
Abstract
BACKGROUND AND PURPOSE: Myelin instability and citrullinated myelin basic protein have been demonstrated in the brains of patients with chronic and fulminating forms of multiple sclerosis (MS). Our aim was to trace citrulline in the brains of patients with early-onset MS by using proton MR spectroscopy (1H-MR spectroscopy).
MATERIALS AND METHODS: A short-echo single-voxel 1H-MR spectroscopy by using the point-resolved proton spectroscopy sequence was performed in 27 patients with MS and 23 healthy subjects. Voxels of interest were chronic demyelinating lesions (CDLs, n = 25) and normal-appearing white matter (NAWM, n = 25) on T2-weighted imaging, and when available in patients with MS, enhancing demyelinating lesions (EDLs, n = 8). Frontal white matter (WM) was studied in control subjects. N-acetylaspartate, choline, and myo-inositol (mIns)-creatine (Cr) ratios and the presence of a citrulline peak were noted.
RESULTS: Citrulline peaks were more frequently observed in patients with MS than in control subjects (P = .035), located in the NAWM in 8/25 (32%), in CDLs in 7/25 (28%), and in EDLs of 1/8 (12.5%) patients with MS. The presence of citrulline and measured metabolite/Cr ratios was not related to age at imaging, age at disease onset, duration of disease, or number of relapses. There was no significant metabolic difference between the NAWM of patients with MS and the WM of the control subjects. mIns/Cr was significantly greater in CDLs compared with the NAWM of patients with MS and the WM of healthy subjects.
CONCLUSIONS: Citrulline was more frequently identified in the brains of patients with early-onset MS than in healthy subjects by 1H-MR spectroscopy, suggesting an association of increased citrullination of myelin proteins with demyelinating diseases.
The pathogenesis of multiple sclerosis (MS) involves immunologic mechanisms resulting from a genetic predisposition or environmental influences. Inherent properties of myelin might contribute to the pathogenesis of MS.1,2 Myelin basic protein (MBP) is the second most abundant myelin protein in the central nervous system (CNS), after proteolipid protein, and the only essential structural protein for the formation of myelin: It is accepted as the “executive molecule of myelin.”3 As a posttranslational modification, it causes conversion of arginine to citrulline through the release of ammonia (deimination/citrullination). Increased citrullination of MBP diminishes its ability to organize lipid bilayers into compact multilayers, creates a more open structure to proteases such as cathepsin D, and thus results in myelin instability.4 Citrullinated MBP was reported to be increased threefold in MBP isolated from MS brain and six- or sevenfold in fulminating forms such as Marburg disease.5,6 Thus deimination/citrullination has been suggested to predispose the white matter (WM) to demyelinating diseases.
We previously investigated the presence of citrulline in patients with acute disseminated encephalomyelitis (ADEM) by using proton MR spectroscopy (1H-MR spectroscopy) and observed it more frequently than in age-matched controls.7 Because, to our knowledge, this issue has not been examined in MS by imaging, we aimed to determine citrulline in patients with early-onset MS compared with healthy subjects by using 1H-MR spectroscopy. We also examined MR spectroscopic findings of the normal-appearing white matter (NAWM) and demyelinating lesions in this particular group of patients with MS.
Materials and Methods
This was a multicenter study of child neurology departments recruiting 27 patients younger than 19 years of age who received the diagnosis of relapsing-remitting MS by clinical and MR imaging features. Approval of the institutional review board and consent from all patients were obtained.
None of the patients were in acute clinical relapse at the time of imaging, but patients 2 and 12 had relapses 4 and 9 weeks following radiologic examination, respectively, and patient 14 had a relapse 3 weeks before the study.
Control subjects were patients examined for the clinical diagnosis of headache or syncope (n = 23) who had normal findings on neurologic examination, electroencephalography, and conventional brain MR imaging.
MR imaging was performed on a 1.5T unit (Symphony; Siemens, Erlangen, Germany) by using a standard quadrature head coil. Initially T2-weighted fast spin-echo images (TR/TE, 4000/100 ms; matrix, 448 × 88) in all 3 orthogonal planes and T1-weighted axial acquisitions at 5 minutes following intravenous administration of gadolinium-based contrast agent (0.01-mmol/kg meglumine-gadoterat, Dotarem; Guerbet, Aulnay-sous-Bois, France) were performed for 2 reasons: 1) to exclude any associated finding of a nondemyelinating disease, and 2) to evaluate the chronic demyelinating lesions (CDLs), enhancing demyelinating lesions (EDLs), and normal WM for further decisions regarding voxel positioning in 1H-MR spectroscopy. All these sequences consisted of 20 sections with 5-mm thickness and 0.5-mm intersection gap.
Following on-site evaluation of these conventional images, dedicated radiologists (K.K.O., A.O.A.) performed 1H-MR spectroscopy. Lesion size, presence of perilesional edema, contrast enhancement, and location of the lesion were the investigators’ concerns during the voxel positioning. 1H-MR spectroscopy was performed routinely in the following 3 regions in all patients when available: a nonenhancing lesion with no surrounding edema (regarded as a CDL), WM without T2 hyperintensity (NAWM), and an EDL (as an acute demyelinating lesion). Because the parietal periventricular WM might contain immature myelin up to early adulthood in healthy individuals, special attention was paid for voxel assignment in the frontal lobe. If 1 or more areas of interest were present in another site, then the voxel of interest (VOI) was placed in the extrafrontal parenchyma. All previous MR imaging examinations of the patients were evaluated by radiologists to verify that selected NAWM was never affected radiologically. For patients who had an enhancing demyelinating lesion, a second shimming was performed before MR spectroscopy of the enhancing lesions.
1H-MR spectroscopy applied a short-echo single voxel study (svs) by using a point-resolved proton spectroscopy sequence (PRESS) from all available regions described above in all patients with MS (TR, 1500; TE, 30 ms; voxel size, 15 × 15 × 15 mm3; 192 scan averages). NAWM was chosen from the contralateral hemisphere, in a comparative region of the lesion of interest. Patients with no lesions and control subjects had only 1 svs imaging in the frontal WM.
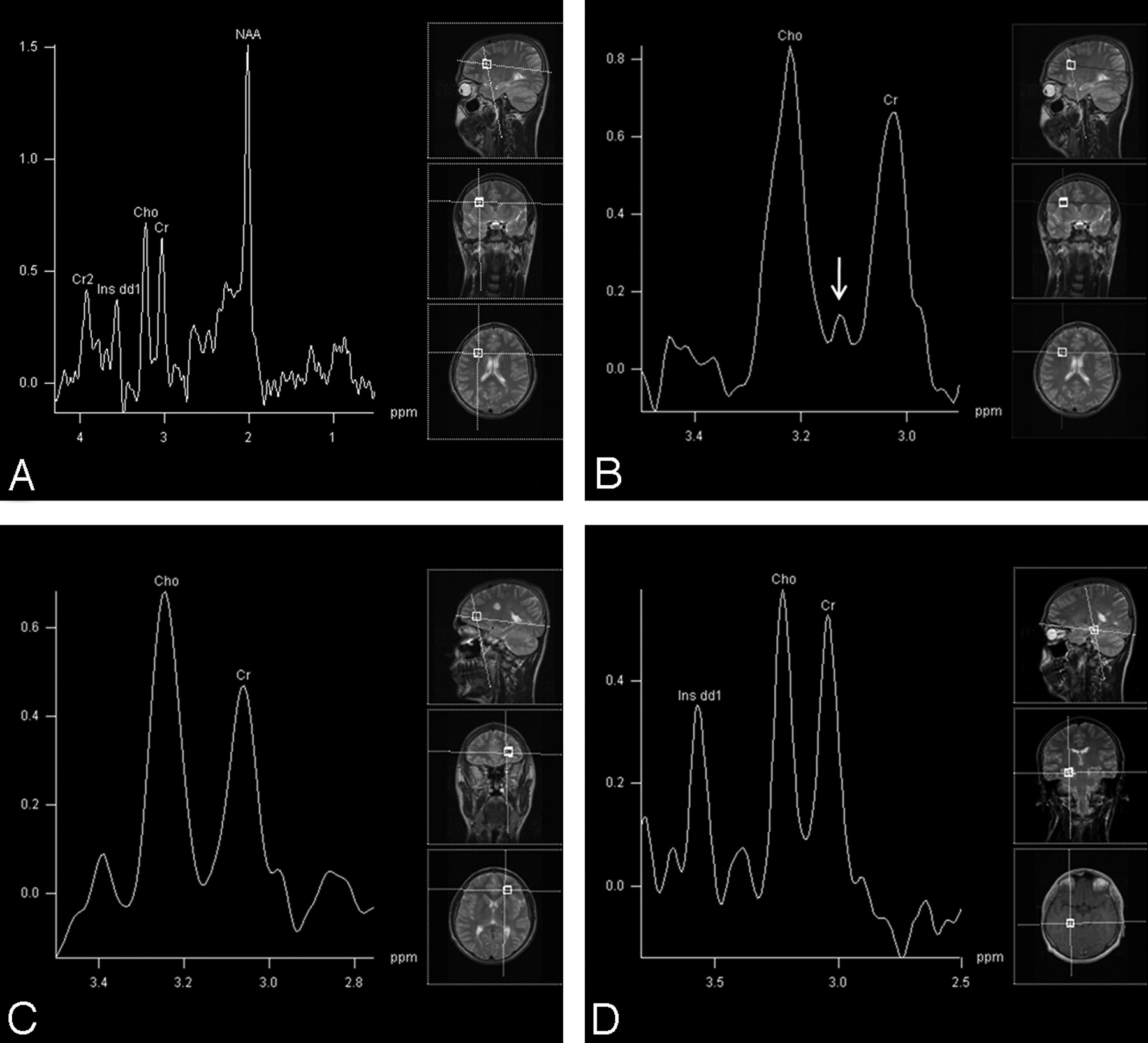
On completion of data acquisition, resonance peaks of N-acetylaspartate (NAA), choline (Cho), creatine (Cr), and myo-inositol (mIns) were identified and ratios of NAA-, Cho-, and mIns-Cr were computed by using an automated postprocessing software provided by the manufacturer on an off-line workstation (Leonardo Systems, Siemens). The citrulline peak was defined at 3.15 ppm between Cho and Cr peaks as described previously.7,8 The presence of the citrulline peak was searched by augmenting the zone between the Cho and Cr peaks through spectral narrowing between 2.75 and 3.5 ppm on the automated software (Fig. 1A, -B). Because just the documented spectral range was changed by the user on the software provided by the MR imaging manufacturer, this process did not require any additional calculation of the resonances. When a differentiation between a peak and noise was equivocal, it was accepted as “peak negative.”
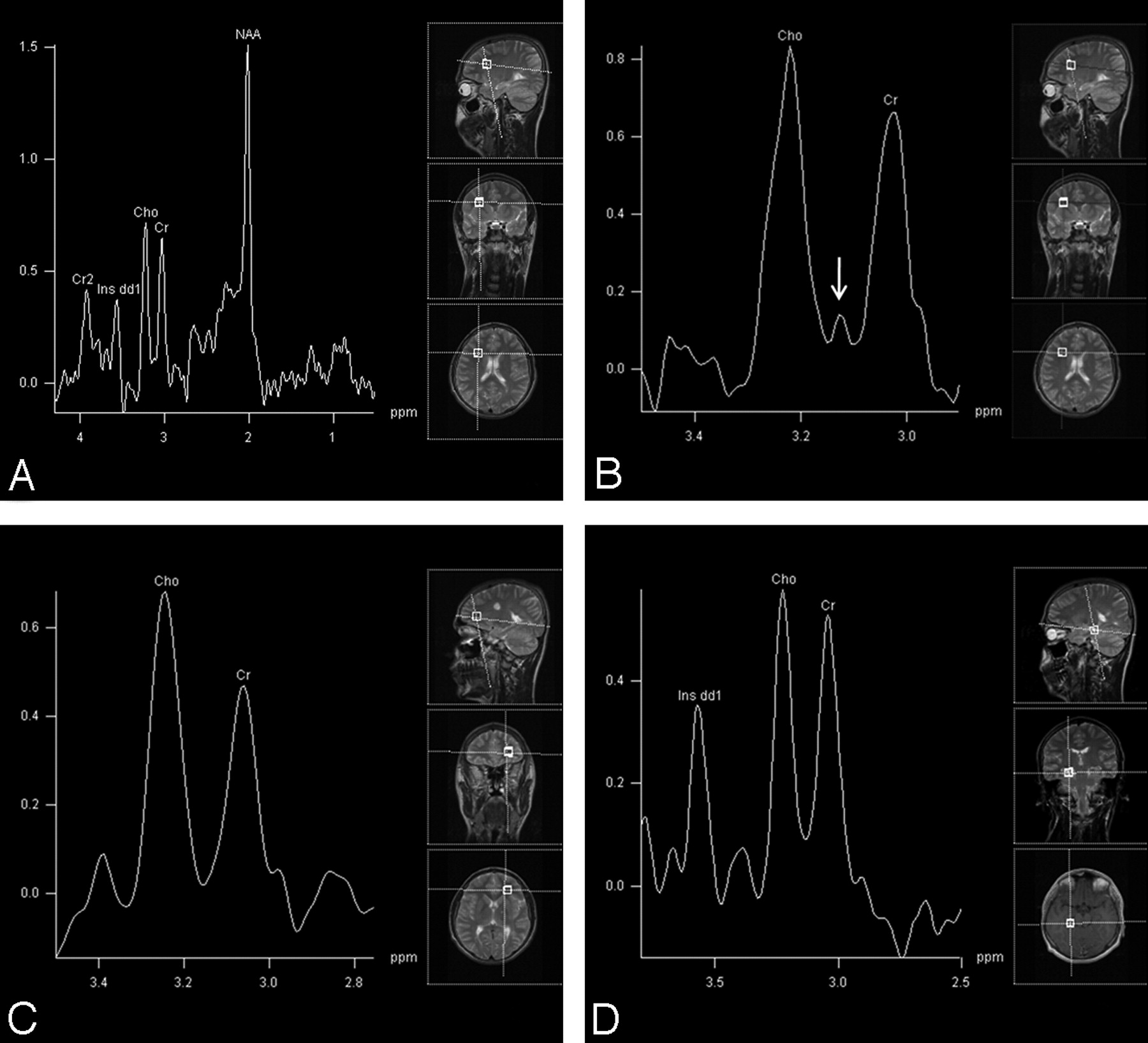
Patient 12. A, Short-echo single-voxel 1H-MR spectroscopy (PRESS; TR, 1500 ms; TE, 30 ms; voxel size, 15 × 15 × 15 mm3) obtained from a right frontal CDL. B, Spectral narrowing with a resultant augmentation between 2.75 and 3.5 ppm shows the citrulline peak (arrow) between Cho and Cr peaks. C and D, No citrulline peak is present in the left frontal NAWM (C) and in the right temporal EDL (D).
Statistical analysis was done by using the following: independent-samples t test, paired-samples t test, χ2 test, Mann Whitney U test, and the Pearson correlation analysis.
Results
Twenty-seven patients with MS and 23 healthy subjects were included in the study. The groups were similar in age (4–22 years; mean, 14.7 ± 4.9 years for MS; and 5–23 years for healthy subjects; mean, 13.4 ± 3.8 for the control group; independent-samples t test, P = .31) and sex (F/M ratio 16/11 in MS and 10/13 in the control groups; χ2 test, P = .407). The mean age at disease onset in patients with MS was 12 years; the mean number of relapses following the diagnosis of MS, 3; and the mean duration of disease, 39 months.
The presence and distribution of the citrulline peak according to the VOI site revealed by 1H-MR spectroscopy in patients with MS are documented in Table 1.
Presence and distribution of the citrulline peak in patients with MS according to the VOI site revealed by 1H-MR Spectroscopy
Of 27 patients, NAWM could be evaluated in 25, and CDL or EDL could be examined in 25 because 2 patients (patients 2 and 3) had no definable WM free of T2-weighted hyperintense lesions and 2 other patients (patients 5 and 17) had no visible MR imaging lesion. Eight patients had acute demyelinating lesions demonstrating gadolinium enhancement (EDL).
A total of 12/27 (44,4%) patients with MS and 3/23 (13%) control subjects revealed a citrulline peak on MR spectroscopy (P = .035) (Figs 1 and 2). The citrulline peak was observed in the NAWM of 8/25 (32%) and in the CDLs of 7/25 (28%) patients with MS. It appeared only in the NAWM in 4, only in CDL in 3, and in both CDL and NAWM in 4 patients with MS. The unique patient with a citrulline-positive EDL (patient 10) showed no citrulline peak in other regions. When other acute relapses were considered, a citrulline peak was identified in the CDL in 1 patient (patient 12), who had a relapse 9 weeks after imaging, but not in patient 2, who relapsed 4 weeks later, or in patient 14, who had a recent relapse 3 weeks before imaging.
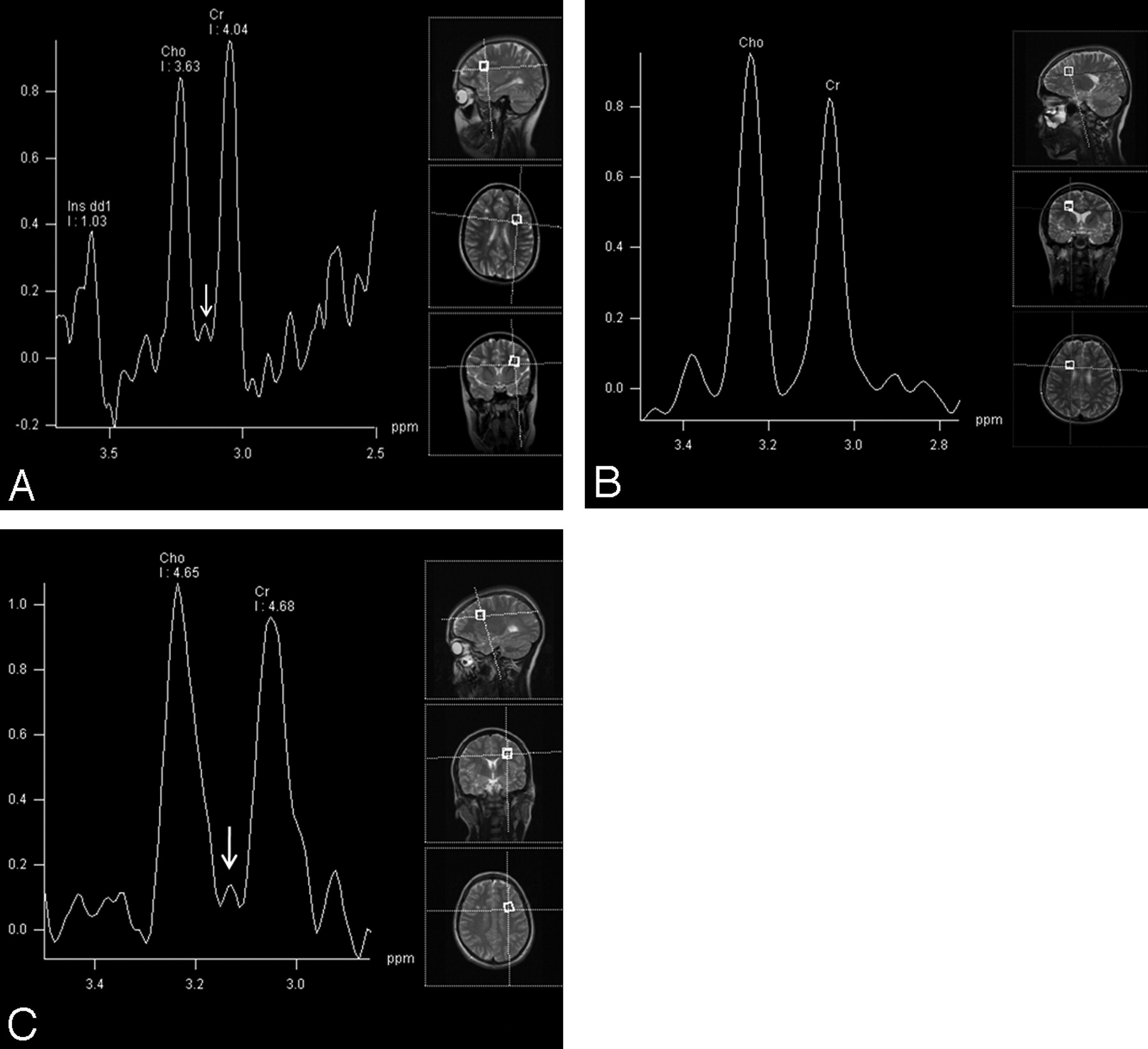
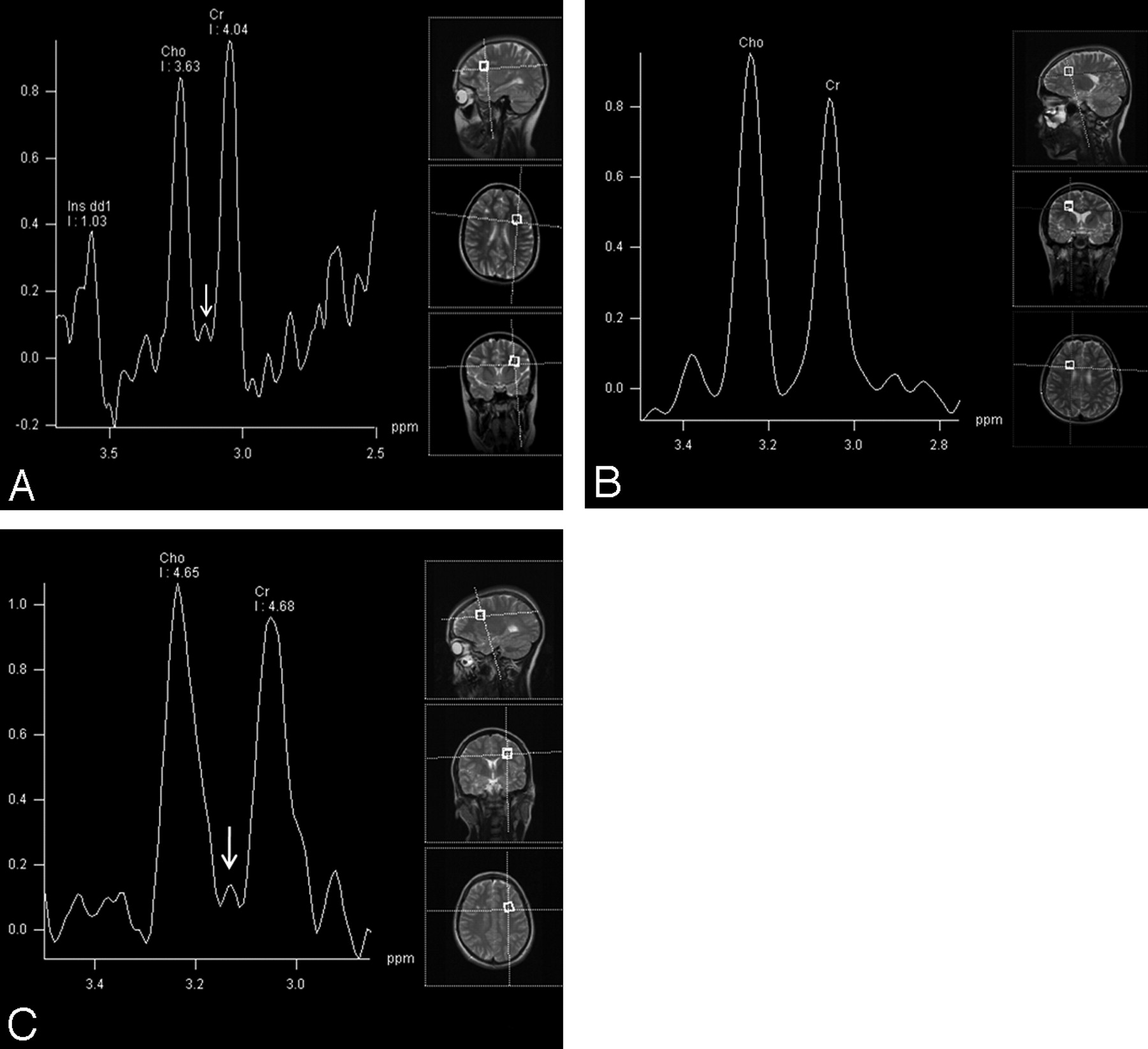
A and B, Patient 4. A small citrulline peak (arrow) is shown between Cho and Cr peaks (A) in a voxel obtained from the left frontal NAWM, whereas it is absent in the voxel from the right frontal lesion (B) on short-echo 1H-MR spectroscopy. C, Patient 1. The voxel from the left NAWM again shows a citrulline peak (arrow).
Three control subjects with a citrulline peak on MR spectroscopy were 17, 10, and 23 years old and had undergone MR imaging because of headache and syncope without accompanying neurologic signs and symptoms. No other neurologic complaints developed during the 6-month follow-up period after imaging.
Citrulline-positive and -negative patients with MS were similar in age at imaging, age at onset, duration of disease, and number of relapses since diagnosis (Mann Whitney U test; P = .375, .214, .907, .and .718, respectively).
Results of statistical analysis of NAA/Cr, Cho/Cr, and mIns/Cr ratios are summarized in Table 2. There was no significant difference in NAA/Cr, Cho/Cr, and mIns/Cr ratios between the NAWM of the patients and the WM of the control subjects (independent-samples t test; P = .704, .810, and .907).
Mean NAA/Cr, Cho/Cr, and mIns/Cr ratios obtained from the WM of healthy subjects, NAWM in MS, CDL, and EDL
In the MS group, the mean NAA/Cr was lower in CDLs (1.45 ± 0.44) than in the NAWM (1.56 ± 0.53) and the control WM (1.61 ± 0.344), but the difference did not reach statistical significance (paired-samples t test, P = .647; and independent-samples t test, P = .175 respectively). Similarly, the mean Cho/Cr was greater in CDLs (1.110 ± 0.249) than in NAWM (1.033 ± 0.225) and control WM (1.016 ± 0.263), but the differences were not significant (paired-samples t test, P = .111; independent-samples t test, P = .211, respectively). The mean mIns/Cr was significantly higher in CDLs (0.557 ± 0.188) than in the NAWM of patients with MS (0.411 ± 0.094, paired-samples test, P = .000) and the WM of normal subjects (0.414 ± 0.116, independent-samples t test, P = .03). NAA/Cr, Cho/Cr, and mIns/Cr ratios in the EDLs did not differ significantly from those of the WM of control subjects (independent-samples t test; P = .279, .326, and .848, respectively).
There was no correlation of any computed ratio and age at imaging, age at disease onset, duration of disease, and number of relapses in lesions and NAWM of patients with MS (Pearson correlation analysis, P > .05).
Discussion
Abnormalities of myelin might underlie the pathogenesis in a certain proportion of patients with MS.9 Among these, citrullination of MBP has been associated with a propensity to myelin disruption in transgenic mice.10 Citrullination, one of numerous posttranslational modifications, results in a less cationic protein through loss of 1 positive charge for each arginine converted to citrulline. Thus, the interaction of MBP with lipids and its “glue activity” for adjacent bilayers are reduced.11,12 In addition to such structural alterations, citrullinyl residues are associated with faster digestion of MBP by proteases.4 The enzymes involved in deimination, peptidylarginine deiminases (PADs), have been found upregulated in MS due to hypomethylation of their promoter region.9 Levels of both PAD enzymes, PAD2 and PAD4, were increased significantly in myelin fractions of patients with MS, as was the amount of citrulline.13,14
Degradation or altered antigenic structure of citrullinated MBP may also provide more antigenic material to the immune system. Patients with MS had a higher overall number of citrullinated MBP-C8-responding cell lines and/or responded with greater sensitivity to the citrullinated MBP antigen. If citrullinated MBP is present in MS brain tissue, a preferential T-cell response to this compound may be involved in the induction and perpetuation of the disease.15
Our study is the first radiologic investigation of citrulline in the WM of patients with MS by using 1H-MR spectroscopy, as described earlier.7,8 Following identification of major resonance peaks and computation, spectral narrowing between 2.75 and 3.5 ppm enabled investigation of the citrulline peak with little expense of time. Citrulline peak was identified in a significantly higher proportion of subjects with MS compared with control subjects. This finding can be attributed to citrullinated MBP and conforms to other biochemical and histopathologic studies in which citrullinated MBP was increased in the WM of patients with MS.5,9 We found it in 28% of CDLs, in 32% of NAWM, and in 12.5% of EDLs that were sampled. As a necessity of the technique (svs) and time constraints, analysis was made from a single lesion of different demyelinating stages (ie, CDL or EDL), as well as a single location of the NAWM. Although the relatively small number of each type of lesion does not allow us to make a complete comparison, our impression is that the citrulline peak tends to occur more frequently in NAWM or chronic lesions of MS.
Longitudinal studies investigating demyelinating lesions throughout their evolution and whole-brain 1H-MR spectroscopy for overall parenchymal analysis may clarify the relation of citrulline with the pathogenesis of MS lesions. Because MS lesions are usually smaller than our voxel volume (1.5 cm3), some perilesional WM might have been included in our VOI. However, this adjacent parenchyma is completely “normal” only according to conventional radiologic description: Biochemical and histopathologic studies show gliosis, perivascular inflammation, microglial activation, blood-brain barrier disruption, and axonal loss in such areas.16 We, therefore, think that the presence of such a minute volume of perilesional WM in the VOIs is less likely to contribute to major changes in our findings.
Advanced imaging techniques also showed abnormalities on magnetization transfer imaging, 1H-MR spectroscopy, diffusion-weighted, and diffusion-tensor imaging, even 2 years before the appearance of lesions in T2-weighted images, supported early alterations in NAWM.17–19 Because we could only examine patients already diagnosed with MS, we do not know whether the presence of citrulline preceded or followed the diagnosis of MS. However, although citrulline was increased in the NAWM of MS brains, we found no significant difference in NAA-, Cho-, and mIns-Cr ratios. These findings suggest overcitrullination of MBP precedes the inflammatory demyelinating process. Moreover, the age of the patient and duration or activity of disease did not correlate with citrulline, also arguing against a secondary or acquired abnormality of myelin after the onset of MS.
On the other hand, certain patients had citrulline in chronic lesions but not in the NAWM; this may suggest that citrullinated myelin appears at a certain stage of the lesion and the NAWM containing citrulline is in fact “healed” parenchyma. The so-called NAWM showing subtle abnormalities on functional and metabolic imaging studies in MS may be the site of active pathology or can be affected by an indirect mechanism as occurs in epilepsy or brain injury.20 Although any past or subtle involvement of these areas cannot be completely ruled out in our patients, we think this is less likely considering the relatively young age, short duration of disease, low number of clinical relapses, and active inflammatory MR imaging lesions in our patients and the lack of correlation between the presence of citrulline and disease duration.21
The citrullinated MBP, also called C-8, constitutes all MBP up to 2 years of age, and adult ratios are reached at 4 years of age.2 We believe that we did not observe the physiologically immature WM because the youngest patient in our series was 4 years old and his MR spectroscopy study revealed no citrulline peak, as did our 3 other patients with MS and 3 control subjects younger than 10 years of age. The presence of the peak in healthy individuals on 1H-MR spectroscopy in our present and previous experiments is not surprising because citrullinated MBP constitutes about 20% of the MBP isolated from normal brain and there is no demonstrated border between mature and immature WM.2 Besides, the citrulline concentration associated with the appearance of the peak on 1H-MR spectroscopy imaging is unknown. MR spectroscopy studies on high-field systems would delineate the peak more precisely and possibly in a greater portion of the individuals as a benefit of increased signal intensity–to-noise ratio and improved spectral separation, especially at short TEs.22 Therefore, although our 3 citrulline-positive controls may be part of the normal spectrum, their follow-up for long periods is mandatory to determine any susceptibility to developing demyelinating disease.
Clinical 1H-MR spectroscopy studies performed in adult patients with different forms of MS have frequently reported decreased NAA and NAA/Cr in lesions and in NAWM even at the earliest stages.23 The reduced NAA of acute demyelinating lesions may remain decreased or show partial recovery, which may be related to the resolution of edema, increases in the diameter of previously shrunk axons after remyelination, and reversible metabolic changes in neurons.24,25 Despite a tendency to reduction, our patients’ chronic lesions and NAWM did not show significant decreases in these metabolites. This may indeed reflect better neuroaxonal recovery in patients with early-onset MS even if affected previously as assessed by the applied technique. On the other hand, significant increase in mIns/Cr of the chronic lesions compared with the NAWM of patients with MS and the WM of control subjects agrees with other reports suggesting intense glial proliferation.18,26
Our findings support previous biochemical and pathologic studies of citrullinated MBP being involved in the pathogenesis of MS. Longitudinal follow-up of patients and 1H-MR spectroscopy investigations in asymptomatic relatives of patients with MS, whose WM tends to contain lower NAA/Cr and higher Cho/Cr than the WM of healthy subjects, might also give information on the role of citrulline in preclinical, acute clinical, and silent phases of MS.27
Conclusions
Biochemical and histopathologic studies propose that overcitrullinated MBP has a role in MS. We performed the first study investigating citrulline in patients with MS by using 1H-MR spectroscopy. A citrulline peak was present significantly in a higher proportion of 1H-MR spectroscopy findings of patients with early-onset MS than of healthy subjects. This finding also suggests that increased citrullination of myelin proteins has an association with demyelinating diseases of the CNS. Further studies to explore its occurrence in various stages of demyelinating lesions or asymptomatic relatives of patients with MS are needed.
Acknowledgments
We thank all participating patients and families and their physicians, including Dr Mefkure Eraksoy, İstanbul University, Department of Neurology, and Dr Coskun Yarar, Gazi University, Department of Child Neurology. We also thank the Turkish Child Neurology and Developmental Child Neurology Associations for their support in this study.
References
- Received August 7, 2007.
- Accepted after revision October 26, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.