Abstract
BACKGROUND AND PURPOSE: The purpose of this study was to review the imaging findings of nasal septal abscess in 2 patients with immunosuppression.
MATERIALS AND METHODS: Two patients with immunosuppression were identified as having a nasal septal abscess, and correlative CT imaging in both patients was evaluated.
RESULTS: The characteristic radiographic appearance of a nasal septal abscess included a fluid collection with thin rim enhancement, located within the cartilaginous nasal septum. After CT examination, incision and drainage was performed in both patients, and appropriate antibiotic coverage was initiated. Clinical and imaging follow-up demonstrated no signs of residual infection.
CONCLUSION: Nasal septal abscess has a characteristic appearance on CT examination. Prompt diagnosis and treatment, including incision and drainage and appropriate antibiotic coverage, are necessary to avoid serious complications.
Nasal septal abscess is defined as a collection of purulent material between the cartilaginous or bony septum and the mucoperichondrium or mucoperiosteum.1 Nasal septal abscesses occur more commonly after minor nasal trauma1 but may also result from iatrogenic causes2 and sinonasal3 or dental infection.4 After minor nasal trauma, a hematoma may form secondary to the rupture of small blood vessels in the nasal septum. The hematoma separates the mucoperichondrium from the septal cartilage and forms an ideal medium for the colonization and growth of bacteria, leading to the formation of an abscess.1
Serious complications may occur as a result of the nasal septal abscess, especially in patients with immunosuppression. The purpose of this study was to review the imaging findings of nasal septal abscess in 2 such patients to assist radiologists to identify this uncommon, but serious infection.
Materials and Methods
Two patients were identified with imaging consistent with a nasal septal abscess. Both patients had immunosuppression and were undergoing chemotherapy. The diagnosis of nasal septal abscess was suspected clinically by history and physical examination. The initial imaging, which was performed less than 1 day before the incision and drainage, included a CT examination in both patients. In patient 1, a CT examination of the head and neck was performed. In patient 2, a CT examination of the head and neck was requested, as per the physician's note; however, a CT of the brain was inadvertently performed. Follow-up imaging also included CT imaging in both patients.
Patient 1 was a 76-year-old man with acute myelogenous leukemia, which was diagnosed approximately 5 months before the development of the nasal septal abscess. He presented with a 3-week history of nasal stuffiness, difficulty with nasal breathing, headache, and facial pain. The patient's white blood cell count was 86.7 K/μL at presentation. Nasal soft tissue swelling was present on physical examination.
Anterior rhinoscopy was performed, which demonstrated fluctuant enlargement of the nasal septum bilaterally, suggesting a septal abscess. Aspiration of both the right and left nasal septa was performed with an 18-gauge needle; 8 mL of purulent discharge was obtained on both sides. CT scanning of the maxillofacial region was performed on a GE scanner (LightSpeed; GE Healthcare, Milwaukee, Wis), after intravenous administration of contrast material.
Patient 2 was a 17-year-old adolescent boy with a history of T-cell lymphoblastic lymphoma in complete remission. The patient was on chemotherapy consisting of modified hyper-CVAD (fractionated cyclophosphamide, vincristine, Adriamycin, and dexamethasone). The patient reported a recent history of minor nasal trauma and complained of frequent blowing of the nose secondary to allergic rhinitis, and nasal tenderness for the previous 2 to 3 days. On clinical examination, there was a mild amount of edema and erythema over the dorsum of the nose with mild tenderness and the presence of a saddle deformity. The white blood cell count was elevated to 13.1 K/UL. Fiberoptic examination of the nasal cavity was performed, which revealed no evidence of asymmetry, erythema, or nasal discharge. Septal abscess was suspected because of the saddle deformity and nasal tenderness. CT examination of the brain with contrast was performed on a GE scanner (GE Healthcare) after administration of intravenous contrast material the next day.
Results
In both patients, CT imaging revealed a fluid collection with thin rim enhancement, located within the cartilaginous nasal septum (Fig 1 and Fig 2A). The nasal septal abscess was not originally detected on the CT examination of the brain in patient 2; however, it was present in retrospect. There were no associated solid components with the abscesses. Patient 1 had swelling of the adjacent nasal soft tissues. There was no bony destruction or evidence of osteomyelitis involving the adjacent bony nasal septum in either patient.
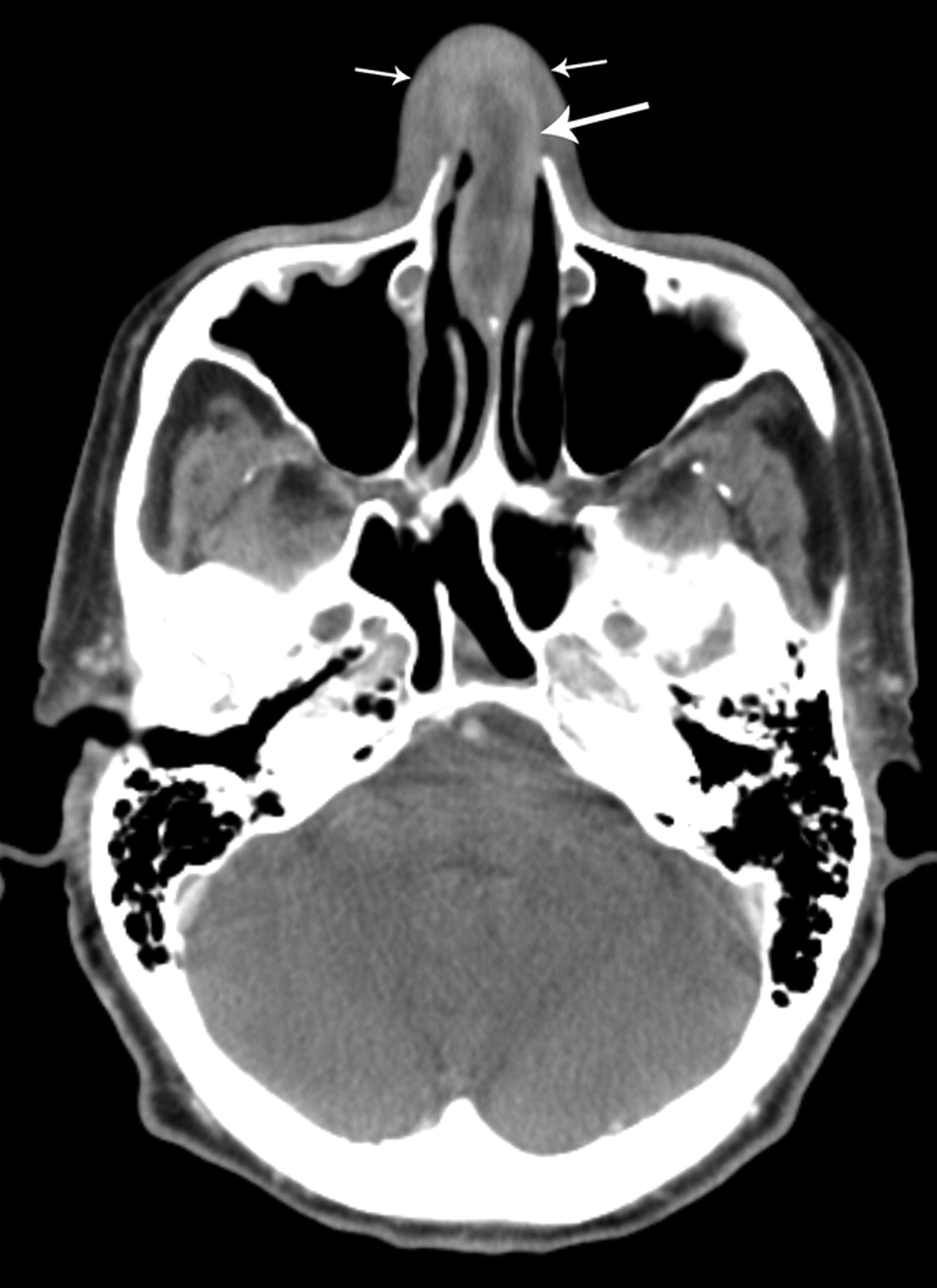
A 76-year-old man with acute myelogenous leukemia. CT imaging through the nasal cavity demonstrates a thin-walled, cystlike collection with peripheral enhancement involving the cartilaginous nasal septum (large arrow) consistent with a nasal abscess. There are no associated solid components. Note the swelling of the adjacent nasal soft tissues (small arrows).

{kind=link}
{kind=link}
A 17-year-old adolescent boy with T-cell lymphoblastic lymphoma. A, CT imaging of the brain demonstrates a subtle hypoattenuation of the cartilaginous nasal septum (arrows), found clinically to represent a nasal septal abscess. B, Resolution of nasal septal abscess after treatment.
After the CT examinations, an incision and drainage was performed on both patients. Collection of purulent material was sent to the laboratory for analysis and confirmed the diagnosis of an abscess. In patent 1, pathologic examination revealed evidence of acute inflammation and the presence of granulocytic sarcoma (chloroma). The patient was placed on Valacyclovir (Valtrex) and levofloxacin (Levaquin). Clinical and radiologic follow-up at approximately 2 months revealed no signs of residual infection. For patient 2, Gram stain and culture were performed, which identified the presence of Aspergillus flavus, which was treated with voriconazole. Clinical and radiologic follow-up at approximately 6 weeks revealed no signs of residual infection (Fig 2B).
Discussion
To our knowledge, no previous reports on the imaging appearance of nasal septal abscess in patients with immunosuppression have been published in the radiology literature. The imaging findings of nasal septal abscess, a thin-walled fluid collection with adjacent inflammatory change, are similar to those seen with abscesses located elsewhere within the body. Pang et al3 reported a case of nasal septal abscess as an unusual complication of acute spheno-ethmoiditis with similar imaging findings of a thin-walled, enhancing fluid collection involving the cartilaginous and bony septum.
Patients with a nasal septal abscess often present clinically with nasal obstruction. Less common symptoms include pain, rhinorrhea, fever, nasal fracture, bleeding, and cellulitis.5 Most patients have a history of at least minor trauma.2,5–7 Direct clinical inspection may reveal swelling and erythema of the dorsum of the nose and nasal septum as well as the presence of destroyed septal cartilage.2
Surgical drainage of the purulent contents of a nasal septal abscess is performed to relieve pressure and to provide a specimen for Gram stain, culture, and sensitivity. Nasal packing, the placement of a Penrose drain,3 reduction of nasal fractures, and delayed reconstruction of destroyed nasal cartilage2 may also be performed. The results of Gram stain and culture and sensitivity of the aspirate determine the appropriate systemic antibiotic coverage. The most common organism to be cultured is Streptococcus aureus.1,5 Other organisms include Streptococcus pneumoniae or Streptococcus viridans, Staphylococcus epidermidis, and Haemophilus influenzae.3,6
Early diagnosis and treatment are essential to prevent associated complications of the nasal septal abscess. These include sepsis, bacteremia, meningitis, brain abscess, cavernous sinus thrombosis, and maxillary hypoplasia.3,7,8 Destruction of cartilage may cause a depression of the nasal bridge from collapse of structural support leading to the formation of a saddle nose deformity.2,3,6 It should also be remembered that granulocytic sarcoma can both mimic and coexist with infection.9
Conclusion
A nasal septal abscess has a characteristic appearance on CT examination as a cystic collection of fluid with thin rim enhancement involving the nasal septum. It is important for the radiologist to be aware of this rare infectious complication of nasal trauma and sinus infection, especially in patients with immunosuppression, not only to provide the correct diagnosis, but also to ensure immediate treatment to avoid life-threatening complications.
References
- Received April 8, 2007.
- Accepted after revision April 16, 2007.
- Copyright © American Society of Neuroradiology