
Abstract
BACKGROUND AND PURPOSE: ICAS is one of the therapeutic options in symptomatic cerebral artery stenosis. iaDSA is the current criterion standard examination after ICAS for the detection of ISR. In this study, we evaluated ivACT as a potential noninvasive follow-up alternative.
MATERIALS AND METHODS: In 17 cases, ivACT and iaDSA were performed after ICAS. Both procedures were carried out on a flat-panel-detector-equipped angiography system. Postprocessing of ivACT acquisitions was performed on a dedicated workstation producing multiplanar reformations of the stent region and other intracranial arteries. Restenotic lesions were compared with iaDSA measurements. All studies were independently evaluated by 2 experienced neuroradiologists blinded to patients data.
RESULTS: In 5 cases, ISR was diagnosed on iaDSA images. All restenotic lesions were reliably detected (sensitivity, 100%; 95%CI, 48%–100%) and could be correctly quantified on ivACT images in comparison with iaDSA. The neuroradiologists correctly excluded ISR in 11 of 12 lesions after viewing the ivACT examinations (specificity, 92%; 95%CI, 62%–100%). Measurements of ISR on ivACT were highly correlated to iaDSA (Pearson r = 0.94, P < .01).
CONCLUSIONS: IvACT is a promising noninvasive follow-up examination after ICAS. With its high spatial resolution, it can reliably detect or exclude ISR. Contrary to iaDSA, there is no need for a recovery period after ivACT and the risk of neurologic complications is practically lowered to zero.
Abbreviations
- A2
- second segment of anterior cerebral artery
- ACT
- angiographic CT
- BA
- basilar artery
- C3
- third segment of ICA
- CI
- confidence interval
- CTDIw
- weighted CT dose index
- ΔDSA%
- change of stenosis percentage at follow-up iaDSA compared with measurements on iaDSA after stenting
- DSApost
- digital subtraction angiography after stenting
- DSApre
- digital subtraction angiography before stenting
- DWI
- diffusion-weighted imaging
- IA
- focal lesion involving the end of the stent
- iaDSA
- intra-arterial digital subtraction angiography
- IB
- focal lesion involving the body of the stent
- IC
- multiple restenotic foci involving <50% of the stented segment
- ICA
- internal carotid artery
- ICAS
- intracranial artery angioplasty and stenting
- II
- diffuse intrastent lesion
- ISR
- in-stent restenosis
- ivACT
- ACT after intravenous contrast medium application
- M1
- first segment of middle cerebral artery
- MDCTA
- multidetector CT angiography
- PTA
- percutaneous transluminal angioplasty
- rePTA
- repeated PTA after ICAS
- TIA
- transient ischemic attack
- V4
- intracranial segment of vertebral artery
ICAS is a viable treatment option in the case of symptomatic intracranial atherosclerotic disease. Due to the high stroke risk under medical treatment, patients with high-grade (>70%) symptomatic intracranial stenosis represent the main target group for alternative endovascular treatment concepts such as ICAS.1 During follow-up, ISR seems to be a major problem, with ≤30% of the patients with ICAS presenting with ISR after 6 months.2,3 The main mechanism of ISR is myointimal hyperplasia. Turk et al2 reported that the rate of ISR was 31.2%, with 31.0% of the lesions being symptomatic. Especially younger patients with intracranial stenosis of the ICA or the M1 segment of the middle cerebral artery have shown a high risk of developing ISR, which may cause stroke in the first 12 months in ≤5% of the cases. Whether restenosis rates are relevant is still under discussion, but it remains undisputable that follow-up is necessary.4,5
Conventional iaDSA is the current criterion standard follow-up examination after ICAS, and as such, it has been primarily used in studies evaluating ISR rates.6,7 Due to its invasive nature, iaDSA carries the risk of neurologic complications, especially in elderly patients with known cardiovascular disease and when fluoroscopic times are ≥10 minutes.8 Recent studies have shown that, within a high-volume neurointerventional department, the risk for neurologic complications during iaDSA is close to zero.9 Nevertheless, the accessibility of a high-volume institution is not always guaranteed for patients having their follow-up after ICAS, and even in high-volume centers, it is impossible to ensure that every iaDSA will be performed by an experienced operator. A new noninvasive technique for the depiction of intracranial vessels after ICAS is the ivACT.10 Buhk et al10 demonstrated, in a small series, that ivACT, in comparison with MDCTA, is a feasible follow-up option for the delineation of in-stent pathologies or the exclusion of ISR. While MDCTA has been proved a reliable tool for screening intracranial artery stenosis,11 in vitro studies have shown that it is insufficient for the assessment of ISR. Trossbach et al12 concluded that it is impossible to visualize the different stenoses subjectively—that is, without using image-analysis software—in a series of in vitro examinations delineating different grades of ISR in 3 and 4 mm stents for intracranial angioplasty. Similar conclusions have been drawn in studies evaluating MDCTA in the assessment of ISR in coronary stents.13 On the other hand, earlier studies have already presented the potential of ACT in the evaluation of small coronary stents. In their study, Mahnken et al14 noted that ACT proved to be superior to MDCT for in vitro visualization of coronary artery stents because the improved spatial resolution of ACT enabled better depiction of the stent lumen. This characteristic of ACT also allows the cross-sectional evaluation of normal or abnormal deployment of small intracranial stents, which is impossible with other imaging modalities such as MDCT, DSA, or MR imaging.15
Other noninvasive techniques allowing the detection of ISR include transcranial duplex sonography and quantitative MR angiography.16,17 However, both of these lack the ability to provide anatomic data of the stent region, and especially duplex sonography is limited due to its dependence on operator experience and the anatomy of the temporal bone window.
The purpose of this study was the evaluation of ivACT in the detection of ISR and the comparison with iaDSA findings in the follow-up of 17 cases after ICAS.
Materials and Methods
Patients
Fourteen patients were treated with ICAS of a symptomatic intracranial artery stenosis from July 2006 to May 2009 (10 men, 4 women; mean age, 60 years; range, 45–75 years). One patient received 2 intracranial stents (petrous ICA and M1), and in another patient, 3 follow-up examinations were performed in the time period mentioned above: the first, 3 months after ICAS; the second and third, 7 and 4 months after the first and second PTA of a recurrent high-grade ISR, respectively. Locations of stenoses, presenting symptoms, and applied stent systems are shown in On-line Table 1. All patients were admitted for standard follow-up within an average of 7 months (range, 3–12 months) after ICAS.
Approval of the local ethics committee and informed patient consent were obtained.
Image Acquisition
IvACT acquisitions and iaDSA examinations were performed on a biplane angiography system equipped with flat panel detectors (Axiom Artis dBA, Siemens, Erlangen, Germany). DSA data included only standard angiography series. For the acquisition of ivACT, we used the DynaCT program of our suite (Siemens) with the following parameters: 20 seconds of rotation; 538 projections; 220° total angle; CTDIw, approximately 35 mGy (manufacturer information); and a 30 × 40 cm detector, which allows the reconstruction of a nontruncated volume of approximately 22 cm (in-plane) and 16 cm (in the z-direction). While planning the DynaCT, we placed the stented segment near the center of the FOV, because a higher image quality is guaranteed near the central plane of the conebeam.18 However, we avoided placing the stented segment exactly in the center of the conebeam because ring artifacts can negatively affect the image quality.19 Postprocessing of the rotational image data to a volume dataset was performed by using dedicated commercial software on a Leonardo medical workstation (InSpace 3D; Siemens). The software includes system-specific algorithms to correct beam-hardening, scattered radiation, truncated projections, and ring artifacts. Reconstruction resulted in a volume dataset of approximately 400 sections with a 512 × 512 matrix and an isotropic spatial resolution of approximately 0.1 × 0.1 × 0.1 mm3. The ivACT datasets were further processed to multiplanar reformations parallel and perpendicular to the stent region with a section thickness of 0.2–0.3 mm and maximum intensity projections of the other intracranial vessels. Before acquisition, 100 mL of iomeprol (Imeron 400; Bracco ALTANA Pharma, Konstanz, Germany) had been injected into a cubital vein at a flow rate of 5 mL/s by using a power injector. The start delay for rotational acquisition was 14–20 seconds, depending on the age and cardiopulmonary status of the patient. During ivACT, the patient was asked to close his or her eyes and to breath-hold during the 20 seconds of the C-arm rotation.
Image Analysis
Two neuroradiologists (M.-N.P., A.X.) independently performed the image viewing and rating on the above-mentioned Leonardo medical workstation by using the Warfarin-Aspirin Symptomatic Intracranial Disease study technique.1 As in the study of Albuquerque et al,6 ISR was defined as >50% stenosis within or adjacent (within 5 mm) to the stent as well as >20% absolute luminal loss at follow-up imaging. Moreover, all restenotic lesions, even those not fulfilling the criteria of ISR, were categorized by using the modified Mehran classification system.6 This system, originally developed to describe ISR after coronary PTA with stent placement, divides ISR into 4 subgroups: class I, a focal group with lesions involving <50% of the stented segment; class II, a diffuse intrastent group (>50% of the stented segment); class III, a proliferative group with lesions expanding beyond the confines of the stent; and class IV, a complete stent occlusion group. Class I lesions can be further categorized IA, IB, or IC cases. ISR cases were then compared with the original lesions presented for treatment.
Statistical Analysis
The mean value of each pair of measurements (rater 1, rater 2) was then calculated and used for further statistical analysis. The correlation between ISR percentage measures on ivACT and iaDSA examinations was assessed by the Pearson correlation coefficient r. Additionally, a simple linear regression of ivACT versus iaDSA was performed. Considering iaDSA as the criterion standard for the detection of ISR, we calculated empiric sensitivity and specificity, as well as the positive and negative predictive values for ivACT as a detection method. Statistical significance was assumed for P values < .05. All analyses were conducted with the free software R (version 2.8, http://www.r-project.org).
Results
Follow-up imaging with iaDSA and ivACT was obtained for 17 stenotic lesions. Measurements and descriptive results can be seen in On-line Table 2. Nine lesions had been treated with a self-expanding intracranial nitinol stent (Wingspan; Boston Scientific, Natick, Massachusetts), 4 with a relatively new balloon-mounted stent designed for intracranial use (Pharos; Micrus Endovascular, Renens, Switzerland), and another 4 lesions with a common coronary stent (Driver RX, Medtronic, Minneapolis, Minnesota). IaDSA excluded ISR in 12 of 17 lesions (70.6%). Five lesions (29.4%) developed ISR during the follow-up interval, and 4 of them were treated successfully with another PTA. The patient in case 4 developed a mild ISR with 54% restenosis (Δ = 22%), for which angioplasty was not considered necessary. At follow-up, 2 of the 5 ISR lesions were symptomatic with a TIA, while the rest presented no new symptoms. The average change of stenosis percentage at follow-up compared with measurements before ICAS documented an absolute reduction of 40% (range, −90% to +9%); compared with the percentages of stenoses directly after ICAS, an average increase of 21% could be confirmed with iaDSA after the follow-up interval (range, 0%–63%). With the modified Mehran system, a restenotic pattern could be described in 9 of 17 lesions (though only 5 fulfilled the criteria for an ISR). Seven of 9 restenotic lesions were characterized as focal lesions involving <50% of the stented segment (class I), of which 5 were group IB and 1, group IA and IC, respectively. Two lesions demonstrated diffuse stenosis (class II), but there were no proliferative lesions (class III) or complete stent occlusions detected.
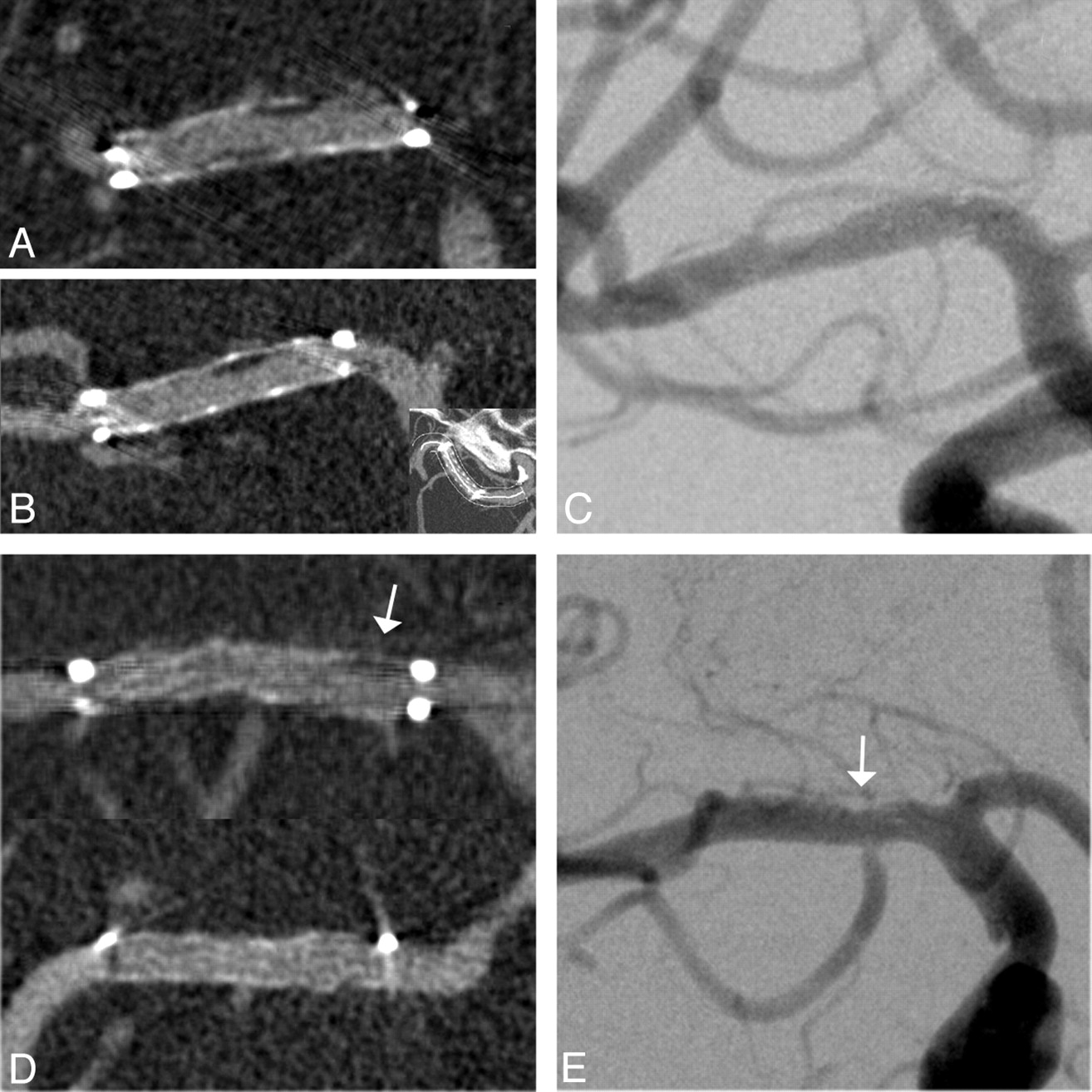
IvACT was of diagnostic quality in all 17 cases examined. No motion artifacts−related problems were encountered, and sufficient delineation of the intracranial vessels and the stented segment was demonstrated. Only the radiopaque stent markers of the Wingspan stent proved to be a problem because a very short segment could not be delineated due to streak artifacts. The confines of the other stents could be depicted without any limitations due to metal artifacts. The neuroradiologists correctly excluded ISR in 11 of 12 lesions after viewing the ivACT examinations (specificity, 92%; 95% CI, 62%–100%). The cases presented in Fig 1 illustrate 2 examples in which ISR was correctly excluded in ivACT, in accordance with iaDSA measurements. With ivACT, there was 1 false-positive diagnosis of ISR (case 2). In this case, a Wingspan stent (2.5 × 15 mm) had been placed in a symptomatic stenosis of the right M1 segment and was expanded to 1.8 mm. On follow-up imaging, a 70% ISR was detected in ivACT, whereas iaDSA excluded an ISR with 33% residual stenosis (ΔafterICAS = 0%, Fig 2). All restenotic lesions were sufficiently depicted in ivACT (sensitivity, 100%; 95% CI, 48%–100%) and could be correctly quantified and categorized by using the modified Mehran system. Thus, a positive predictive value of 83% (95% CI, 36%–100%) and a negative predictive value of 100% (95% CI, 71%–100%) could be achieved with ivACT.

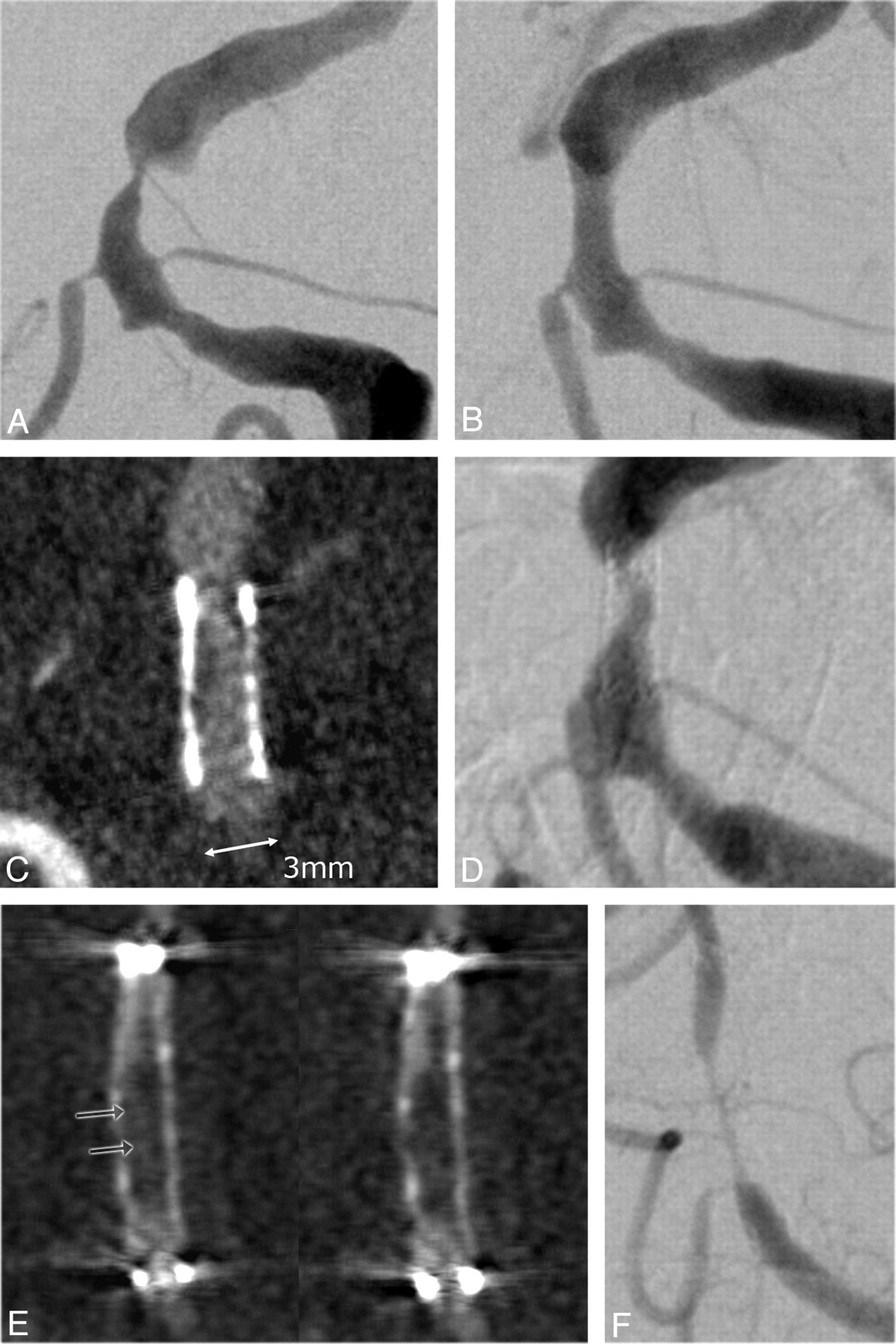
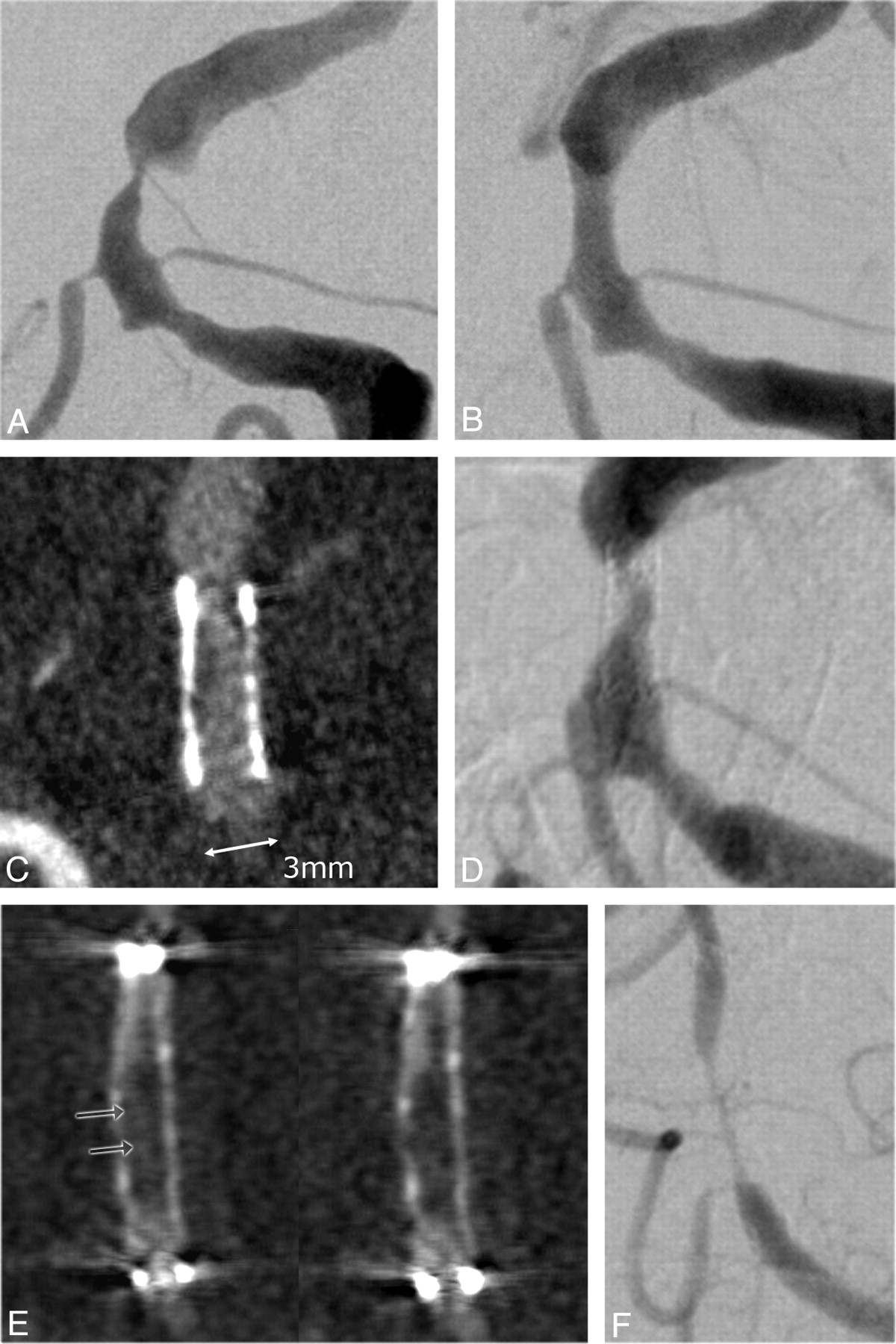
Follow-up images of a 56-year-old woman 7 months after ICAS of a 76% middle cerebral artery stenosis. A and B, Excellent delineation of in-stent anatomy on coronal (A) and curved planar (B) ivACT reformations allows exclusion of a high-grade ISR and detection of low-grade neointimal hyperplasia within the body of the stent. C, The same findings are demonstrated on the iaDSA image. D and E, Another example of a low-grade restenotic lesion (25%), which is depicted in the proximal stent portion (arrows) on both ivACT (D) and a standard iaDSA image (E). This 61-year-old woman was admitted to standard follow-up without any new symptoms after ICAS of a symptomatic 79% middle cerebral artery stenosis. At the confines of the Wingspan stent, streak artifacts limit the image quality on ivACT reformations.

ISR is falsely diagnosed by both raters on transversal (A) and coronal (B) ivACT reformations. C, On both images, a restenotic lesion is delineated at the distal stent portion. ISR can be excluded by iaDSA. The patient was admitted 2 months earlier than his planned follow-up appointment, despite no new symptoms, due to suspected restenosis on transcranial duplex sonography.
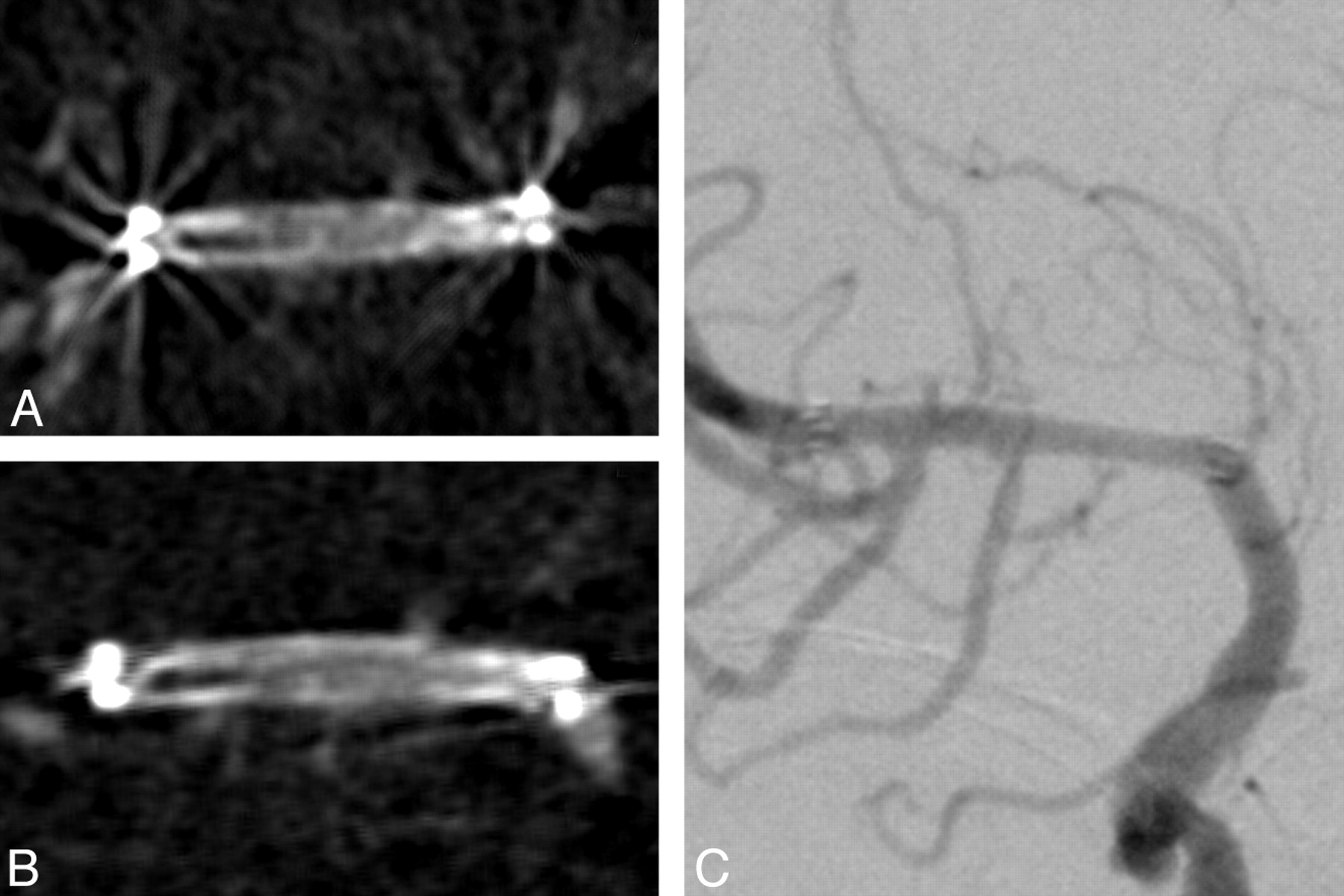
Figure 3 shows the follow-up images of a 69-year-old male patient. Seven months after ICAS of a symptomatic BA stenosis, the patient was admitted for standard follow-up imaging without any new symptoms. IvACT revealed a high-grade ISR within the applied Pharos stent (78% ISR, class II), which was verified by iaDSA, with which an 81% ISR could be depicted. ISR quantification on ivACT images was highly correlated to iaDSA (Pearson r = 0.94, P < .01). Therefore, we built a simple linear regression model of both parameters, the estimated coefficients of which are depicted in Fig 4.
Images of a 69-year-old patient before (A) and after (B) ICAS of a high-grade (85%) symptomatic BA stenosis. The patient was admitted to follow-up without any new symptoms 7 months after stent placement. C and D, ISR is depicted on ivACT reformations (C), a finding that is confirmed on iaDSA (D). The stenosis percentage on ivACT and iaDSA correlates excellently. E and F, In another example of a 45-year-old woman, high-grade ISR can be reliably diagnosed on ivACT (E) due to extensive neointimal hyperplasia. The residual filiform lumen within the stent can be correctly measured on ivACT reformations (E, arrows), compared with iaDSA images (F).

Scatterplot of ivACT (%) versus iaDSA (%) plus an estimated regression line.
Discussion
ICAS is a promising new therapeutic option in patients with symptomatic intracranial atherosclerotic disease, especially when stenotic lesions are refractory to medical treatment.3,7,20 However, ISR rates of ≤31% have been reported in the past, proving the necessity for reliable follow-up imaging. The current criterion standard, iaDSA, has known issues due to its invasive nature, carrying the risks of neurologic or other periprocedural complications.8
Noninvasive follow-up imaging of small intracranial stents for the detection of ISR has not been very successful to date. Commonly used stainless steel coronary stents cause metal artifacts on CT and significant signal intensity loss on MR images. Nitinol stents are more compatible with MR imaging, but exact depiction of the in-stent region and exact measurement of ISR are not possible. Duplex sonography is another noninvasive follow-up examination for the detection of ISR.16 However, the absence of a sufficient temporal bone window, the investigator dependency, and its substantial limitations in the assessment of the petrous segment of the ICA or the BA restrict the use of duplex sonography as a first-line follow-up technique. Small series have shown the feasibility of MDCTA as a follow-up after ICAS,21 but larger in vitro studies have concluded that it is insufficient for the exact quantification of ISR in small vessel stents.12 Similar results have been shown in studies evaluating MDCTA in the assessment of ISR in small coronary stents.13
On the contrary, ACT has proved to be a technique with performance characteristics suitable for imaging small high-contrast structures such as intracranial stents.22 Due to its superior spatial resolution compared with MDCT, ACT has already proved to be better for the depiction of self-expandable intracranial stents or other small objects, such as cochlear implants.15,23 The slightly inferior contrast resolution leads to insufficient detection of ischemic lesions on ACT compared with MDCT,24 but in high-contrast imaging (such as ivACT and MDCTA), this minor difference does not have a significant influence on image quality. Also, contrary to MDCT, reconstruction of ACT rotational data results in volume datasets with isotropic voxel size, meaning sufficient image quality on multiplanar reformations even if the stent is not aligned to the conebeam axis (vessels with curved shape, irregular walls, and so forth, Fig 1).12,25 The addition of intravenous contrast medium has created a “mixture” with the ability of sufficient depiction of ISR.10 This potential is very important if one takes into account the increased use of intracranial stents, not only for revascularization of stenotic vessels but also for treating cerebral aneurysms.26,27 Moreover, the use of new flat detector technologies and new reconstruction algorithms may, in the near future, allow dynamic perfusion imaging to be extracted from the same ivACT dataset used for angiographic imaging. This would facilitate the assessment of hemodynamic relevance of the stenotic lesion in addition to quantification of restenosis.28
In our study, ivACT showed a high sensitivity and specificity for the detection of ISR compared with iaDSA. We could successfully detect and quantify ISR on ACT images in all 5 patients presenting an ISR at follow-up iaDSA. Additionally, in 11 of 12 cases without an ISR, ivACT sufficiently excluded a restenotic lesion. In the majority of cases, these were stents with diameters of 2.75–4 mm. In only 1 case, both neuroradiologists falsely diagnosed an ISR on ACT images. A possible explanation could be the size of this stent because it was a 2.5-mm Wingspan stent self-expanded to a diameter of 1.8 mm, as well as the streak artifacts near the confines of the stent (Fig 2).
Regarding the radiation dose, the use of a 20-second ACT protocol results in a CTDIw value ∼ 3 5 mGy, which is comparable with or even lower than the usual MDCTA or conventional cranial CT protocols (∼60 mGy).29,30 The dose could be further reduced with the application of a 5-second (CTDIw ∼ 9 mGy) or an 8-second ACT protocol. However, longer rotating time is currently necessary to achieve sufficient contrast resolution for the depiction of ISR. Kyriakou et al31 report in their publication that “the sampling artifacts, originating from the small number of projections in high speed (5 seconds), are quite distinct, and in high-speed protocols low tissue resolution is nearly nonexistent.” In contrast to other studies that have used a high-dose 20-second ACT protocol with a CTDIw ∼ 75 mGy, we used the low-dose protocol solely in our study.23,31
The amount of contrast media used for ivACT in our study is higher than the amount being used in a conventional MDCTA (∼60 mL in our department). The reason for this difference is the necessity of a longer acquisition time with the ACT protocol. To achieve an adequate contrast throughout the whole rotation, one must inject large amounts of contrast media continuously. We are currently using a modified protocol with 90 mL of contrast medium followed by 30 mL of saline flush, but a definite solution to the contrast dosage issue will be the deployment, in the future, of a shorter rotation protocol, with contrast and spatial resolution comparable with the currently used 20-second ACT.
The limitations of this study include its small sample size, the absence of bolus-tracking for ivACT, and the metal artifacts around the markers of the Wingspan stent. Larger studies have to be conducted to verify the value of ivACT in the follow-up imaging after ICAS. Although the first results are very promising, the absence of a bolus-tracking method after intravenous contrast medium administration could sometimes result in an insufficient depiction of intracranial vessels. This would mean repeated examinations and increased overall radiation and contrast dosage for the patient. We are currently working with the manufacturer on this issue, and we think that a viable method of bolus-tracking will be available in the months to come. Regarding the streak artifacts at the confines of the Wingspan stent, one should consider that an ISR that includes the confines of a stent is an infrequent one (modified Mehran IA).6 Moreover, with the development of new metal artifacts-reduction algorithms for ACT, even the marker region of the Wingspan stent may be visible without any streak artifacts in the near future.32
Conclusions
IvACT is a promising new noninvasive follow-up tool after ICAS. In our sample, we could detect ISR on ivACT images with a high sensitivity and specificity. Further research is required to conclude that ivACT could replace iaDSA as a standard follow-up examination after ICAS.
Footnotes
-
Paper previously presented at: 34th Annual Meeting of the European Society of Neuroradiology, September 17–20 2009; Athens, Greece. Preliminary results after 10 cases.
Indicates article with supplemental on-line tables.
References
- Received February 16, 2010.
- Accepted after revision April 13, 2010.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Quantitative analysis of high-resolution, contrast-enhanced, cone-beam CT for the detection of intracranial in-stent hyperplasia
- Successful detection of embologenic ulceration in a symptomatic non-hemodynamic intracranial stenosis using C-arm cone beam CT
- Feasibility of Intravenous Flat Panel Detector CT Angiography for Intracranial Arterial Stenosis
- Applicability of Tableside Flat Panel Detector CT Parenchymal Cerebral Blood Volume Measurement in Neurovascular Interventions: Preliminary Clinical Experience
- Feasibility of Flat Panel Angiographic CT after Intravenous Contrast Agent Application in the Postoperative Evaluation of Patients with Clipped Aneurysms