Abstract
BACKGROUND AND PURPOSE: Subsequent fracture is often seen after percutaneous vertebroplasty. The purpose of this prospective study was to evaluate preoperative multidetector row CT (MDCT) for the prediction of subsequent fractures after vertebroplasty.
MATERIALS AND METHODS: This study included 26 consecutive patients (18 women and 8 men) with osteoporotic compression fractures (58 vertebrae). A 64-section MDCT with multiplanar reformation was obtained 1 day before the procedure. Subsequent MR imaging was used to evaluate new fractures at least 3 months after treatment on a routine basis or if there was recurrent pain. We used logistic regression analysis with MDCT findings and clinical data for statistical evaluation according to the location of new fractures.
RESULTS: Subsequent fractures were noted at 14 adjacent vertebrae (12.1%) in 13 patients and at 14 remote vertebrae in 6 patients (23.1%). Subsequent fractures in adjacent vertebrae tended to occur in small vertebrae before treatment (P < .05). Steroid medication and low CT value in nonfractured vertebrae were associated with subsequent fractures in remote vertebrae (P < .05). Further collapse of the treated vertebral bodies was noted in 10 patients (11 vertebrae [19.0%]) without specific findings (P > .05).
CONCLUSIONS: The small size of the treated vertebrae may relate to subsequent fractures in adjacent vertebrae. Steroid use and low CT value of nonfractured vertebrae on preoperative MDCT can be associated with subsequent fractures in remote vertebrae.
Percutaneous vertebroplasty is a minimally invasive treatment that provides pain relief and stability for osteoporotic compression fractures.1–25 Previous studies have shown significant pain relief in more than 80% of patients.1–4 However, the substantial risk for subsequent fractures was also reported.3–25
In our clinical work, we used multidetector row CT (MDCT) for treatment planning for vertebroplasty. The well-known disadvantage of the use of CT is its radiation exposure. However, it can offer precise information on bony structures including their degree of collapse and extent of fracture. In addition, previous studies suggested severe collapse (wedge deformity)5,6 as one of the predictors for subsequent fractures after vertebroplasty. Therefore, the purpose of this prospective study was to evaluate preoperative MDCT for the prediction of subsequent fractures after percutaneous vertebroplasty.
Materials and Methods
Our institutional review board approved this study, and we obtained written informed consent from all participants before their enrollment in the study.
Patients
The participants in this prospective study were 26 consecutive patients (18 women and 8 men; age range, 54–88 years; median age, 74 years) in whom a total of 60 vertebral bodies were treated with percutaneous vertebroplasty at our institution. All of these patients had back pain refractory to conservative treatment with compression fractures on MR imaging. All patients except 1 (1 vertebra) returned 3 months after the procedure on a routine basis or sooner with recurrent pain. The patients were then routinely observed at our clinic 6, 12, 18, and 24 months after the treatment or on an as-needed basis. All of the patients underwent MR imaging at the time of all return visits. One patient who did not have a return visit died 22 days after the second treatment for subsequent fracture as a result of end-stage lung cancer. This fracture was considered osteoporotic because the bone specimen from the treated vertebra did not reveal a malignant growth. In addition, in 1 patient who was treated at T6 and T12 on the basis of MR imaging findings, a treated vertebra at T6 was not scanned preoperatively. Thus, this study included 58 vertebrae in 26 patients that were treated in 32 sessions. In these 26 patients, 7 patients were treated twice, but 1 patient who died of lung cancer described previously did not have a return visit after the second treatment. Therefore, this study included a total of 32 sessions in which 20 patients were treated once and 6 patients were treated twice. In these sessions, 1 vertebra was treated in 13 sessions, 2 were treated in 13 sessions, 3 in 5 sessions, and 4 in 1 session. Most of the treated vertebrae were located around the thoracolumbar junction. The locations and numbers of the treated vertebrae were as follows: T5 (n = 1), T7 (n = 2), T8 (n = 2), T9 (n = 3), T10 (n = 2), T11 (n = 3), T12 (n = 12), L1 (n = 16), L2 (n = 6), L3 (n = 5), and L4 (n = 6).
Preoperative evaluation included bone mineral attenuation (BMD) measured at the femur without a fracture (QDR 4500 A; Hologic, Bedford, Mass). Long-term use of steroid medication was also investigated.
The interval of the development of new fractures was calculated on the basis of the time between the date of treatment and the date of the diagnosis of a new compression fracture, which was based on positive MR findings.
Vertebroplasty Technique
Vertebroplasty was performed with a bipedicular or unipedicular approach with 11-gauge bone biopsy needles (Osteo-site; Cook, Bloomington, Ind) placed into the anterior one fourth of the vertebral body. The procedure was performed under biplane fluoroscopic control with the patient under conscious sedation and local anesthesia on an inpatient basis.
Once the needles were placed in the vertebral body, liquid and powder polymethylmethacrylate (Cranioplastic; Codman, Raynham, Mass) was mixed with 15 g of barium sulfate. Under biplane fluoroscopic guidance, the cement was injected through the needles. Injection was continued until the vertebral body was filled toward its posterior 25% or there was notable leakage. The amount of cement injected ranged from 1.5 mL to 15 mL (mean, 5.0 mL). The patient was lying prone on the angiographic table during the injection and remained in that position until the cement had completely hardened (approximately 15 minutes); then the patient was transferred to a regular bed. There were no immediate complications in any of the patients.
Imaging Technique
A 64-section MDCT (Aquilion; Toshiba, Tokyo, Japan) was performed within 1 day before vertebroplasty with the patient in the supine position. Typical imaging parameters were as follows: collimation, 64 × 0.5 mm; gantry rotation time, 400 ms; tube voltage, 120 kVp; tube current, 300 mA; FOV, 240 × 240 mm; and matrix, 512 × 512. Most of the patients underwent CT from T6 to L5.
All patients underwent entire thoracic and lumbar MR imaging with a 1.5T imager (Achieva; Philips Medical Systems, Best, the Netherlands) within 1 day before and 2 days after treatment as well as on all return visits. At minimum, fat-suppressed sagittal T2-weighted (TR, 1700 ms; TE, 120 ms; NEX, 4) and sagittal T1-weighted (TR, 424 ms; TE, 12 ms; NEX, 3) images were obtained. Additional typical imaging parameters were as follows: FOV, 32 × 32 cm; matrix size, 384 × 512; section thickness, 4 mm; and intersection gap, 0.4 mm.
Image Assessment
All images were transferred to PACS (Rapideye; Toshiba, Tokyo, Japan). MDCT was shown with regular clinical window settings. Multiplanar reformation of the axial, sagittal, and coronal planes perpendicular to each vertebra with 1-mm thickness without a gap was carried out with use of software (AquariusNet; TeraRecon, San Mateo, Calif). The analysis was based on a reading by a neuroradiologist. The preoperative height of the treated vertebrae and their adjacent disks was measured in 3 portions (anterior, middle, and posterior) in the midsagittal plane perpendicular to an inferior endplate and parallel to the anteroposterior direction of a spinous process. The wedge angles of the treated vertebral bodies and their adjacent disks were also measured in the same plane. In addition, CT values of the treated, adjacent, and nonfractured remote (at least 1 vertebra away from the treated vertebral body) vertebrae were measured in the midsagittal plane.
Subsequent fractures were defined as new bone marrow edema on follow-up MR including sagittal T1-weighted and fat-suppressed T2-weighted images compared with baseline examinations obtained 1 day before and within 2 days after treatment. Subsequent fractures were divided into 3 types according to their locations. Classification criteria were as follows: adjacent type, new bone marrow edema in vertebrae adjacent to treated vertebral bodies; remote type, new bone marrow edema in vertebrae with at least 1 vertebral body between the treated vertebrae; and further collapse, treated vertebrae with height loss.
Statistical Analysis
We performed statistical analysis with commercially available software (SPSS 17.0J for Windows; SPSS, Chicago, Ill). We used logistic regression analysis with univariate and multivariate models. Relevant clinical characteristics including the BMD (T-score), and a history of long-term use of steroids were entered to determine predictors of new fractures. In addition, mean height (mm) and wedge angle (°) of the treated vertebrae and adjacent disks, and mean CT value of the treated, adjacent, or remote vertebrae were also entered depending on the location of the type of subsequent fractures. A P value of less than .05 on both univariate and multivariate analysis was considered statistically significant.
Results
The mean follow-up period was 200 days (range, 26–730 days). Eight of 26 patients returned with subsequent fractures before the routine follow-up visit at 3 months (range, 1–56 days).
In this study, 9 of 26 patients had a history of steroid use. The causes of its use were rheumatoid arthritis in 4 patients, chemotherapy for primary cancer in 2, atopic dermatitis in 1, myasthenia gravis in 1, and multiple sclerosis in 1.
Subsequent fractures were noted at 14 adjacent vertebrae (14/116, 12.1%) in 13 patients (Fig 1). The mean interval between the treatment and the identification of these fractures was 68 days (range, 1–231 days). The locations and numbers of the treated vertebrae that caused new fractures in adjacent vertebrae were as follows: T7 (n = 1), T8 (n = 1), T12 (n = 1), L1 (n = 7), L3 (n = 2), and L4 (n = 2). Subsequent fractures in adjacent vertebrae tended to occur in smaller vertebrae before treatment compared with the vertebrae without adjacent fractures (P < .05) (Table 1).

A 72-year-old woman with a compression fracture at L3. A, Preoperative MDCT with sagittal reformation shows a compression fracture at L3 with an intravertebral cleft (arrow). B, Postoperative T1-weighted MR image obtained 2 days after treatment shows the treated L3 vertebral body without other fractures. C, Postoperative T1-weighted MR image obtained 19 days after treatment shows a subsequent fracture at L2.
Associations between variables and subsequent fractures in adjacent vertebrae
Subsequent fractures were noted in 14 remote vertebrae in 6 patients (23.1%) (Fig 2). The mean interval between the treatment and the identification of these fractures was 100 days (range, 4–231 days). The locations and numbers of the treated vertebrae that caused new fractures in remote vertebrae were as follows: T7 (n = 1), T8 (n = 1), T11 (n = 1), T12 (n = 3), L1 (n = 2), L2 (n = 2), L3 (n = 2), and L4 (n = 2). Steroid medication and low CT values in remote vertebrae were risk factors for subsequent fractures in remote vertebrae (P < .05) (Table 2).
{kind=link}
{kind=link}
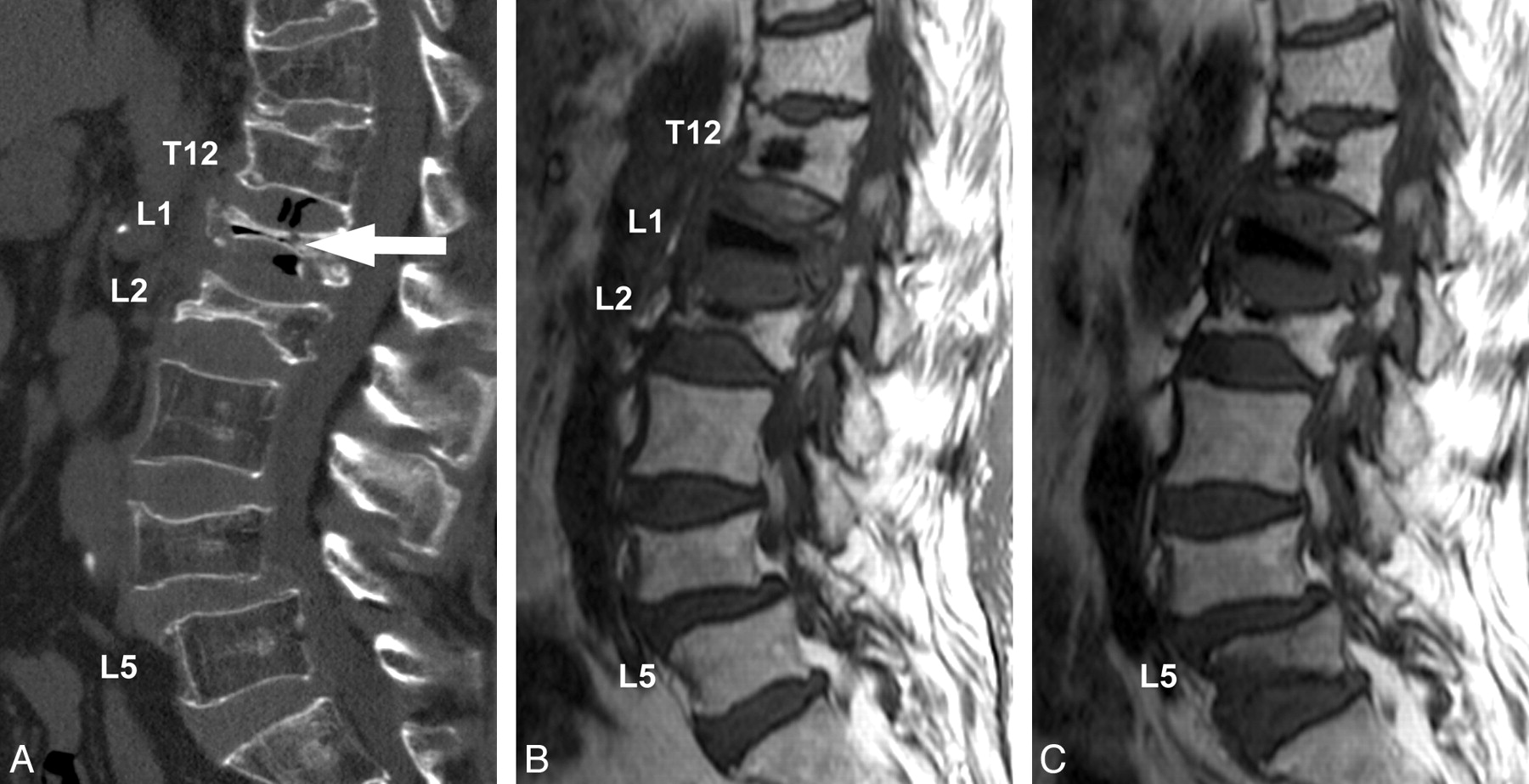
A 76-year-old woman with compression fractures at T11, T12, L1, L2, and L4. The patient had a long history of steroid use for rheumatoid arthritis. A, Preoperative MDCT with sagittal reformation shows compression fractures at T11, T12, L1, L2, and L4. An intravertebral cleft is noted at L1 (arrow). B, Postoperative T1-weighted MR image obtained 2 days after treatment shows the treated vertebral bodies at T12, L1, and L2. C, Postoperative T1-weighted MR image obtained 93 days after treatment shows a subsequent fracture at L5.
Associations between variables and subsequent fractures in remote vertebrae
Further collapse of the treated vertebral bodies was noted in 10 patients (11 vertebrae, 19.0%). The mean interval between the treatment and identification of these collapses was 76 days (range, 2–190 days). The locations and numbers of the treated vertebrae with further collapse were as follows: T5 (n = 1), T9 (n = 1), T12 (n = 5), L1 (n = 1), L2 (n = 1), and L4 (n = 2). No specific finding related to further collapse of treated vertebrae was seen (P > .05) (Table 3).
Associations between variables and subsequent fractures in treated vertebrae
The mean CT value of treated, adjacent, and remote vertebrae was 228.7, 154.6, and 147.5, respectively.
Discussion
This study revealed the usefulness of preoperative MDCT for the prediction of subsequent fractures in adjacent and remote vertebral bodies. To the best of our knowledge, no previous study has analyzed risk factors for subsequent fractures according to their locations or preoperative CT findings as predictive factors. It has been reported that adjacent vertebrae are the most common site of subsequent fractures after cement augmentation procedures including vertebroplasty and kyphoplasty, which uses balloons to create cavities before cement injection (incidence, 41%–76%).5–10,26,27 From preoperative clinical or radiologic datasets, previous studies have proposed risk factors related to adjacent fractures including low body mass index,9,11 location of thoracolumbar junction,12 the presence of cleft,6,13 and shorter distance from the treated vertebrae.12 In addition, Lee et al5 reported that advanced age of the patient, treatment of multiple vertebrae, and severe wedge deformity were risk factors for subsequent fractures. Other investigators proposed that severity of the vertebral fractures as well as disk narrowing was related to subsequent vertebral and nonvertebral fractures in patients with osteoporosis.28,29 We identified small size of vertebrae before treatment as a risk factor for subsequent fractures, seen in 12% of vertebrae adjacent to the treated vertebral bodies, probably reflecting the severity of collapsed vertebrae as an indicator for new fracture. On the basis of the postoperative images, the presence of intradiskal leak9,14,15 and greater height restoration12 were also considered to be potential risk factors. In this study, we used only preoperative MDCT for evaluation because our intention was to make a good patient selection preoperatively. We will analyze postoperative images in the future.
In this study, subsequent fractures were noted in 14 remote vertebrae in 6 patients (23.1%). We found steroid use and low CT values in remote vertebrae without a fracture to be risk factors for subsequent fractures in remote vertebrae. Long-term steroid use is considered to be one of the major causes of secondary osteoporosis.30–32 Previous studies showed a 2 to 3 times higher incidence of refracture in patients with steroid use compared with incidence of those with primary osteoporosis.16,17 In addition, Harrop et al26 reported a higher incidence of subsequent fractures in patients with steroid use after balloon kyphoplasty. However, other proponents revealed no relationship between subsequent fractures and steroid use.18 This issue should be resolved in the future. From our results, a low CT value in nonfractured vertebrae can stand for the fragility of the vertebral body. However, the CT value of a vertebra can be affected by the degree of fatty marrow, red marrow, bone trabeculae, and cortical bone. More sophisticated evaluation of vertebral microstructure or quantification of trabecular and cortical bone has been proposed33,34; however, it was not available to us at the time of this study. Moreover, in nonadjacent fracture, Ahn et al9 reported relatively low segmental mobility as a predictive factor, though this was also not available in the present study. Further investigation is also required.
Further collapse of the treated vertebral bodies was noted in 10 patients (11 vertebrae, 19.0%) in this study. We could not identify any specific findings related to recollapse of the treated vertebrae. Previous studies have reported well-maintained vertebral height after vertebroplasty.8,19 However, other investigators reported the occurrence of recollapse of the treated vertebrae or cement extrusion, mostly because of the presence of intravertebral cleft (osteonecrosis) or greater height restoration.20–22 In contrast to the achievement of the height restoration, Gilula23 recommended maximal filling to prevent further collapse of the treated vertebral body. In our clinical setting, we also tried to obtain maximal filling without causing other complications such as pulmonary embolism or worsening of spinal stenosis.
The short follow-up period was a limitation of our study. To investigate late complications of the procedure, a randomized study with a long observation time is needed. However, in vertebroplasty, previous studies have indicated that subsequent fractures occurred soon after the procedure, mainly within 3 months.7,8,10,24,25 Therefore, we believe that most of the early complications have been observed in this study. Another limitation of this study was the small number of patients included. This project is ongoing and may produce results with a larger population in the future. We analyzed the incidence of subsequent fractures on a vertebra basis. The information on patient background may be exaggerated in this study. Because of difficulty defining symptomatic or asymptomatic fracture in elderly patients with chronic back pain, we could not evaluate patients' activities precisely. Therefore, we defined new bone marrow edema as new fracture that was unable to separate from increased degenerative disease related to renewed activity. These might be other limitations in this study. In addition, as we previously mentioned, we lacked detailed analysis of CT value of vertebrae. Quantification of BMD on CT should be favorable; however, a clinical study showed usefulness of CT attenuation measurement as an indicator for bone mineral content.35 We need further investigation in this issue.
Conclusions
The small size of the treated vertebrae is associated with subsequent fractures in adjacent vertebrae. Steroid use and low CT value of nonfractured vertebrae on preoperative MDCT were found to be risk factors for subsequent fractures in remote vertebrae. MDCT before percutaneous vertebroplasty could predict subsequent fractures in adjacent and remote vertebrae.
Acknowledgment
We thank Mr. Junji Kishimoto for advice in statistical analysis.
Footnotes
Previously presented at: Annual Meeting of the American Society of Neuroradiology and Neuroradiology Education and Research Foundation Symposium, May 16–21, 2009, Vancouver, British Columbia, Canada.
This study was supported in part by research grants from the Ministry of Education, Culture, Sports, Science and Technology (19790879) and the Japan Radiological Society (KJ-18–3).
Indicates open access to non-subscribers at www.ajnr.org
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- Received January 20, 2009.
- Accepted after revision May 7, 2009.
- Copyright © American Society of Neuroradiology