A, Anterior and posterior part of the left subclavian artery (white arrows). B, Origin of the left vertebral artery (white arrowheads) contralateral to the normal course of the right vertebral artery.
Discussion
In 1912, Maurice Klippel and Andre Feil first described a patient presenting an association of short neck, low posterior hairline, and limited range of motion. The complete clinical triad is seen in <50% of the cases, and many patients with KFS demonstrate additional developmental anomalies. Therefore, KFS is diagnosed by the presence of 2 or more nonsegmented cervical vertebrae alone.1
KFS is reported to be present in 1 of 42,000 individuals, and 57%–70% of all patients are female. Various classification schemes were developed. KFS was classically categorized into 3 groups, depending on the level and extent of vertebral fusion. Genetic analysis revealed an autosomal recessive trait for types I and III and an autosomal dominant trait for type II. Subsequent studies incorporated the mode of inheritance with the location of the most rostral vertebral fusion. This system includes 4 groups with different autosomal dominant or recessive or X-linked traits.
Anomalies of the aortic arch, carotid arteries, subclavian artery, vertebral artery, and a persistent trigeminal artery are known in association with KFS.2–6
SD has been found in 7%–42% of the patients with KFS. The scapula develops from the paraxial mesoderm and is, therefore, closely associated with the development of the cervical spine. Patients with KFS and SD show more congenital fused segments, especially at the C6 through C7 level.7
Cervical spine development starts with gastrulation in the fourteenth week by formation of the 3 germ cell layers and the notochord. Between days 20–30, the paraxial mesoderm subdivides into somites, which divide into sclerotomes and dermomyotomes. Sclerotomes resegment into a cranial and a caudal area, and in between forms the intervertebral disk. Fusion of the caudal section from a rostral somite with the cranial section of the corresponding caudal somite forms a vertebral body. Errors in segmentation may result in KFS. Vascular system development runs parallel to the development of the spinal cord. At days 21–29, thirty pairs of dorsal intersegmental arteries arise from the dorsal aortae and supply their corresponding somites. Between days 32–42, vertical and right-angle anastomoses develop between them and cross the vertebral bodies. The anastomoses serve as the origin of the vertebral arteries. During gestational days 37–42, the first 6 cervical intersegmental arteries regress, and only the seventh intersegmental arteries persist. The entire left and the greater part of the right subclavian artery originate from this seventh intersegmental artery.
Fetal vascular disruption disorders have been found to be responsible for various congenital anomalies, depending on the extent and timing of the disruptive event. A subclavian artery supply disruption sequence has been hypothesized to result in KFS on the basis of the theory that vascular disruption of the vertebral artery leads to ischemia during morphogenesis. Subsequent structural anomalies will involve not only the definitive vascular pattern by itself but also the vasculature-dependent soft-tissue territories.8,9 Due to the heterogeneity in KFS, the exact influence of vascular and genetic factors remains unclear. Because of the complex vascular variants in this group of patients, prior imaging of the aortic arch and supra-aortic vessels is recommended.10
References
- Received October 3, 2007.
- Accepted after revision October 12, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.