
Abstract
SUMMARY: CSF-venous fistula is an important treatable cause of spontaneous intracranial hypotension that is often difficult to detect using traditional imaging techniques. Herein, we describe the technical aspects and diagnostic performance of MR myelography when used for identifying CSF-venous fistulas. We report 3 cases in which the CSF-venous fistula was occult on CT myelography but readily detected using MR myelography.
ABBREVIATIONS:
- CVF
- CSF-venous fistula
- SIH
- spontaneous intracranial hypotension
- VIBE
- volumetric interpolated brain examination
CSF-venous fistula (CVF) is an important cause of spontaneous intracranial hypotension (SIH) and a critical diagnosis because treatment can result in a clinical cure.1-5 The fistulous connection is typically associated with a nerve root sleeve diverticulum; therefore, a detectable epidural fluid collection is often absent. Some authors advocate decubitus CT myelography to improve CVF detection,1,2,6 while others suggest that digital subtraction myelography may increase rates of fistula identification.7,8 We report surgically confirmed cases of CVF that were identified using MR myelography following the intrathecal administration of gadolinium.
MR Myelography Technique
Intrathecal gadolinium was instilled in the subarachnoid space via CT-guided lumbar puncture using a Gertie Marx Whitacre-style spinal needle (IMD). The opening pressure was measured and recorded, and 0.5 mL of gadobutrol (Gadavist; Bayer Schering Pharma) mixed with 4.5 mL of iohexol (Omnipaque 180; GE Healthcare) was intrathecally administered. After a 1-mL test injection, CT imaging confirmed intrathecal contrast, and 5 mL was instilled before the needle was removed with the stylet in place. The patient was positioned in a decubitus Trendelenberg position and rolled multiple times to disperse contrast throughout the subarachnoid space. The patient was then transferred to the MR imaging suite where MR myelography was performed on a 3T Biograph mMR scanner (Siemens) using multiplanar fat-suppressed T1 sequences (On-line Table). Imaging was reviewed in real time, and delayed thin-section axial sequences were acquired as needed. MR imaging was completed approximately 1 hour after intrathecal gadolinium administration.
Cases
Case 1.
A 26-year-old woman with a 3-year history of orthostatic headaches after a spontaneous onset had brain MR imaging findings characteristic of SIH, including sagging, pituitary enlargement, venous distention, small subdural collections, and pachymeningeal enhancement. A CT myelogram was unrevealing for CSF leak, and 3 epidural blood patches were unsuccessful. She subsequently developed upper extremity pain and paresthesias, leading to the discovery of a large cervicothoracic syrinx on cervical spine MR imaging (Fig 1). She was treated with a posterior fossa decompression to improve craniocervical CSF flow but obtained neither symptom nor imaging improvement. Eventually, she underwent MR myelography with an opening pressure of <4 cm H2O and was discovered to have a prominent left T7–T8 spinal meningeal diverticulum fistulizing to a left paraspinous vein draining into the azygous system. She also had early contrast opacification of her renal collecting system on the MR myelography completed approximately 1 hour after intrathecal contrast injection (Fig 2). The patient was offered and accepted surgical CVF ligation at T7–T8. The diverticulum was identified with dilated draining veins, and the entire nerve root complex with the CVF was interrupted with an aneurysm clip and silk suture (On-line Fig 1). The patient experienced an immediate improvement in symptoms followed by a transient new headache and sixth-nerve palsy 3 days following the operation. This was presumed to be secondary to transient rebound intracranial hypertension, and her symptoms slowly resolved. Eight months postoperatively, she is without headaches, and follow-up MR imaging revealed both a dramatic resolution of brain sagging and near-complete resolution of the spinal cord syrinx (Fig 1).
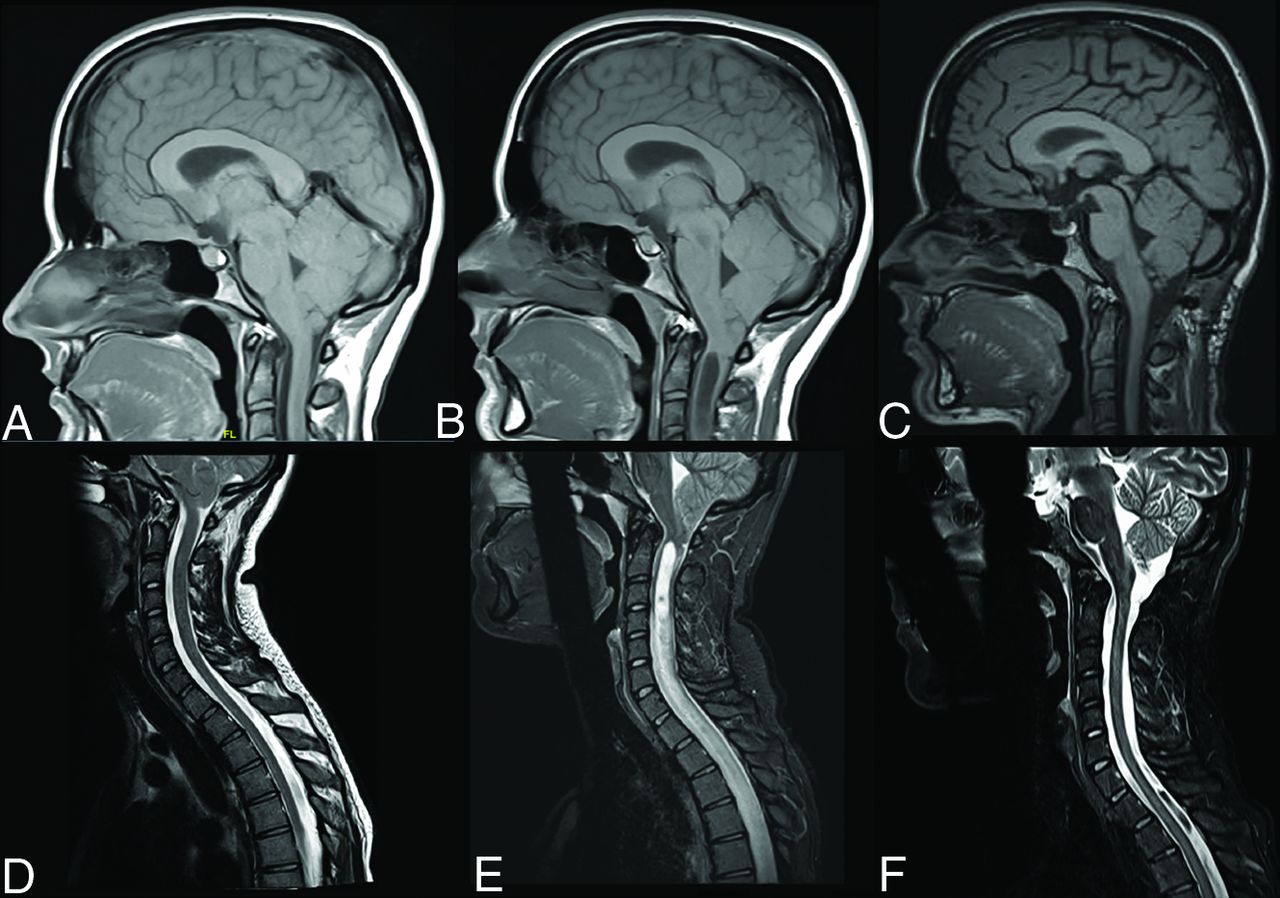
Sagittal T1 brain (A–C) and sagittal T2-weighted cervical spine (D–F) imaging. Initial MR imaging from June 2016 (A and D) shows classic intracranial findings of SIH with low-lying cerebellar tonsils, effacement of the prepontine cistern, enlarged pituitary, and brain stem sagging. Spine imaging findings are normal. Follow-up MRIs from June 2018 (B and E) show similar brain findings with interval development of a large cervicothoracic syrinx. Postoperative MRIs from June 2019 (C and F) reveal complete resolution of intracranial SIH sequelae, with a normal position of the cerebellar tonsils and resolution of spinal syrinx.

MR myelogram axial T1 VIBE (A) demonstrates early contrast opacification of the renal collecting system (dashed circles). CT myelogram (B) demonstrates an irregular left T7–T8 perineural cyst without evidence of an opacifying paraspinal vein. No renal contrast excretion was identified on CT myelography. MR myelogram axial T1 VIBE (C) shows a spinal meningeal diverticulum with an opacifying paraspinal vein (arrows) draining into the azygous system, consistent with a CSF-venous fistula.
Case 2.
A 64-year-old man presented with a 9-month history of orthostatic headache, distorted hearing, and tinnitus with onset during Valsalva exacerbated by severe constipation. Brain imaging demonstrated a venous distention sign without other intracranial sequelae of SIH. Standard CT myelography could not identify a CSF leak, and multiple epidural blood patches were unsuccessful. An MR myelogram with an opening pressure of 9 cm H2O revealed a left T8–T9 spinal meningeal diverticulum and adjacent opacification of a paraspinous vein (Fig 3). Small-volume contrast was also seen in the renal collecting systems. The patient was offered and accepted surgical CVF ligation at T8–T9. The diverticulum was identified with dilated draining veins, and the entire nerve root complex with the CVF was interrupted with an aneurysm clip and silk suture. The patient experienced marked symptomatic improvement with resolution of headache and tinnitus, sustained at the most recent 4-month follow-up visit.
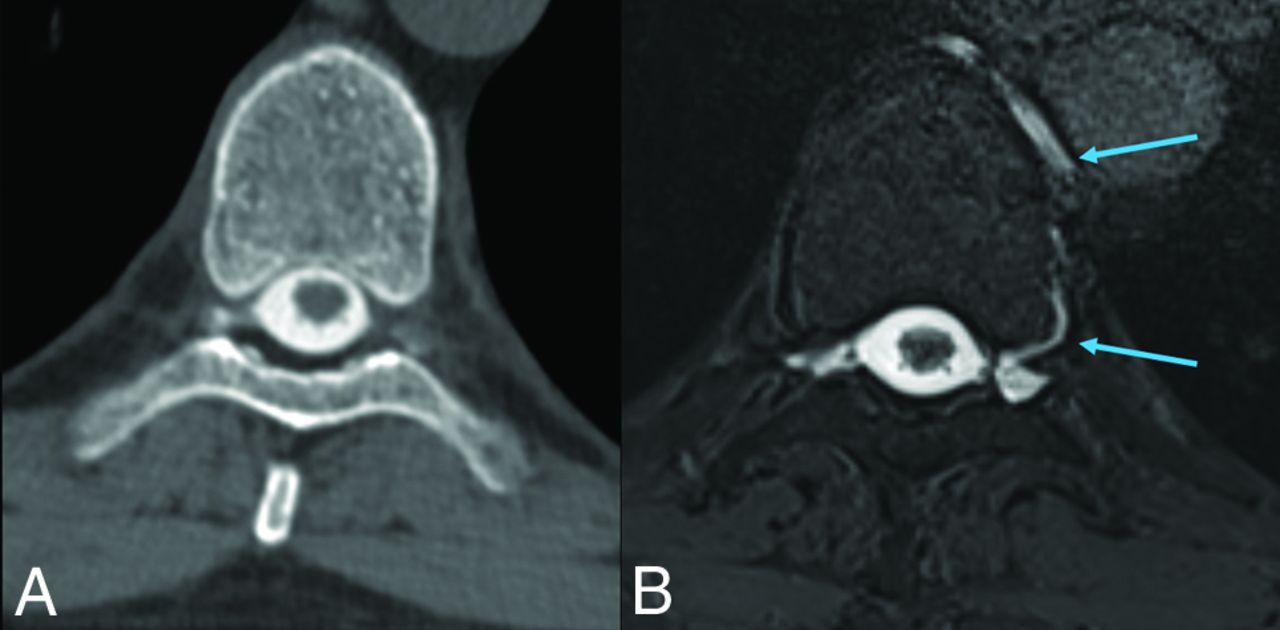
CT and MR myelogram images from case 2. A, CT myelogram reveals perineural cysts at T8–T9 without opacification of the left-sided cyst. B, MR myelogram axial T1 VIBE demonstrates opacification of the left-sided spinal meningeal diverticulum and left paraspinal vein draining into the azygous system (arrows), consistent with a CSF-venous fistula.
Case 3.
A 53-year-old woman presented with a 2-year history of spontaneous-onset orthostatic headache and neck pressure. Brain imaging findings were suspicious for SIH with sagging, pituitary enlargement, venous distention, small subdural collections, and pachymeningeal enhancement. A CT myelogram revealed multiple spinal meningeal diverticula and Tarlov cysts without evidence of spinal fluid leak, and the patient received multiple epidural blood patches with only transient improvement of symptoms. An MR myelogram with an opening pressure of <4 cm H2O revealed a left T9–T10 spinal meningeal diverticulum and an opacified left paraspinous vein (On-line Fig 2). The patient was offered and accepted surgical CVF ligation at T9–T10. The diverticulum was identified with dilated draining veins, and the entire nerve root complex with the CVF was interrupted with an aneurysm clip and silk suture. The patient reported an immediate improvement in symptoms with return to baseline and resolution of headache, sustained for 7 months at the most recent follow-up visit.
DISCUSSION
CSF-venous fistulas are an under-recognized cause of SIH. Improved detection using advanced imaging techniques may increase our sensitivity in detecting CSF leaks. CT myelography may detect CVF, and the technique can be augmented with decubitus positioning and provocative maneuvers to increase CSF pressure.5,9 Digital subtraction myelography has also been used to identify CSF-venous fistulas. However, both of these techniques require substantial ionizing radiation exposure to the patient, and the digital subtraction myelography technique is operator-dependent with different techniques described in the literature.7,8 Intrathecal administration of gadolinium is an off-label use in the United States but is well-tolerated and frequently used for clinical and research applications.10,11 However, while no long-term harmful effects from intrathecal gadolinium are known, this has not been extensively studied. Only a macrocyclic gadolinium agent (gadobutrol) was used in this study, which has a weaker association with deposition compared with linear gadolinium agents.12 MR myelography eliminates the ionizing radiation exposure aside from any used for lumbar puncture. Additionally, multiple imaging sequences can be repeated as necessary to confirm a suspected fistula. Furthermore, while the attenuation of intrathecal CT contrast fades rapidly within an hour of intrathecal administration, intrathecal gadolinium maintains robust T1-shortening MR imaging signal for hours after administration. We found the axial T1 fat-suppressed volumetric interpolated brain examination (VIBE) imaging sequences to be particularly helpful. These may help highlight a fistula on MR myelography that may be less apparent on other imaging modalities. The technique is further bolstered by the improved soft-tissue contrast of MR imaging and the prominent signal intensity of gadolinium on fat suppressed T1-weighted images. MR myelography has been shown previously to detect leaking gadolinium from perineural cysts.13
Outstanding questions remain regarding the diagnostic performance of MR myelography and other myelographic techniques in the detection of CVF because no known criterion standard is available. We report 3 patients who had unrevealing CT myelograms in whom CVF was detected on MR myelography, all of whom experienced marked clinical improvement following ligation of the suspected fistula. This report raises important questions for further study regarding the optimal technique for imaging patients with suspected CSF leak.
In conclusion, MR myelography with intrathecal gadolinium may identify CSF-venous fistulas in patients without readily apparent fistulas on CT myelography. Further study is needed to confirm these promising findings.
Footnotes
Disclosures: Dr. Chazen—RELATED: Grant: Insightec, Inc., Alzheimer's Drug Discovery Foundation.
References
- Received December 25, 2019.
- Accepted after revision February 29, 2020.
- © 2020 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Spinal CSF Leaks: The Neuroradiologist Transforming Care
- Spontaneous Intracranial Hypotension in Children: A Multi-Institutional Review of Spinal CSF Leaks Localized on Advanced Myelography
- Different Glymphatic Kinetics in Spontaneous Intracranial Hypotension
- Myelographic Techniques for the Localization of CSF-Venous Fistulas: Updates in 2024
- Temporal Characteristics of CSF-Venous Fistulas on Digital Subtraction Myelography
- Resisted Inspiration: A New Technique to Aid in the Detection of CSF-Venous Fistulas
- Multiple Spinal CSF Leaks in Spontaneous Intracranial Hypotension: Do They Exist?
- Spinal CSF-Venous Fistulas in Morbidly and Super Obese Patients with Spontaneous Intracranial Hypotension
- Decubitus CT Myelography for CSF-Venous Fistulas: A Procedural Approach