Abstract
Summary: Persistent proatlantal artery type 1 is one of the four anastomotic vessels between the carotid and vertebrobasilar arterial systems. Persistence of this embryonic anastomosis is extremely rare. We present such a case with bilateral persistent proatlantal arteries that arose from internal carotid arteries, entered the skull via the foramen magnum and united with the horizontal portions of vertebral arteries. We also mention its embryology, potential clinical implications, and differentiating features between two types of proatlantal arteries.
Persistence of fetal anastomoses between carotid and vertebrobasilar arteries is a well-known anomaly, although bilateral persistence of these anastomoses is rare. To the best of our knowledge, only three cases have been reported with persistent bilateral type 1 or type 2 proatlantal arteries in the literature (1–3). Just a single case has bilateral type 1 proatlantal arteries (3). We present a case of persistent bilateral type 1 proatlantal arteries with absence of the vertebral arteries.
Case Report
A 55-year-old man had been complaining of left-sided weakness and numbness for 6 weeks. Neurologic examination revealed left-sided hemihypoesthesia and indistinctness of left nasolabial sulcus. Cerebral CT imaging showed bilateral periventricular white matter hyperlucencies and lacunar infarcts. Six days later, MR angiography (MRA) of the supraaortic vessels was performed (2D time of flight), which showed absence of both vertebral arteries at their origin.
The horizontal portion of vertebral arteries were constituted by two vessels originating from the internal carotid arteries bilaterally (Fig 1). Selective catheterization of both common carotid arteries confirmed the findings of the MRA. An aortic arch arteriogram revealed absence of the vertebral arteries bilaterally (Fig 2). Evaluation of right carotid system demonstrated the origin of anastomostic vessel from the internal carotid artery at the level of the C2 vertebra. The vessel coursed superiorly until the atlantooccipital junction and continued dorsally before entering the skull through foramen magnum (Fig 3). Evaluation of the left carotid system showed a smaller vessel originating from the internal carotid artery at the level of C2 vertebra. This vessel also coursed superiorly and entered skull through foramen magnum after proceeding dorsally (Fig 4). The basilar artery and both posterior cerebral arteries were supplied by these vessels, especially by the dominant right one. Atherosclerotic plaques were present at the proximal portion of both internal carotid arteries and right persistent proatlantal artery. They probably were the source of the emboli causing the neurologic symptoms we have described.

MR angiogram (2D time of flight). Right proatlantal artery originating from internal carotid artery can be seen in its full course (arrows), but only the proximal portion of left proatlantal artery can be seen (arrowhead).
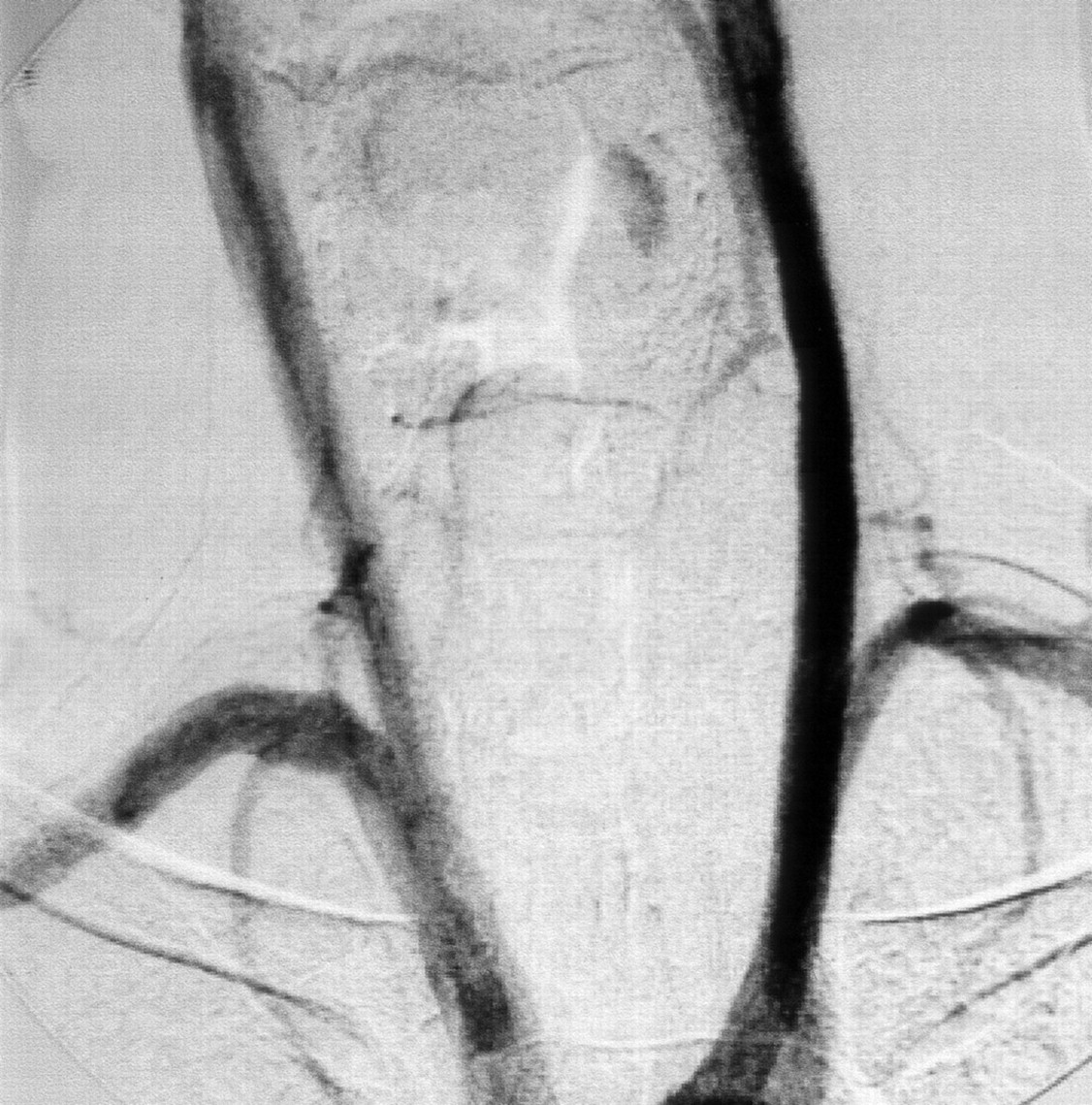
Aortic arch angiogram, showing the absence of both vertebral arteries.

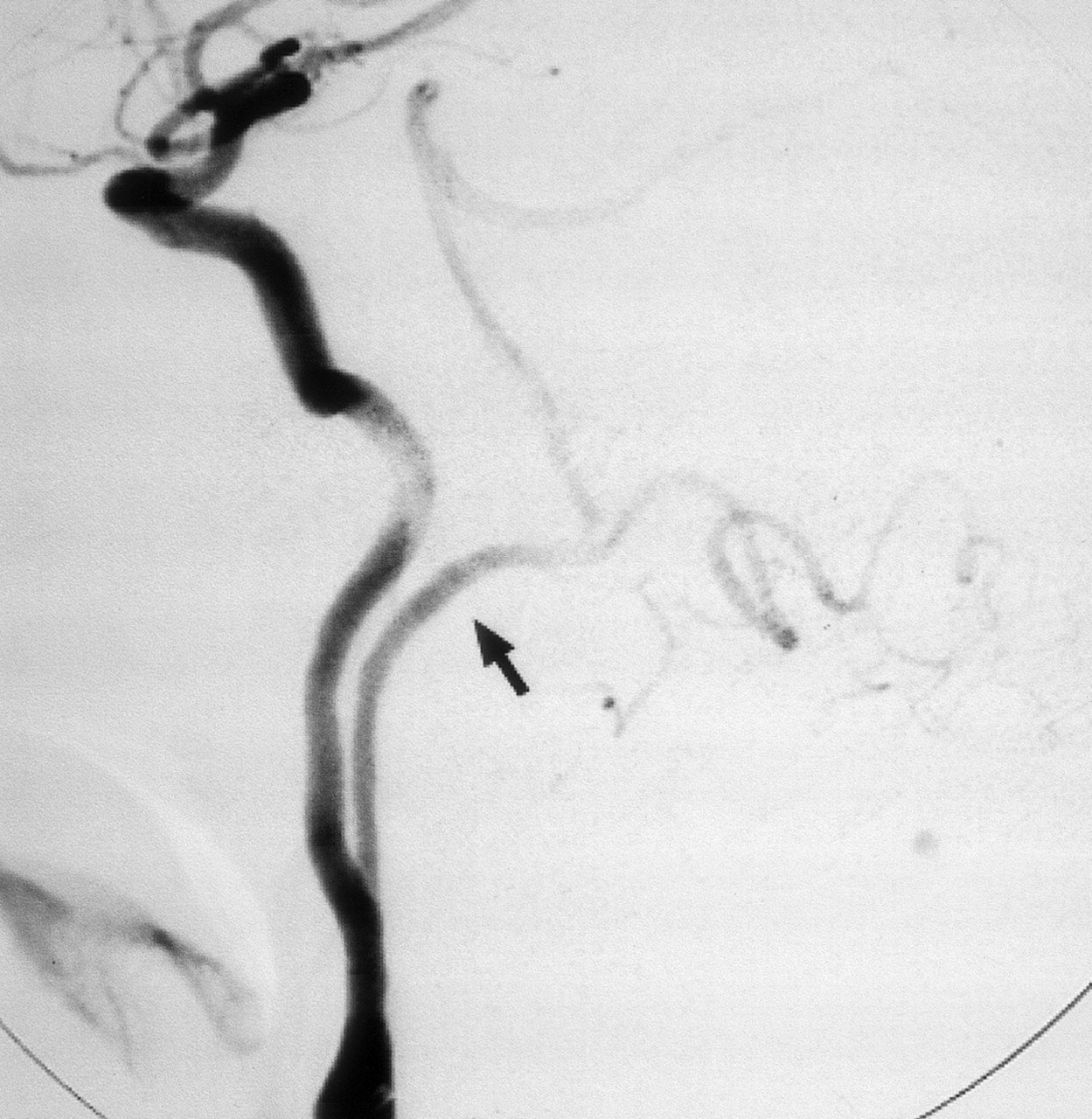
Right common carotid artery digital subtraction arteriogram, lateral projection. Proatlantal artery (arrow) originates from the internal carotid artery. The vessel extends to the posterior aspect of atlas with a horizontal sweep characteristic of a type 1 proatlantal artery (arrowhead) before turning upward to join the horizontal segment of the vertebral artery.
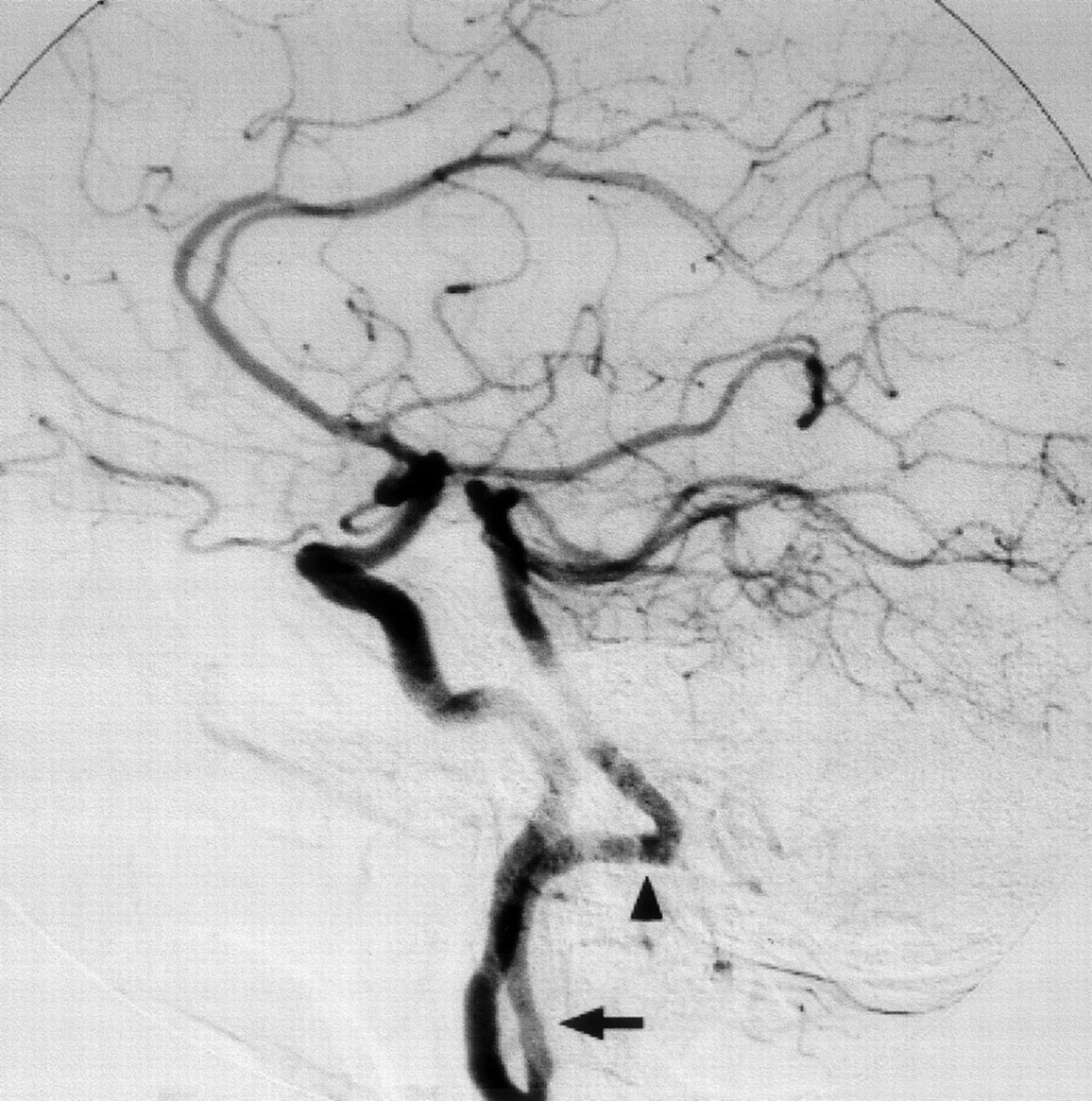
Left common carotid artery digital subtraction arteriogram, lateral projection. Proatlantal artery (arrow) courses dorsally above C1 before joining the vertebral artery.
Discussion
At the 4–5-mm embryonic stage, the hindbrain is supplied by two parallel neural arteries. These two neural arteries supply blood from the carotid system via trigeminal, otic, hypoglossal, and proatlantal arteries (4, 5).
As the posterior communicating arteries develop, three of the four anastomoses—otic, hypoglossal, and trigeminal arteries—regress (6). The life span of these arteries is about a week. The proatlantal arteries persist until the vertebral arteries develop. During the 7 to 12 mm embryonic stage, the vertebral arteries are formed from transverse anastomoses between adjacent cervical intersegmental arteries, beginning with the proatlantal intersegmental artery and proceeding downward to the C6 intersegmental artery, which forms the origin of adult vertebral artery and subclavian artery (7). Part of the proatlantal artery becomes the horizontal portion of the vertebral artery (4; Fig 5). The horizontal and distal portions of occipital artery are also derived from the proatlantal artery (8).

A, At the 4–5-mm embryonic stage bilateral longitudinal neural arteries (arrows)—one set of longitudinal neural arteries, dorsal aorta, and cervical intersegmental arteries is shown—are supplied by trigeminal artery (TA), otic artery (OA), hypoglossal artery (HA), proatlantal intersegmental artery (PA), and cervical intersegmental arteries (CIA1–6)
B, At the 7–12-mm embryo vertebral artery (VA) develops through the transverse anastomoses between adjacent cervical intersegmental arteries and distal part of the proatlantal artery becomes the horizontal portion of the vertebral artery (arrowheads) while proximal part regresses completely. Failure of this regression results as persistent proatlantal artery (dashed lines). Also note that at this stage of embryo TA, OA, and HA has disappeared after development of posterior communicating artery (PCA). AA, fourth aortic arch; DAo, dorsal aorta; ECA, external carotid artery; ICA, internal carotid artery; VAo, ventral aorta.
When the proatlantal artery persists, the ipsilateral, contralateral, or both, vertebral arteries are hypoplastic in about half of the cases (9). Like the hypoglossal artery, the persistent proatlantal artery arises from the carotid system outside cranium and unites with the posterior vascular system inside cranium. Therefore, there are some difficulties in differentiating these two anastomoses. A higher origin is expected for hypoglossal artery. The hypoglossal artery usually leaves the internal carotid artery at the level of C1 vertebra or C1–C2 interspace. Origin of proatlantal artery at the C2 or C3 vertebra is typical (9).
Analysis of well-documented cases reveals two important differentiating features: 1) The suboccipital horizontal course is characteristic of vertebral and proatlantal arteries. The hypoglossal artery lacks this horizontal course. 2) The proatlantal artery enters the skull through the foramen magnum, whereas the hypoglossal artery enters the skull through the hypoglossal canal. Therefore, a small dorsal curve will be enough for hypoglossal artery, but the proatlantal artery extends much more posteriorly and horizontally.
Two types of proatlantal arteries have been described, both arising from the carotid artery and entering the foramen magnum (8). The type 1 proatlantal artery (proatlantal intersegmental artery) rises from the caudal internal carotid artery and ascends to the level of the occipitoatlantal space without passing through the transverse foramen of any cervical vertebra. The artery takes a dorsal course cephalad to the transverse process of C1 and then travels rostrally to enter the foramen magnum. The type 2 proatlantal artery (C1 intersegmental artery) arises from the external carotid artery laterally, remains more lateral in position than the type 1 artery, and joins the course of the horizontal portion of the vertebral artery before entering the foramen magnum (Fig 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A, Persistent proatlantal artery type I (PPA 1) arises from the caudal part of the internal carotid artery and courses along the anterior aspect of the vertebral bodies to the level of the occipitoatlantal space before coursing dorsally.
B, Persistent proatlantal artery type II (PPA 2) arises from the external carotid artery; it crosses the C1 or C2 vertebra obliquely. Both PPA-1 and PPA-2 enter the skull via the foramen magnum.
In the case reported here, the arteries arise from the internal carotid artery at the C2 level. They ascend to the level of transverse processes of C1 and course dorsally in the occipitoatlantal space. This suboccipital horizontal sweep is characteristic of proatlantal artery 1. They also extend farther posteriorly than would be expected of hypoglossal artery. Thereafter, they enter the skull through the foramen magnum bilaterally and combine with the horizontal segment of vertebral artery to form the basilar artery.
As in our case, most of the proatlantal arteries are incidentally found. Associated vascular anomalies are more common with persistent primitive anastomoses, although neither the reported persistent bilateral proatlantal artery cases nor our case was associated with such an anomaly. It can be theorized that persistence of carotid-basilar anastomoses relate to a teleologic effort to preserve blood flow to the posterior fossa compromised by hypoplastic or nonexistent vertebral arteries. Also environmental, mechanical, and genetic factors before the 14-mm stage of the embryo may cause predisposition to multiple vascular anomalies (10). It is important for the surgeon to be aware of these primitive anastomoses while performing endarterectomy (11) or ligation of the external carotid artery. If the anomalous vessel is the only source for posterior circulation and there is stenosis or occlusion in the carotid system, symptoms of posterior fossa ischemia may ensue. Furthermore, interventional neuroradiologic procedures may require modification if such anomalies exist.
References
- Received December 8, 2003.
- Accepted after revision February 2, 2004.
- Copyright © American Society of Neuroradiology