
Abstract
BACKGROUND AND PURPOSE: Few data are available on the frequency and location distribution of fenestrations of intracranial arteries. We used 3D rotational angiography of all intracranial arteries in a cohort of 179 patients with suspected intracranial aneurysms to assess the prevalence and location of fenestrations and the relation of fenestrations to aneurysms.
MATERIALS AND METHODS: Of 179 patients with subarachnoid hemorrhage admitted between March 2013 and June 2014, 140 had 3D rotational angiography of all cerebral vessels. The presence and location of aneurysms and fenestrations were assessed. In patients with both aneurysms and fenestrations, we classified the relation of the location of the aneurysm as remote from the fenestration or on the fenestration.
RESULTS: In 140 patients, 210 aneurysms were present. In 33 of 140 patients (24%; 95% confidence interval, 17.2%–31.3%), 45 fenestrations were detected with the following locations: anterior communicating artery in 31 (69%), A1 segment of the anterior cerebral artery in 4 (9%), middle cerebral artery in 4 (9%), basilar artery in 4 (9%), vertebral artery in 1 (2%), and anterior inferior cerebellar artery in 1 (2%). Of 56 patients with anterior communicating artery aneurysms, 14 had a fenestration on the anterior communicating artery complex. The remaining 31 fenestrations had no anatomic relation to aneurysms. In 140 patients with 210 aneurysms, 14 aneurysms (7%) were located on a fenestration and 196 were not.
CONCLUSIONS: In patients with a suspected ruptured aneurysm, fenestrations of intracranial arteries were detected in 24% (33 of 140). Most fenestrations were located on the anterior communicating artery. Of 45 fenestrations, 14 (31%) were related to an aneurysm.
ABBREVIATION:
- AcomA
- anterior communicating artery
Fenestrations of intracranial arteries are segmental duplications of the lumen into 2 distinct channels, each comprising endothelial and muscular layers with or without a shared adventitia. Fenestrations are anatomic variants and can range from a small focus of divided tissue to duplication of a long vessel segment.1,2
Fenestrations result from partial failure of fusion of paired primitive embryologic vessels or from incomplete obliteration of anastomosis in a primitive vascular network.2
The association of fenestrations with aneurysms and other neurovascular disorders has been noted. Some suggest that altered flow dynamics in the presence of fenestrations may promote aneurysm development, though the exact relationship is not well-defined.
Surgical and anatomic studies suggest that fenestrations are common in intracranial arteries with the highest prevalence in the anterior communicating artery (AcomA) complex.3⇓–5 Demonstration of fenestrations with imaging is uncommon.6,7 Most fenestrations are only visible from a specific viewing angle that is often not provided by conventional angiography or reconstructed cross-sectional imaging. With 3D imaging, especially 3D rotational angiography, the detection rate of fenestrations has improved.8 Scant data are available on the frequency and location distribution of fenestrations of intracranial arteries, to our knowledge. We used 3D rotational angiography of all intracranial arteries in a cohort of 179 patients with suspected intracranial aneurysms to assess the prevalence and location of fenestrations and the relation of fenestrations with aneurysms.
Materials and Methods
Patient Population
The institutional review board approved this prospective study with a waiver for informed consent. Between March 2013 and June 2014, 179 patients with acute SAH were admitted. The diagnosis of SAH was established with a native CT scan or lumbar puncture. Of 179 patients, 177 had CTA as the first diagnostic imaging technique, and 2 patients proceeded to angiography without CTA because of poor renal function. CTA was not followed by angiography in 37 patients because of a perimesencephalic hemorrhage pattern (n = 18), a moribund clinical condition (n = 10), or trauma and SAH (n = 9). In the remaining 140 patients, CTA was followed within 24 hours by 3D rotational angiography of 3 vessels. These 140 patients form the present study group.
3D Rotational Angiography
Angiography was performed on a biplane angiographic system (Allura Xper FD20/10; Philips Healthcare, Best, the Netherlands) by 1 of 3 interventional neuroradiologists (W.J.v.R., M.S., and J.P.P. with 26, 24, and 8 years of experience, respectively). In 80 (57%) uncooperative or intubated patients, angiography was performed with the patient under general anesthesia. A single 3D rotational angiographic run was acquired of both internal carotid arteries and 1 vertebral artery with a hand injection of 12–20 mL of contrast material. When the contralateral distal vertebral artery was not visualized, an additional 2D biplane run was performed of this vessel. The tube rotation arc was 240° with a rotation time of approximately 4.0 seconds. The rotational angiographic data were transferred to an independent workstation (Integris 3DRA Workstation; Philips Healthcare) for instant generation of 3D reformatted images in a 2563 matrix.
When possible, angiography was followed immediately by endovascular treatment with the patient under general anesthesia. Patients with aneurysms not suitable for coiling were scheduled for surgery.
Image Analysis
3D reformatted images were reviewed on the workstation by 2 observers in consensus (W.J.v.R. and S.B.T.v.R. with 26 and 3 years' experience in neuroradiology). Presence, location, and size of the aneurysms were recorded in a database. Other vascular disorders that might be responsible for the subarachnoid hemorrhage, such as arterial dissections, arteriovenous malformations, dural fistula, Moyamoya phenomenon, or reversible vasospasm syndrome, were separately recorded.
The presence and location of fenestrations was assessed. In patients with both aneurysms and fenestrations, we classified the relation of the location of the fenestration with the location of the aneurysm as remote from the fenestration or on the fenestration itself.
Data Analysis
Descriptive statistics were used for the presence, size, and locations of aneurysms and the frequency and locations of fenestrations. The sex distribution in patients with and without fenestrations was compared. In patients with and without intracranial aneurysms, the proportion of patients with a fenestration was compared with those without a fenestration. For comparison of proportions, the χ2 test was used.
Results
Patients
Of 140 patients with SAH and 3D rotational angiography of 3 vessels, 100 were women (71%) and 40 were men (29%), with a mean age of 58.0 years (median, 59 years; range, 27–84 years).
Aneurysms
In 140 patients, 213 aneurysms were detected. Twenty patients (14%) had no aneurysms; 68 patients had 1 aneurysm; 24 patients, 2 aneurysms; 16 patients, 3 aneurysms; 11 patients, 4 aneurysms; and 1 patient, 5 aneurysms. Of 120 patients with aneurysms, 52 (43%) had multiple aneurysms.
Aneurysm locations were the anterior communicating artery in 56, middle cerebral artery in 51, posterior communicating artery in 29, basilar tip in 15, carotid cavernous sinus in 12, superior cerebellar artery in 10, posterior inferior cerebellar artery in 8, internal carotid bifurcation in 7, pericallosal artery in 5, anterior choroidal artery in 4, supraclinoid carotid dissection in 4, vertebral junction in 3, posterior cerebral artery in 2, carotid ophthalmic artery in 2, anterior cerebral artery in 1, and anterior inferior cerebellar artery in 1.
Fenestrations
On 3D rotational angiography, 45 fenestrations were detected in 33 of 140 patients (24%; 95% confidence interval, 17.2%–31.3%). Examples are provided in the Figure. Eleven patients had 2 fenestrations, and 1 patient had 3 fenestrations. Location distribution was as follows: the AcomA in 31 (69%), A1 segment of the anterior cerebral artery in 4 (9%), middle cerebral artery in 4 (9%), basilar artery in 4 (9%), vertebral artery in 1 (2%), and anterior inferior cerebellar artery in 1 (2%). Of 45 fenestrations, 39 (87%) were located in the anterior circulation, and 6 (13%), in the posterior circulation. Of 33 patients with fenestrations, 7 were men (21%) and 26 were women (79%). Sex distribution did not differ between patients with and without fenestrations.
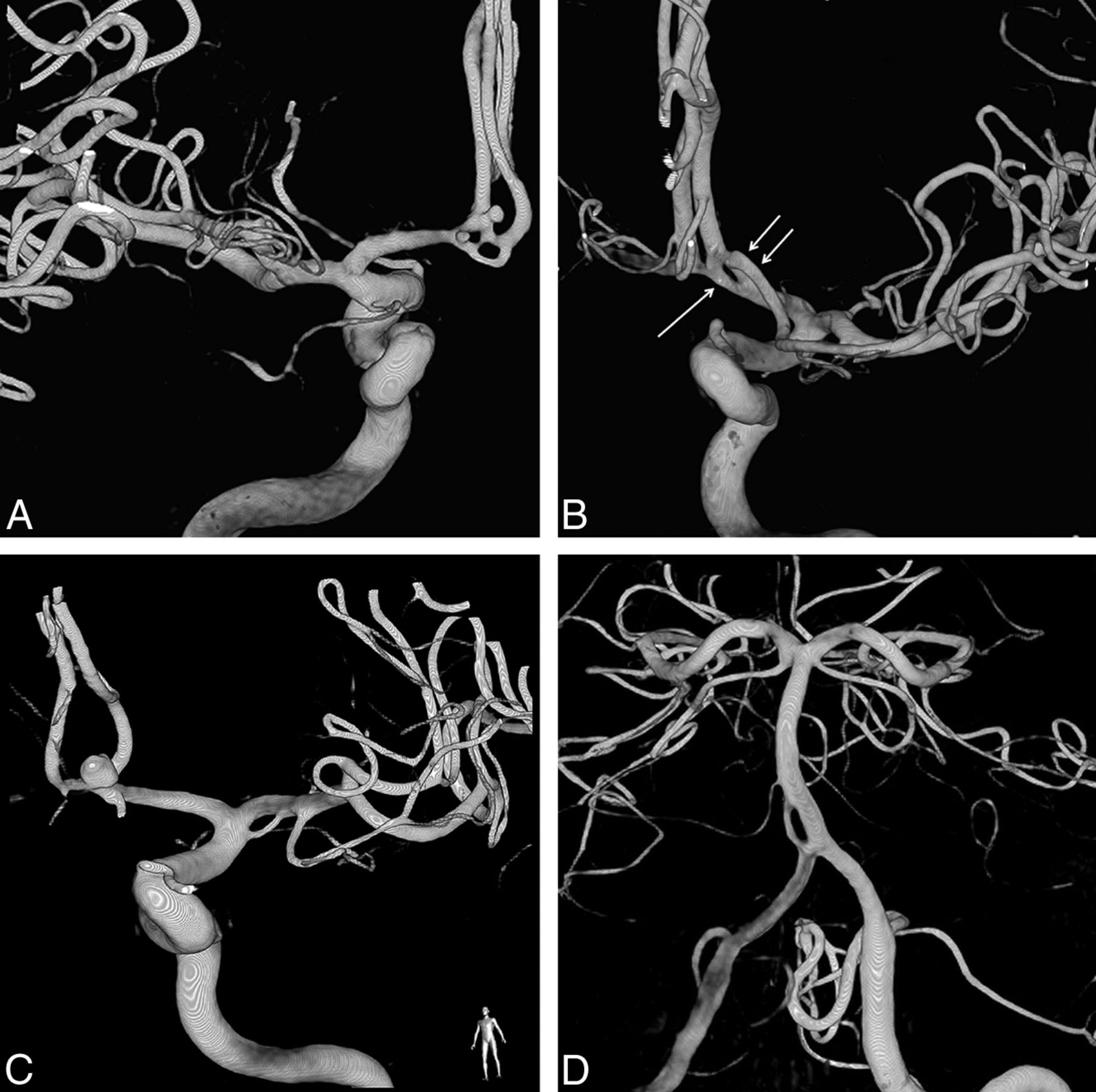
Examples of fenestrations of intracranial arteries. A, Double-fenestrated anterior communicating artery with 2 small aneurysms. B, Fenestration on the anterior communicating artery (arrow). Note the aberrant origin of a duplicated middle cerebral artery from A2 (double arrow). C, A small fenestration on the middle cerebral artery. D, A proximal basilar fenestration.
Relation of Fenestrations to Aneurysms
Of 56 patients with an AcomA aneurysms, 14 (25%) had a fenestration on the AcomA complex. The remaining 31 fenestrations had no anatomic relation with aneurysms. In 140 patients with 210 aneurysms, 14 aneurysms (7%) were located on or adjacent to a fenestration and 196 (93%) were not.
Forty-one fenestrations were present in 30 of the 120 patients (25%) with aneurysms, and 4 fenestrations were present in 3 of the 20 patients (15%) without aneurysms. This difference was not significant (P = .49).
Discussion
We found that fenestrations are common anatomic variations of intracranial arteries with a frequency of 24% in a cohort of 140 patients with suspected ruptured aneurysms. There was no significant difference in the occurrence of fenestrations in 120 patients with and 20 patients without aneurysms. We used optimal 3D rotational angiography imaging of all cerebral vessels in the clinical setting of patients with subarachnoid hemorrhage with intended endovascular treatment of aneurysms. Most 3D angiography was performed with the patient under general anesthesia, thereby eliminating image degradation by patient motion. These 3D images acquired under optimal circumstances were scrutinized by 2 experienced readers for the presence of fenestrations. Thus, data are robust, and the assessed frequency of fenestrations is likely to be realistic.
The only limitation of the study is that the patient population is a selection of those with subarachnoid hemorrhage with a much higher incidence of intracranial aneurysms than that in the general population. The high frequency of fenestrations may, therefore, not be generalized. Postmortem studies with a large sample size may resolve this issue but are currently not available.
Although almost a third of fenestrations had an anatomic relation to an aneurysm, these were all AcomA aneurysms on AcomA fenestrations. This observation may be expected in the given patient population with suspected aneurysms because most fenestrations and most aneurysms occurred on the AcomA. A definite association between aneurysms and fenestrations on this location remains unclear from our data.
This study confirms the common occurrence of fenestrations that was found in a previous study using 3D rotational angiography in patients with intracranial aneurysms.8 In that study, 3D rotational angiography was performed in only 1 cerebral vessel territory following detection of an aneurysm with 2D angiography. In the present study, all cerebral vessels were imaged in 3D, so data are more robust. Despite this methodologic difference, fenestrations were more frequent in the previous study than in the present study (28%, 59 of 208 patients versus 24%, 33 of 140 patients). With the relatively small sample sizes of both studies, the difference might be within the confidence limits. In both studies, the AcomA complex was the most common location of fenestrations and most fenestrations occurred in the anterior circulation.
Until recently, before the era of 3D imaging, fenestrations were considered a rarity. This might be because fenestrations are only visible from specific viewing angles that are mostly not available on 2D angiograms. In a recent study of almost 11,000 angiograms, fenestrations were identified in 2.1%, with the highest prevalence in the posterior circulation, especially the basilar artery.7 Also in another recent review of intracranial fenestrations with associated aneurysms, the most common single fenestration location was the basilar artery.9 With modern 3D reconstructions of axial images of CT and MR angiography, the prevalence was somewhat higher, up to 13%.10⇓⇓⇓–14 Large-vessel fenestrations such as those on the proximal basilar artery are readily depicted with 2D angiograms or CT and MR angiography, but resolution is insufficient to detect subtle small-vessel fenestrations such as in the AcomA complex.15
Many studies have noted the presence of fenestrations in the setting of a variety of neurovascular pathology apart from aneurysms, such as dissections, arteriovenous malformations, dural fistula, and even ischemic stroke. This may not be surprising because cerebral angiography is performed exclusively in patients with suspected intracranial vascular disease. A causative relation of fenestrations with neurovascular disorders has never been firmly established. On the contrary, recent studies with more frequent depiction of fenestrations including the present study suggest that a relation to aneurysms or other vascular pathology is not very likely.7,8,10 Only large postmortem studies can provide a definite answer to this issue.
Conclusions
In patients with a suspected ruptured aneurysm, fenestrations of intracranial arteries were detected in 24% (33 of 140). Most fenestrations were located on the AcomA. Of 45 fenestrations, 14 (31%) were related to an aneurysm.
References
- Received November 13, 2014.
- Accepted after revision December 1, 2014.
- © 2015 by American Journal of Neuroradiology





{kind=link}