
Abstract
SUMMARY: In accelerated hypertension, vasogenic brain edema associated with PRES may represent either autoregulatory breakthrough leading to vasodilation or excessive autoregulation leading to vasoconstriction. We describe 2 patients with PRES in accelerated hypertension who had serous retinal detachments, a vasoconstrictive phenomenon. The concurrence of serous retinal detachment and PRES offers intriguing support for the idea that vasoconstriction rather than vasodilation is the mechanism of vasogenic edema in PRES.
ABBREVIATIONS
- CCA
- catheter cerebral angiography
- DWI
- diffusion-weighted imaging
- FLAIR
- fluid-attenuated inversion recovery
- MRA
- MR angiography
- PCA
- posterior cerebral artery
- PRES
- posterior reversible encephalopathy syndrome
- RPE
- retinal pigment epithelium
PRES is manifested clinically by headache, seizures, altered mental status, and retrogeniculate visual loss, with scattered foci of high T2/FLAIR signal intensity without restricted diffusion, reflecting vasogenic edema.1 In the setting of accelerated hypertension, there are 2 competing hypotheses to explain the vasogenic edema: 1) autoregulatory breakthrough leading to the dilation of cerebral arterial vessels, hyperperfusion injury to the capillary bed, and secondary cerebral edema2,3; and 2) autoregulatory excess leading to constriction of cerebral arterial vessels, ischemia of vascular endothelial cells, and vascular leakage.4,5
The choroidopathy of hypertension is attributed to vasoconstriction of choroidal arterioles,6 which causes RPE necrosis and overlying serous detachment of the retina. Although commonly reported in acute hypertension, choroidopathy has been described in only 1 case of hypertensive encephalopathy7 and never in PRES.
We describe 2 patients with serous retinal detachment and PRES in the setting of accelerated hypertension. The occurrence of choroidopathy in PRES offers anecdotal support for vasoconstriction as the mechanism underlying the vasogenic edema of PRES in accelerated hypertension.
Case Reports
Case 1.
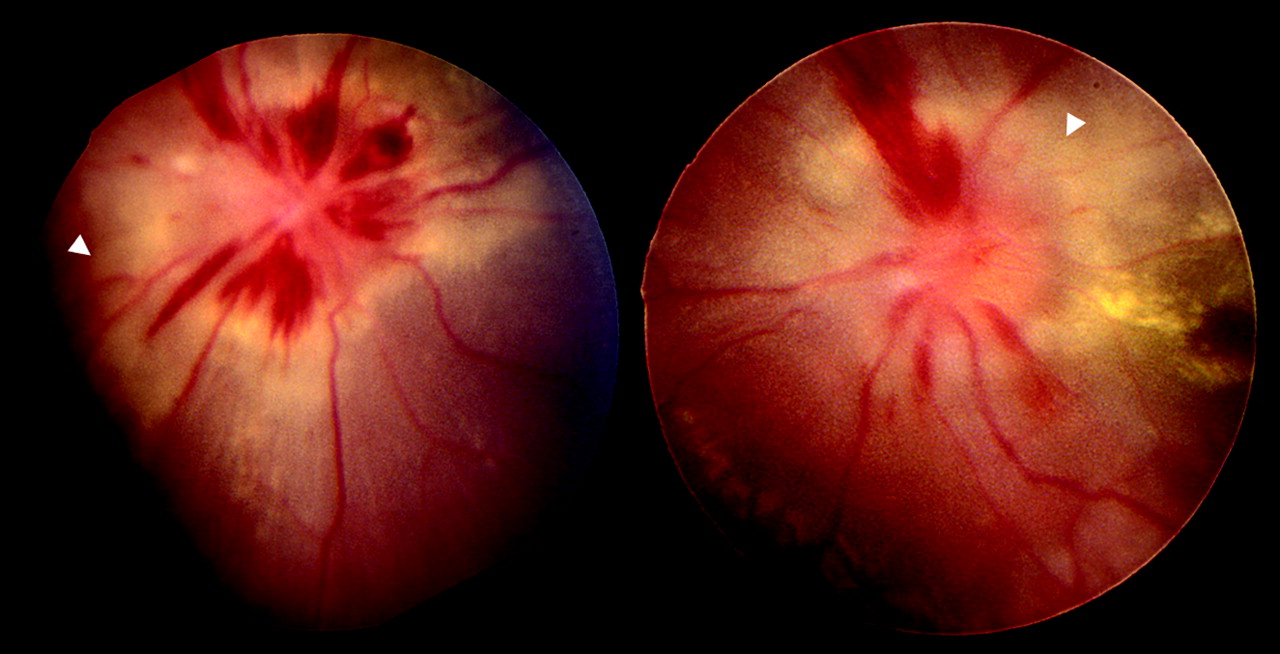
A 22-year-old woman with angioimmunoblastic lymphoma, treated with cyclophosphamide, hydroxydaunorubicin, vincristine, prednisolone, and gemcitabine, developed renal failure, severe hypertension (182/96 mm Hg), generalized seizures, and depressed consciousness. Ophthalmoscopy revealed bilateral peripapillary serous retinal detachment (Fig 1). After she returned to full consciousness, a complete right homonymous hemianopia was elicitable. MR imaging demonstrated high T2/FLAIR signal intensity in the posterior parietal and occipital lobes without restricted diffusion (Fig 2), a finding compatible with PRES. The serous retinal detachments disappeared within weeks, but the right homonymous hemianopia persisted. Repeat brain MR imaging showed disappearance of the signal-intensity abnormality in the right occipital lobe and development of restricted diffusion in the left occipital lobe, implying conversion to infarction (not shown).

Case 1. Peripapillary serous retinal detachments are evident in both eyes.

Case 1. Brain MR imaging performed at presentation. A, Axial FLAIR study shows high signal intensity within the parieto-occipital regions bilaterally in a distribution typical for PRES more on the left side (black arrow) than the right side (white arrow). B and C, Axial DWI study (B) shows high signal intensity, but an apparent diffusion coefficient study (C) does not show corresponding low signal intensity, findings indicative of vasogenic edema.
Case 2.
A 15-year-old boy presented with a seizure in the setting of severe hypertension (250/140 mm Hg) secondary to crescentic glomerulonephritis. Ophthalmoscopy showed serous retinal detachment, optic disc swelling, hard exudates, and peripapillary flame-shaped hemorrhages bilaterally (Fig 3). MR imaging demonstrated occipital T2/FLAIR hyperintensities without restricted diffusion, consistent with PRES (Fig 4). After the patient returned to full consciousness, visual acuity was 20/200 in both eyes and Humphrey visual fields showed enlarged blind spots. During the next 6 weeks, visual acuity gradually recovered to 20/20 bilaterally. In view of the recovery of vision, brain MR imaging was not repeated. Six months later, visual acuity remained 20/20 in both eyes, but he had tiny scotomas, corresponding to infarcts of the RPE (not shown).
Case 2. Optic disc swelling, hard exudates, peripapillary flame-shaped hemorrhages, and peripapillary serous retinal detachment are evident in both eyes.

Case 2. Brain MR imaging performed at presentation. A, Axial FLAIR study shows high signal intensity within the occipital regions bilaterally (white arrows) in a distribution typical for PRES. B and C, Axial DWI (B) shows moderately high signal intensity in the occipital regions bilaterally (white arrows), but an apparent diffusion coefficient study (C) did not show corresponding low-signal-intensity findings indicative of vasogenic edema.
Discussion
We have described 2 patients who developed binocular serous retinal detachments in the setting of accelerated hypertension and PRES. Considering that clinical, pathologic, and experimental evidence indicates choroidal vasoconstriction as the underlying cause of serous retinal detachments, we believe that these cases fortify the concept that vasoconstriction rather than vasodilation underlies the development of PRES.
Ample evidence supports a link between systemic hypertension and vasoconstrictive choroidopathy. Histopathologic studies of postmortem specimens drawn from the acute ischemic phase of hypertension show constriction of choroidal arterioles with obliteration of their lumina.6 Patchy filling of the choriocapillaris on fluorescein angiography has been documented in patients with hypertension8; and fibrinoid necrosis of choroidal arteries and arterioles with occlusion of the choriocapillaris has been noted on histopathogic studies of human eyes with accelerated hypertension.9 Primate models of renovascular hypertension have shown serous retinal detachment and RPE lesions associated with delayed or patchy choroidal filling.6
The vasodilation mechanism of PRES in accelerated hypertension is supported by studies showing increased perfusion in the edematous portions of the brain in patients with hypertensive encephalopathy.3 However, emerging evidence suggests that vasoconstriction is a better explanation for the PRES of accelerated hypertension. In patients with acute hypertension, Brubaker et al4 found significant posterior brain hypoperfusion, reduced cerebral blood volume, reduced cerebral blood flow, and a heterogeneous pattern of mean transit time on perfusion MR imaging. Other MR perfusion studies10,11 of PRES have revealed that relative cerebral blood volume is reduced in high-signal-intensity areas of the cerebral cortex and white matter compared with normal-signal-intensity areas.
In a retrospective study of patients with PRES by using CCA and MRA, Bartynski and Boardman12 observed that 87% of patients showed diffuse vasoconstriction, focal vasculopathy, or vessel pruning of the PCA. Vasospasm on CCA and MRA and watershed hypoperfusion on technetium-Tc99m-hexamethylpropyleneamine oxime single-photon emission tomography have also been demonstrated in women with toxemia of pregnancy, a condition with clinical features similar to PRES and hypertensive encephalopathy.13
The development of infarction is further evidence for vasoconstriction as a common mechanism of choroidopathy and PRES in our patients. In our case 1, the visual cortex on 1 side became infarcted. In our case 2, there were residual Elschnig spots in both eyes, reflecting multifocal RPE infarctions. Infarction has been previously reported in PRES,4 a phenomenon less likely to occur if vasodilation was the mechanism.
If serous retinal detachment and PRES share the same mechanism, why has serous detachment not been reported before in PRES? We speculate that this retinal abnormality has been overlooked because it may present asymptomatically.
Acknowledgments
The authors wish to thank Robert Prusak, Department of Photography, W.K. Kellogg Eye Center, for his assistance with photographs.
Footnotes
-
Paper previously presented at: Annual Meeting of the North American Neuro-Ophthalmology Society, March 6–11, 2010; Tucson, Arizona.
References
- Received September 28, 2010.
- Accepted after revision October 14, 2010.
- © 2011 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.