
Abstract
BACKGROUND AND PURPOSE: Focal point tenderness over the fractured level is believed to be a necessary criterion for performing vertebroplasty. The purpose of this study was to explore whether the presence of focal-point tenderness over a fracture treated with vertebroplasty predicts superior clinical outcome as compared with outcomes in patients without such tenderness.
MATERIALS AND METHODS: In this retrospective study, we divided patients into 3 groups on the basis of pain patterns noted during history and physical examination before an initial vertebroplasty in 534 consecutive patients. Group 1 comprised 373 (70%) of 534 patients with focal-point tenderness over the treated fractures. Group 2 comprised 119 (22%) patients with focal-point tenderness over the treated fractures as well as subjective off-midline pain or focal tenderness to palpation over nontreated vertebrae. Group 3 comprised 42 (8%) patients without focal-point tenderness over the treated fractures but with subjective off-midline pain or tenderness to palpation over nontreated vertebrae. Outcomes included pain at rest and with activity as well as the Roland-Morris Disability Questionnaire score. Statistical tools included the 2-tailed t test with a Bonferroni adjustment.
RESULTS: Baseline pain at rest and with activity was not different among groups, but the proportion of group 3 patients maintained on a narcotic anesthesia preprocedure was less than that of groups 1 and 2 (P = .02 compared with both groups). Group 3 achieved significantly lower pain scores at rest at 1 month (P < .0001 compared with group 1 and P < .001 compared with group 2).
CONCLUSION: The presence of focal-point tenderness does not predict superior clinical response following vertebroplasty compared with the absence of focal tenderness. Even patients without focal tenderness may benefit from vertebroplasty.
Vertebroplasty has been widely accepted as an effective treatment for vertebral compression fractures that produce pain resistant to medical therapy. The clinical criteria for selecting patients for vertebroplasty include a suggestion that the fracture represents the prime generator responsible for the refractory pain. The specific clinical criteria used to identify whether a particular fracture is the prime pain generator are poorly described in the vertebroplasty literature. Many case series simply state that the treated levels were selected because they were causing pain, without further description of how a painful fracture is identified by using clinical criteria.1-5 Some publications, including a consensus statement,6-11 report that focal tenderness to palpation is an important or necessary clinical finding in selecting patients for vertebroplasty, but the data to support such a recommendation remain sparse.
Previous publications have suggested that even patients without focal tenderness may benefit from vertebroplasty. Gaughen et al,12 in a small series of patients, noted good pain relief in patients without localizing pain. Gibson et al,13 in a larger series of patients, noted good outcomes in most of patients who had pain distant from the treated level or levels. However, this latter publication did not indicate whether focal tenderness was present in these patients in addition to the nonlocalizing pain pattern.
In this study, we offer additional data regarding the value of focal tenderness as a predictor of outcome following vertebroplasty. We compare patients, with and without localizing tenderness, regarding baseline and postprocedural pain severity and functional status to determine whether such localizing pain predicts response following vertebroplasty.
Materials and Methods
This retrospective study was performed in all patients undergoing vertebroplasty between February 1999 and March 2007 at our tertiary care institution. Institutional review board approval was granted for the study. Our group has previously published retrospective reviews of these same patients, but we have never previously evaluated the pattern of pain localization in this cohort.14-28 Preprocedural evaluation, including plain radiographs, MR imaging, bone scans, and physical examination, was performed to determine patients eligible for undergoing vertebroplasty. Our practice includes 6 experienced practitioners, and we do not and have not had a rigorous standardized algorithm for the clinical assessment of patients presenting for potential vertebroplasty. For the purpose of this study, we define “localizing tenderness on palpation” to include patients who reported pain when the examiner pressed over the spinous process of the suggested fractured vertebral body. These clinical assessments were usually performed by experienced vertebroplasty practitioners, both in the office with the patient in the sitting or standing position, or in the prone position using fluoroscopic guidance. Other clinical criteria used in varying ways by different practitioners in our practice included the presence of subjective pain as well as other pain patterns. For some practitioners in our practice, the lack of focal tenderness was considered an exclusion for vertebroplasty. We also relied on imaging heavily, with signal-intensity changes of marrow edema or increased activity on MR imaging and bone scanning,29 respectively, considered predictors of good response following vertebroplasty.
We have previously reported our vertebroplasty technique in this same patient cohort.27
Routine follow-up in our center was performed with physical examination by a neuroradiologist within 2 hours postprocedure and over the phone by experienced nurses at 1 week, 1 month, 6 months, 1 year, and 2 years following the procedure. Pain score at rest and with activity, (1–10), subjective pain score (worse to completely resolved), and Roland-Morris Disability Questionnaire score were measured at each follow-up point.
We reviewed reports of preprocedural physical examination and categorized the patients to 3 groups:
group 1: patients with focal-point tenderness only at the treated vertebrae, without subjective pain separate from the treated vertebrae;
group 2: patients with both focal tenderness over the treated levels as well as off-midline, subjective pain or focal tenderness over nontreated or nonfractured vertebrae;
group 3: patients without focal-point tenderness over the treated levels, but with off-midline pain or with pain over nontreated or nonfractured vertebrae.
We also determined the relative proportion of groups on an annual basis, to explore whether our practice patterns regarding patient selection changed with time.
Statistical Analysis
A 2-tailed t test was performed to evaluate the differences in pre- and postprocedural pain scores (1–10) at rest and with activity, and the Roland- Morris Disability Scale. A χ2 test was performed to compare the difference in the proportion of patients treated with narcotic medication prior to the procedure among groups. As we included 15 comparisons in pain scores among groups over time, the P value (.05) was adjusted on the Bonferroni method so that P values < .003 were considered significant.
Results
Seven hundred ninety-one procedures were performed on 656 (women, 67%) patients and 1191 levels between February 1999 and March 2007. The median age of patients was 76 years (range, 31–97). Because we included only the first vertebroplasty procedure of all patients, 134 (17%) procedures were excluded. One hundred twenty-two of 656 (19%) patients were excluded because no data were available regarding preprocedure physical examination findings, so our study group contained 534 patients. Patient demographics, preprocedural imaging examinations, baseline pain and Roland-Morris scores, and narcotic usage are shown in the Table. There were no differences among groups regarding the proportion of female patients, age, baseline pain at rest or with activity, or baseline Roland-Morris scores. A significantly lower fraction of patients in group 3 were maintained preprocedurally on narcotic medication compared with the other 2 groups (χ2, P = .02 compared with groups 1 and 2).
Baseline characteristics of groups
With time, group 3 patients composed an increasing proportion of patients treated at our center, increasing from 3% to 7% of patients from 1999 to 2007 (Fig 1).

Graph shows increasing vertebroplasties in patients without focal-point tenderness in our center. Asterisk indicates that data are from 2007, with patients included up to the end of February; Preop, preoperative.
Clinical Outcomes
All 3 groups demonstrated significant improvement in all outcome measures following vertebroplasty compared with baseline values as we have noted in a previous publication that included many of the same patients studied here.17 Outcome measures within any individual group were not different across time.
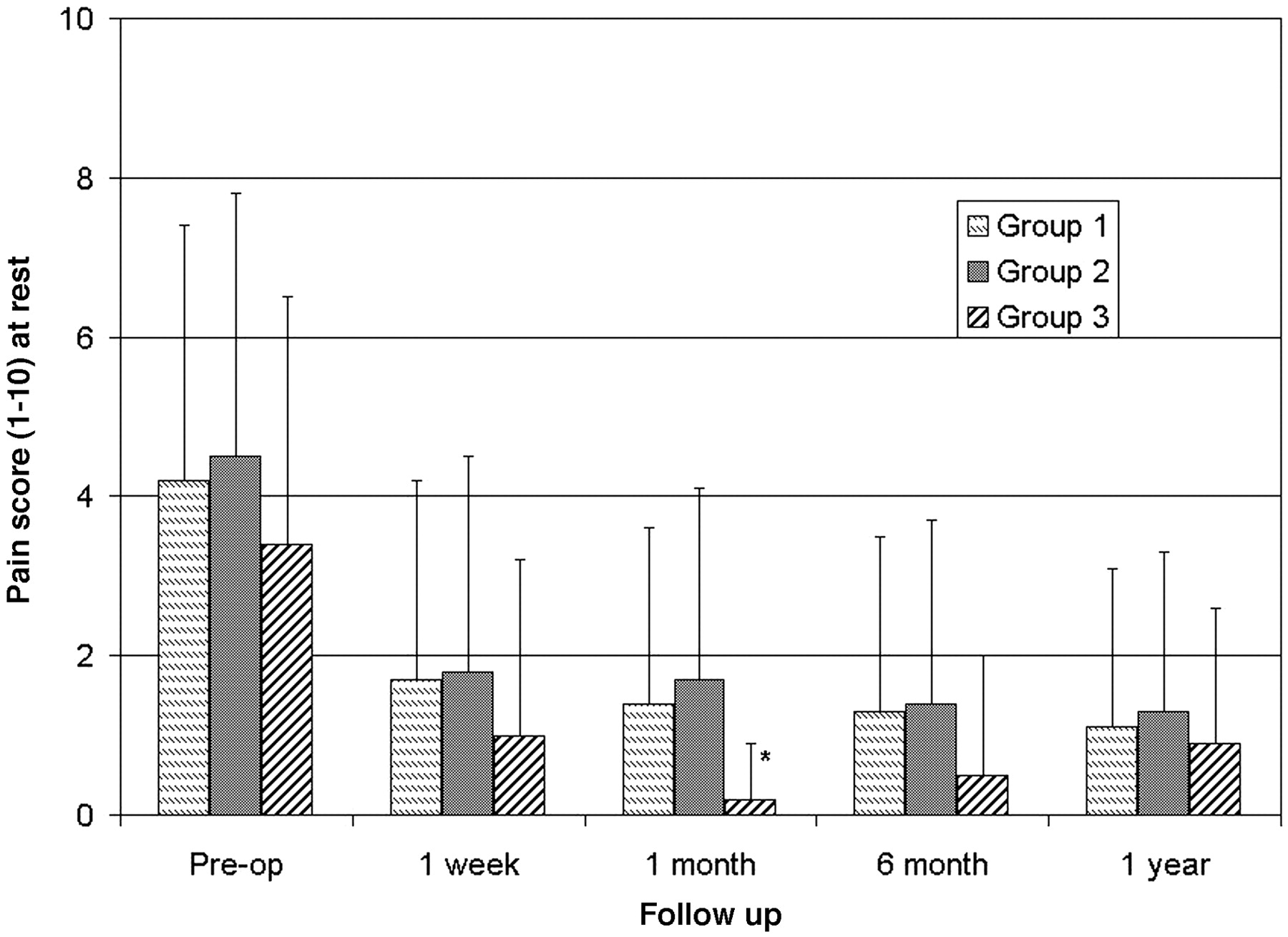
Compared with groups 1 and 2, group 3 demonstrated a lower severity of pain at rest at 1 month (P < .0001 and P < .001, respectively). There were no other significant differences among groups (Figs 2–⇓4).
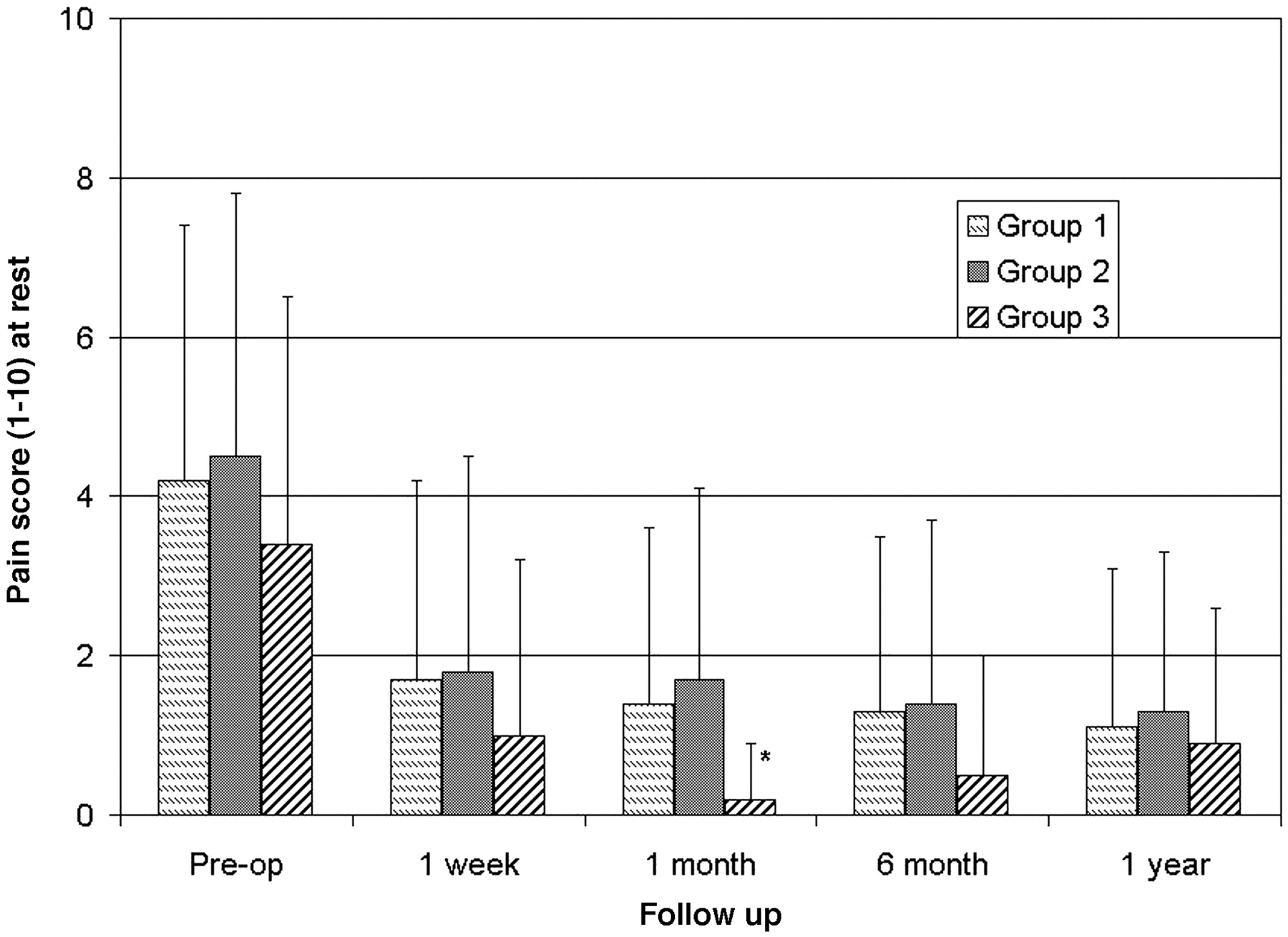
Graph shows pain score (1–10) at rest. Asterisk indicates significant difference compared with groups 1 and 2 (P = .0001 and .001, respectively); Preop, preoperative.

Graph shows pain score (1–10) with activity.

Graph shows modified Roland-Morris Disability Questionnarie (0–23) score.
Discussion
In this retrospective review, we assessed the impact of preprocedural pain patterns on outcomes following vertebroplasty. Although we are unclear about the sign's relevance to patient selection, the physical finding of tenderness to palpation over a fracture's spinous process occupies a prominent place in triaging patients to or from vertebroplasty. Do reported focal point tenderness as a requirement for selecting patients to undergo vertebroplasty.30 Amar et al31 excluded the patients for vertebroplasty who failed to localize tenderness on the fractured level. Indeed, in our own practice, most patients selected for the procedure demonstrated such tenderness over the fractured vertebra, which correlated with preoperative imaging.
The current study indicates that patients in our practice selected for vertebroplasty without focal tenderness actually had better outcomes than patients with focal tenderness, even though baseline pain and Roland-Morris scores were similar among groups. The improved clinical outcome for patients without focal tenderness as compared with patients with such tenderness does not, in our opinion, prove that vertebroplasty is necessarily superior if focal tenderness is absent. Rather, these patients may represent a separate and distinct group in which multiple factors are at work in predicting clinical outcome. Given the retrospective nature of this study, it is difficult or impossible to address potential differences in patient groups, beyond the severity of baseline parameters. However, our findings suggest that tenderness to palpation is not a necessary criterion for performing vertebroplasty.
Previous authors have evaluated the impact of pain patterns on outcomes following vertebroplasty. Gibson et al13 reported an overall 83% improvement of nonmidline pain in 240 patients postvertebroplasty. However, these authors did not report whether these same patients also had focal tenderness to palpation. Thus, our current study adds additional information about the specific patterns of tenderness and their prognostic value.
Gaughen et al12 described a group of 100 patients, including 10 patients without point tenderness on physical examination at the time of vertebroplasty evaluation. In postvertebroplasty follow-up, they found 100% pain improvement in 9 available patients without preoperative focal-point tenderness. The authors failed to demonstrate a significant difference between the 2 groups in pain improvement after the procedure but suggested that physical examination findings may be of dubious value in patient selection.
On the basis of the current series alone, we are unable to evaluate the relative impact of various selection criteria for vertebroplasty. Most of our patients had MR imaging or bone scanning findings suggesting ongoing healing, irrespective of physical examination findings. It may be that imaging studies are the most accurate tool for patient selection. For example, Maynard et al29 demonstrated the predictive role of bone scanning in clinical response to vertebroplasty. However, we are aware of no prospective studies focused on the utility of routine MR imaging in triaging patients to vertebroplasty. As such, we believe that further study of the use of MR imaging in vertebroplasty is warranted.
In this current patient series, there were relatively few patients without localizing tenderness as compared with patients with localizing tenderness. This pattern simply reflects our clinical practice, in which the presence of localizing tenderness has been considered by some of our group to be an essential component for patient selection. Undoubtedly, this practice pattern has introduced bias into this study, but its retrospective nature prohibits exploration of potential bias. In addition, we used no standard protocol describing how firmly one should push on the spine during the examination. It remains likely that insufficient pressure would diminish sensitivity, whereas overexuberant pressure would enhance sensitivity of the clinical sign. Furthermore, we perform the examination with the patient in either the upright or prone position, without using other positions such the decubitus position. Some investigators believe that examination in the decubitus position represents the ideal technique for this type of physical examination (personal communication, Sander P.D. Dijkstra, MD, PhD, Leiden University Medical Center, the Netherlands, March 2008).
Conclusion
Patients without focal-point tenderness over the treated fractures in preprocedural evaluations showed significant pain improvement, in some cases even superior to that in patients with such tenderness. The presence of focal-point tenderness does not predict superior clinical response following vertebroplasty compared with the absence of focal tenderness.
References
- Received March 26, 2008.
- Accepted after revision April 28, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Effect of Systemic Therapies on Outcomes following Vertebroplasty among Patients with Multiple Myeloma
- Is Severe Pain Immediately after Spinal Augmentation a Predictor of Long-Term Outcomes?
- Asymptomatic and Unrecognized Cement Pulmonary Embolism Commonly Occurs with Vertebroplasty
- Clinical Outcomes with Hemivertebral Filling during Percutaneous Vertebroplasty
- Efficacy of Percutaneous Vertebroplasty for Multiple Synchronous and Metachronous Vertebral Compression Fractures
- Urinary Tract Infections in the Potential Vertebroplasty Patient: Incidence, Significance, and Management
- Vertebroplasty for the Treatment of Traumatic Nonosteoporotic Compression Fractures