Abstract
BACKGROUND AND PURPOSE: Detection and evaluation of ruptured aneurysms is critical for choosing an appropriate endovascular or neurosurgical intervention. Our aim was to assess whether bone-subtraction CTA is capable of guiding treatment for cerebral aneurysms in patients with acute SAH and could replace DSA.
MATERIALS AND METHODS: We prospectively studied 116 consecutive patients with SAH with 16–detector row bone-subtraction CTA and DSA before intracranial aneurysm treatment. Two independent neuroradiologists reviewed the bone-subtraction CTA blinded to DSA (reference standard). We determined the accuracy of bone-subtraction CTA for aneurysm detection and the measurement of aneurysm dimensions and compared the radiation doses of the 2 imaging modalities.
RESULTS: Seventy-one patients (61%) had 74 aneurysms on DSA. Bone-subtraction CTA detected 73 of these aneurysms, but it detected 1 additional aneurysm. On a per-aneurysm basis, sensitivity, specificity, and positive and negative predictive values for bone-subtraction CTA were 99%, 98%, and 99% and 98%, respectively. For aneurysms of ≤3 mm, sensitivity was 94% (95% CI, 73%–99%). Bone-subtraction CTA slightly overestimated neck and dome diameters by <0.2 mm and overestimated the dome-to-neck ratios by 2% on average. Dose-length product was 565 ± 201 mGy × cm for bone-subtraction CTA and 1609 ± 1300 mGy × cm for DSA.
CONCLUSIONS: Bone-subtraction CTA is as accurate as DSA in detecting cerebral aneurysms after SAH, provides similar information about aneurysm configuration and measures, and reduces the average effective radiation dose for vascular diagnostics by 65%. Diagnostic equivalence in association with dose reduction suggests replacing DSA with bone-subtraction CTA in the diagnostic work-up of spontaneous SAH.
ABBREVIATIONS:
- BSCTA
- bone-subtraction CTA
- D/N
- dome-to-neck
- NECT
- nonenhanced CT
Prompt detection and evaluation of ruptured intracranial aneurysms is critical for choosing an appropriate endovascular or neurosurgical intervention.1 Invasive digital subtraction angiography carries an overall risk of neurologic complications, resulting in permanent deficits in 0.5%.2,3 Providing false-negative results in 5%–10% of patients,4 it also may increase the risk of rebleeding.5,6
Multidetector CT angiography with high spatial resolution and bone-subtraction CTA (BSCTA) approaches the diagnostic accuracy of DSA in the detection of intracranial aneurysms.7⇓⇓⇓⇓–12 Thus, BSCTA can be considered an alternative to DSA in treatment planning.13,14 Some authors already recommend BSCTA as the primary imaging in acute SAH.7,15,16 However, it still seems unclear whether BSCTA can provide sufficient information for therapy decisions, making diagnostic DSA redundant.17,18
We therefore tested the hypothesis that BSCTA is as accurate as DSA for the identification and characterization of cerebral aneurysms in patients with SAH, even for small aneurysms and for those at the level of the skull base. We additionally studied the reliability of BSCTA and radiation-exposure reduction by avoiding diagnostic DSA.
Materials and Methods
Participants
After University Hospital Dresden review board approval (EK No. 73042008) and informed consent, from November 2007 to June 2011, neuroradiologists or neurosurgeons familiar with the protocol prospectively enrolled patients with acute SAH able to undergo CTA and DSA. We classified SAH severity with the Fisher score. Patients underwent nonenhanced CT (NECT) and BSCTA followed by DSA with 3D reconstructions. We documented the time interval between CT and DSA. Patients with typical exclusion criteria for CTA or previous coiling or clipping were excluded. Because we aimed to assess the accuracy of BSCTA for the detection and description of cerebral aneurysms, we did not follow patients with perimesencephalic SAH further.
CTA Imaging Technique
Examinations were performed with the patient in the supine position from the C1 vertebral body to the vertex on a 16–detector row spiral CT (Somatom Sensation 16; Siemens, Malvern, Pennsylvania). We performed BSCTA after low-dose NECT (bone mask) and CTA, avoiding motion by head fixation and minimizing the delay between the 2 scans.
We did not use standard NECT for bone masking because standard NECT is acquired with a gantry tilt preventing direct x-ray to the eye lenses, whereas CTA data are acquired with no gantry tilt. The BSCTA algorithm used requires similar, narrow, section acquisition (0.75 mm for high spatial resolution) and datasets with minimum motion artifacts (0.5 seconds for minimized motion artifacts during acquisition). Standard-dose NECT, however, requires a slower rotation time of 1.0 second (to collect a sufficient amount of x-ray quanta) and a wider collimation of 1.5 mm. The CT scan parameters are listed in Table 1. The acquisition time was approximately 10 seconds. Bone-subtraction was performed automatically by using special prototype software on a workstation (syngo 2006G and syngo MultiTechnique Workplace, VE31D; Siemens).
Scan parameters for CT examinations
DSA and 3D-DSA
We used a rotational biplane DSA unit (Allura Xper FD 20 biplane; Philips Healthcare, Best, the Netherlands) for panangiography (all cerebral arteries). Per acquisition, we administered 3–6 mL of nonionic contrast agent (iohexol, Accupaque, 300 mg I/mL; GE Healthcare, Milwaukee, Wisconsin). 3D reformatted images of rotational angiographic data were generated at the DSA workstation.
Image Analysis
Two neuroradiologists (D.M., K.E.), with 14 and 10 years of experience, reviewed the DSA images independently and blinded to BSCTA. Readers were informed of the patient's clinical symptoms and initial CT findings. Reading of BSCTA and DSA datasets was separated by 8–10 weeks to prevent bias. To assess intraobserver reliability, reader 1 analyzed 15 randomly selected BSCTA imaging studies (12.9%) twice, separated by an interval of 1 month.
An aneurysm was considered entirely characterized if all 3 orthogonal dimensions were obtained and the aneurysm neck and dome and arterial incorporations into the sac or neck were visualized and precisely measured. We categorized aneurysms as “berry-formed,” “fusiform,” and “branching” if they were located at an arterial bifurcation.
The readers generated maximum intensity projections, volume rendering technique reformations, and multiplanar reconstructions searching for aneurysms. If multiple aneurysms were detected, the most likely source of bleeding was estimated. Dome-to-neck (D/N) ratios were calculated for both modalities. The 2 readers evaluated images in consensus in case of discrepancies. We evaluated the effect of patient motion on image quality for DSA and BSCTA and rated the quality of BSCTA images on a 4-point scale as “excellent,” “good,” “moderate,” or “poor.”
Radiation Dose
We measured the dose-length product of both modalities and calculated the effective doses. Among the recorded values for DSA examinations, we only considered the diagnostic portion of the dose-length product for comparison. Exposure information was reported automatically, as required by the standard of the International Electrotechnical Commission (IEC 60601-2-43) for total fluoroscopy time in minutes, total number of exposures in numbers, accumulated fluoroscopy dose in milligrays, accumulated exposure dose in milligrays, total dose in milligrays, total number of frames in numbers, image-area dose product in milligrays, entrance dose and air kerma in milligrays, exposure start time, kilovolt (peak), distance source-to-image receptor distance, exposure time, x-ray tube current, positioner primary angle, positioner secondary angle, and frame rate.
Examination and dose reporting for both BSCTA and DSA examinations are provided through Radiology Information DICOM 2-way interface, by using the DICOM Worklist Management and Technique Performed Procedure Step Standards.
Statistical Methods
We used MedCalc for Windows 12 (Version 12.3.0; MedCalc Software, Mariakerke, Belgium) for statistical analysis. We considered DSA, including 3D reconstructions, as the reference standard for aneurysm evaluation. We calculated the sensitivity, specificity, and accuracy of BSCTA on per-aneurysm and per-patient bases and used the Wilson procedure, without a correction for continuity, for the limits of the CI. We used the Cohen κ to quantify inter- and intrareader agreement beyond chance in detecting aneurysms with BSCTA. A P value ≤ .05 was statistically significant. We compared the DSA and BSCTA differences for aneurysm dome and neck diameter and the D/N ratio, applying the Bland-Altman method and a paired Student t test, to analyze differences in radiation doses.
Results
Participants
During 44 months, 269 consecutive patients presented to our department with SAH. We excluded 6 patients with prior clipping or coiling and 147 patients due to imaging protocol violations. Finally, 116 patients (50% women) (mean age, 53.9 ± 13.6 years) were prospectively examined with BSCTA and DSA according to the study protocol.
CT Findings
All patients had SAH, with a Fisher grade 1 in 8 patients (6.9%), 2 in 7 patients (6.0%), 3 in 42 patients (36.2%), and 4 in 59 patients (50.9%).
DSA Reference
The time between BSCTA and DSA varied from 20 minutes to 43 hours (median time, 7.0 hours). Of 116 patients, 71 patients (61.2%) had 74 intracranial aneurysms on initial DSA. Table 2 shows the locations and sizes of intracranial aneurysms as detected and characterized by DSA. We found 53 branching aneurysms (71.6%), 20 berry-form aneurysms (27.0%), and 1 fusiform aneurysm (1.4%). Among the 45 patients without aneurysms, 6 had arteriovenous malformations. We could not identify the cause of SAH in 39 patients, among them 27 patients with additional intracerebral hematomas. We did not have any observations because our patients with acute SAH had not shown signs of vasospasm. The average amount of contrast media used for diagnostic DSA was 106.4 ± 39.8 mL, with a median of 100 mL. The maximum amount was 230 mL, and the lowest, 50 mL.
Location and sizes of cerebral aneurysms as detected by DSA
BSCTA Findings
BSCTA detected 73 aneurysms in 70 patients, confirmed by DSA (Fig 1), and missed 1 anterior cerebral artery A2/A3 segment aneurysm with a diameter of 1.7 mm that was detected by DSA (Fig 2). Bone-subtraction CTA detected a 2.5-mm left MCA M2 segment aneurysm that was missed by DSA and finally confirmed by both readers in consensus (Fig 3). Both findings did not change clinical decisions.

A 78-year-old-female patient with symmetric infraclinoid aneurysms of the ICA. A, Volume-rendering of BSCTA displays both aneurysms (arrowhead: right aneurysm; arrow: left aneurysm). B and C, DSA confirms both aneurysms in size and configuration.
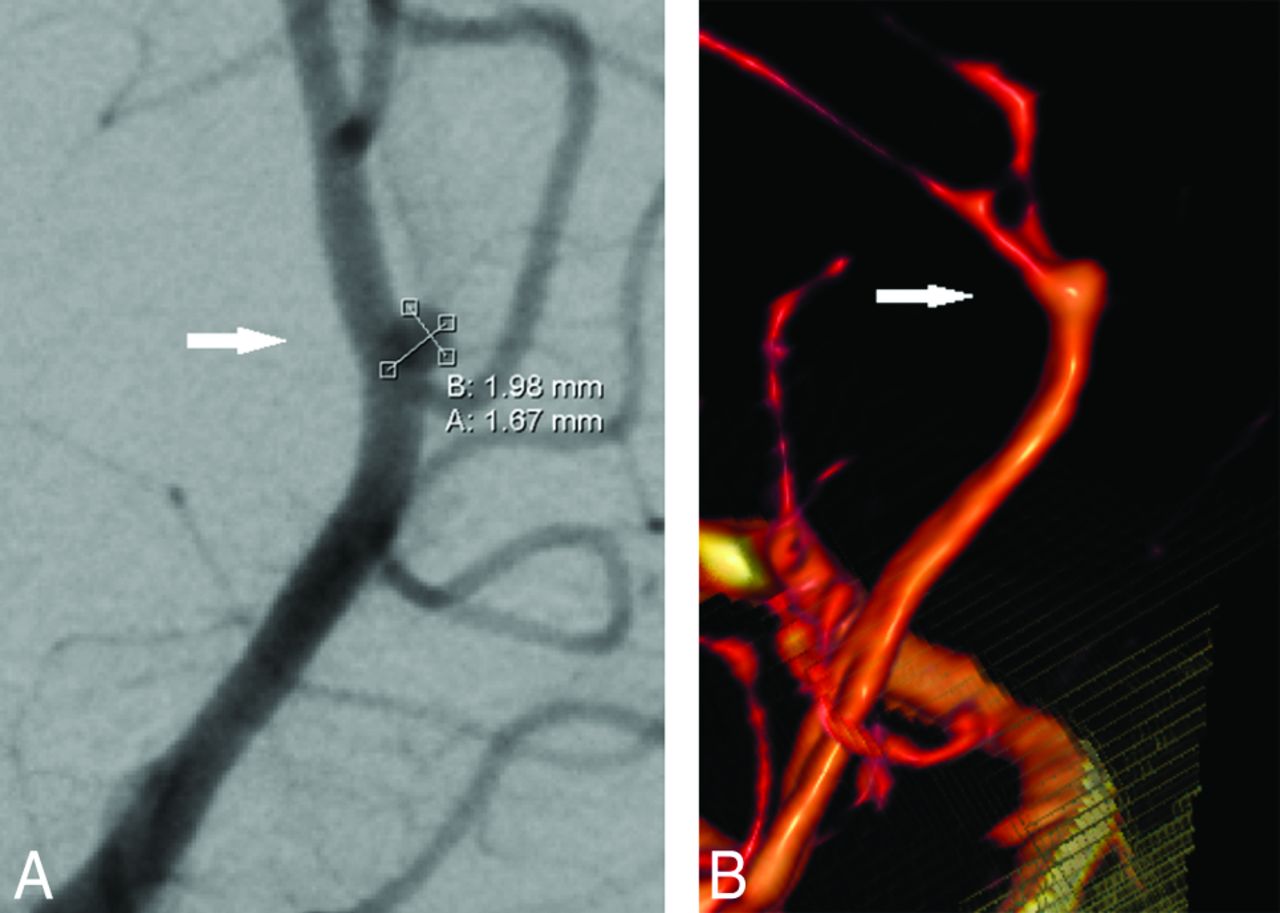
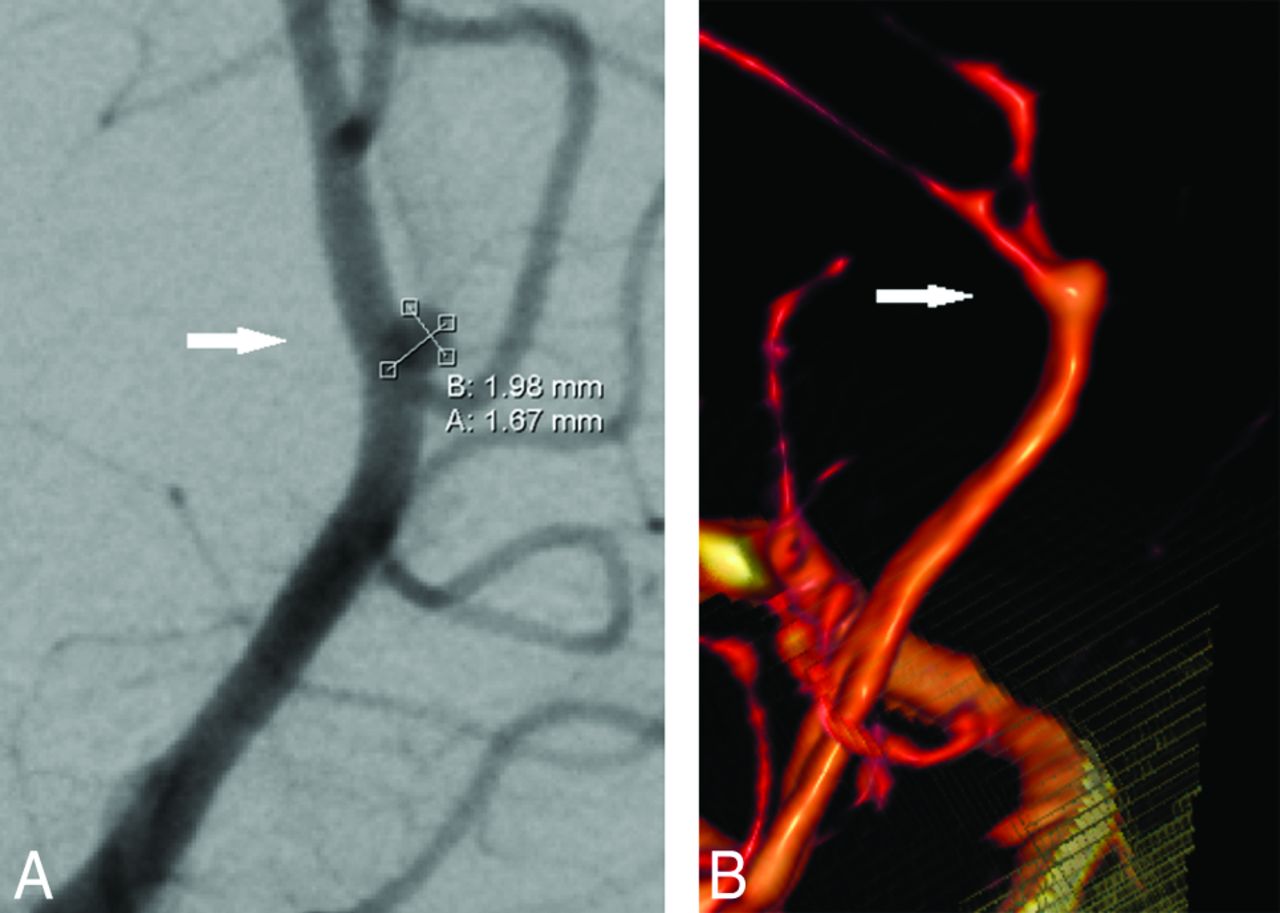
False-negative bone-subtraction CTA findings of an aneurysm of the right anterior cerebral artery in a 50-year-old woman. A, The right anterior oblique projection DSA shows a small broad-based aneurysm (arrow). B, On volume-rendering reconstruction, the aneurysm (arrow) appears fusiform. The white surface in the lower part of the image represents the bone-to-vessel boundary of the bone-removal processing.
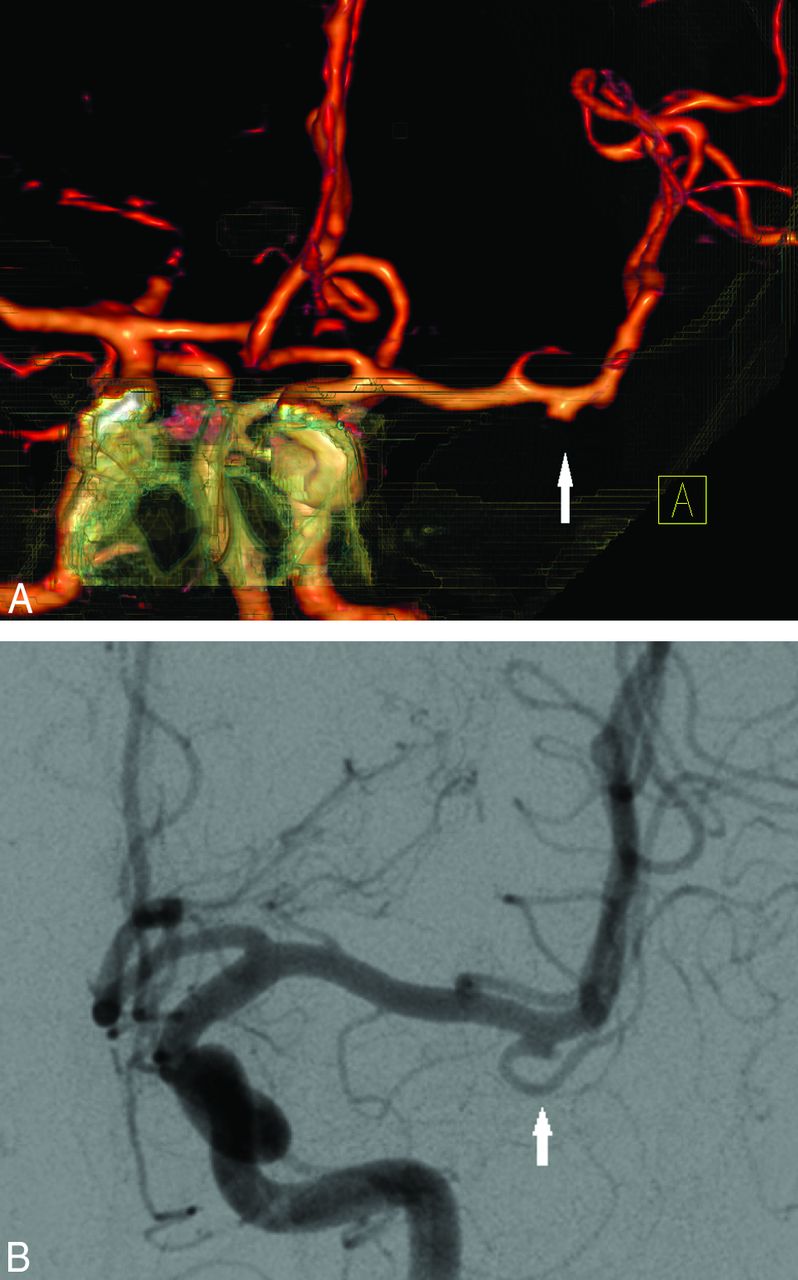
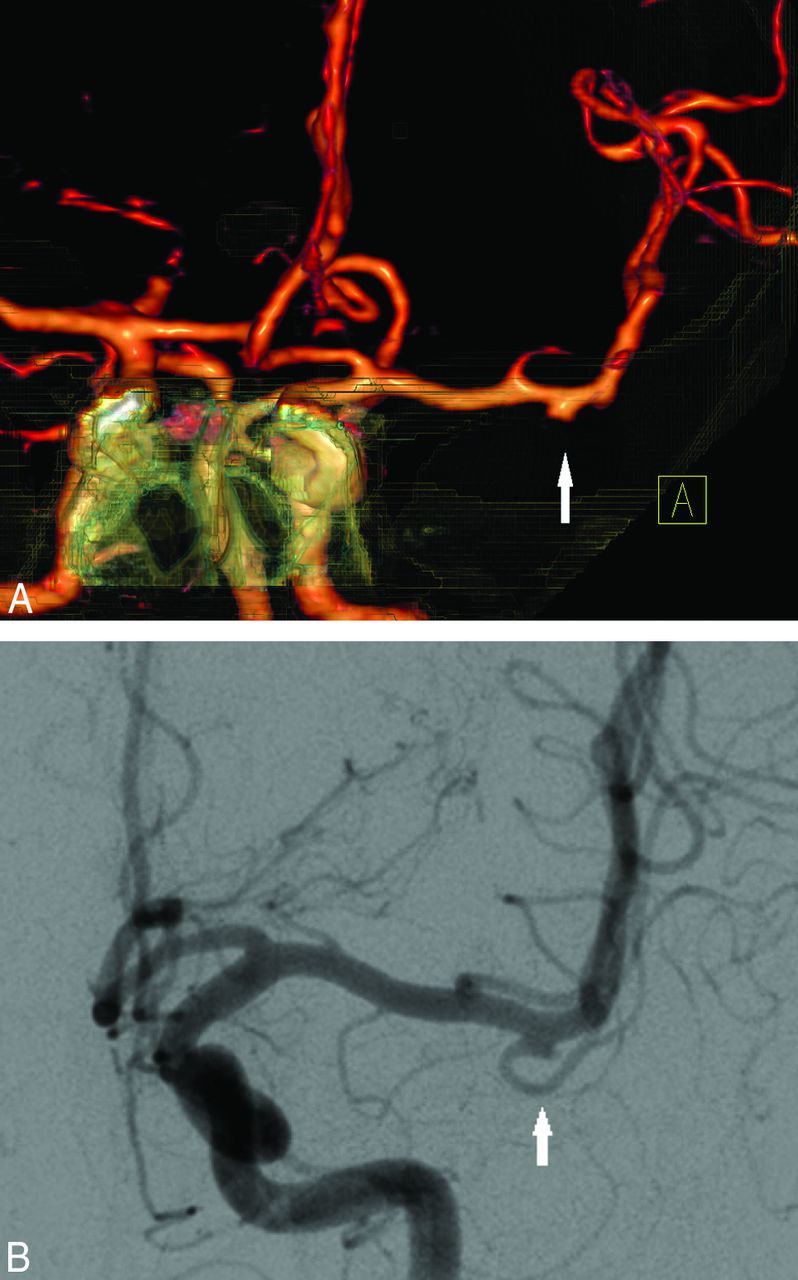
False-positive bone-subtraction CTA findings in an aneurysm (2.5 mm) of the left middle cerebral artery distal to the trifurcation in a 50-year-old man with 2 aneurysms. A, Volume-rendering of bone-subtraction CTA depicts the aneurysm (anteroposterior view) that was missed by DSA. B, 3D-DSA image of the initially missed M2 MCA trifurcation aneurysm (left anterior oblique view) that was confirmed in retrospect.
Sensitivity and specificity of BSCTA for intracranial aneurysms are presented in Tables 3 and 4.
Accuracy of BSCTA in detecting cerebral aneurysms
Accuracy of BSCTA in detecting cerebral aneurysms of different sizes
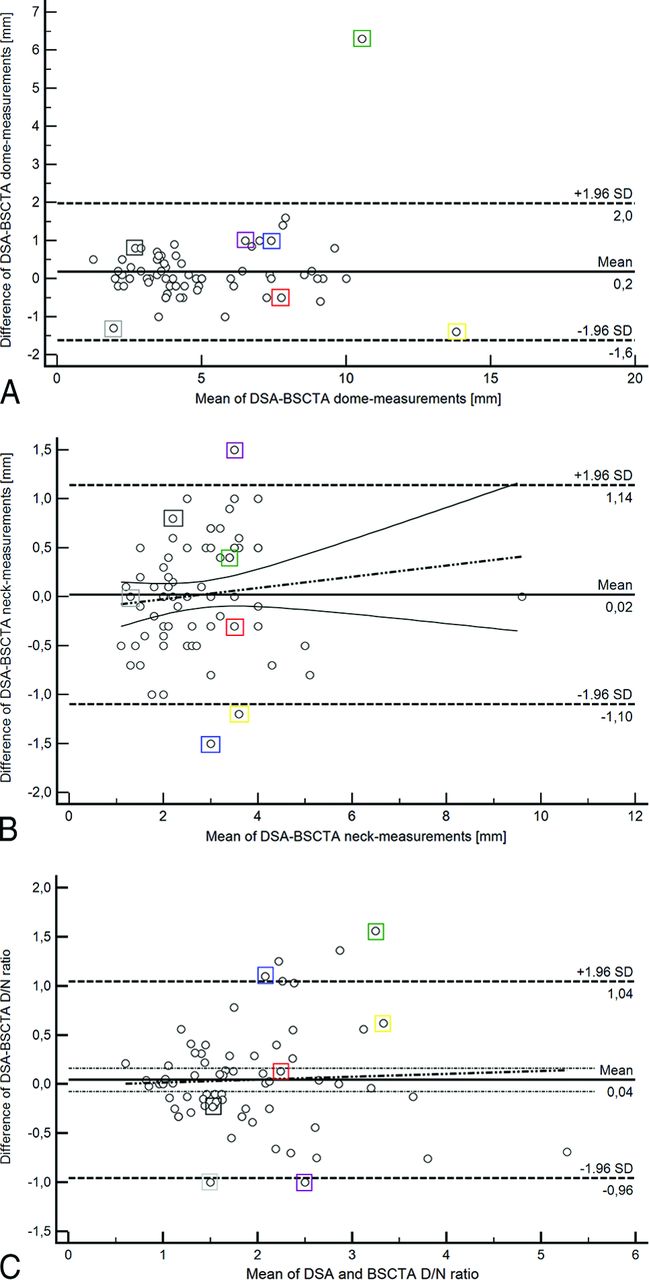
Aneurysm dome diameters were slightly longer with a 0.17-mm bias (95% CI, −0.04 to 0.39 mm) measured on BSCTA compared with DSA (Fig 4A). The measurement differences are relatively constant over all aneurysm diameters. Aneurysm neck diameters of BSCTA did not differ from those on DSA (Fig 4B). Figure 4C shows that BSCTA aneurysm D/N ratios differ by −0.04 only (95% CI, − 0.16 to 0.08) from the DSA D/N ratios. The average DSA D/N ratio was 1.90 ± 0.86, and the average BSCTA D/N ratio was 1.86 ± 0.84. On average, BSCTA D/N ratios were 2% smaller than DSA D/N ratios (P = .4678). The highest agreement of methods was for the D/N ratio of 1.5–2.0. Comparison of the distribution of D/N ratios in DSA versus BSCTA is shown in Fig 4C.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bland-Altman plots show the relationship between differences and means of DSA and BSCTA in aneurysm dome (A) and neck (B) measurements and dome/neck ratios (C). The black dotted line indicates the regression line of the differences. The 2 thin black lines represent the 95% confidence interval for the regression line of the differences. A, Bone subtraction CTA tends to overestimate aneurysm domes by 0.17 mm (95% CI, 0.04–0.39 mm) and has a mild trend toward higher values for dome diameters with larger values. The colored rectangular boxes highlight manual measurements with interpolation of DSA results because DSA millimeter calibrations were not transferred with the other DSA data. The outlier case is 1 large 14.0-mm aneurysm that was overestimated by 6.0 mm and belongs to the manually calculated measurements. B, Bone-subtraction CTA measurements of the aneurysm neck are in good agreement with DSA (0 ± 1.96 mm). Outlier cases are small 2.5- and 2.7-mm aneurysms that were underestimated by −1.5 and −1.2 mm. The third outlier was a 2.7-mm aneurysm that was overestimated by 1.5 mm. C, Bone-subtraction CTA slightly overestimates dome/neck ratios compared with DSA (mean, 0.04; 95% CI, 0.08–0.16). Four of the 6 outliers belong to the manually calculated DSA measurements (colored rectangular boxes).
Image Quality and Reliability
Overall bone-subtraction quality was high (91.4% good or excellent). Ten of 116 datasets were rated moderate or poor. Fifteen of 74 aneurysms were near or surrounded by bone and were correctly detected and characterized with BSCTA. Motion artifacts impaired DSA in 28 patients (23.9%) and BSCTA in 2 patients (1.7%). The effect of the motion-impaired data on the diagnosis is shown in Table 5. The interobserver agreement for the identification of aneurysms was substantial (κ = 0.950; 95% CI, 0.894–1.000). Agreement per patient was also high with (κ = 0.965; 95% CI, 0.916–1.000). Both readers agreed substantially on aneurysm configuration (κ = 0.969; 95% CI, 0.941–0.996; P < .001). Reader 1 agreed in all repeated cases with his initial reading.
Patient motion artifacts and performance on aneurysm detection
Radiation Dose
The mean dose-length product was 564.7 ± 201.4 mGy × cm for BSCTA and 1608.9 ± 1299.6 mGy × cm for DSA, meaning a reduction of 65% (P < .001, 2-sample Student t test). The effective dose for BSCTA was between 0.8 and 3.6 mSv, with an average effective dose of 1.3 ± 0.3 mSv. The average effective radiation dose for diagnostic DSA was 3.7 ± 2.98 mSv, ranging from 0.37 to 17.3 mSv.
Discussion
Our study confirmed a high accuracy of 16–detector row BSCTA in depicting and characterizing intracranial aneurysms. Immediate selection and planning of treatment was possible, even for complex and small aneurysms. This effect was true even for the relatively small amount of aneurysms that were close to bony structures. Furthermore, we demonstrated that the BSCTA method is already delivering high accuracy and robustness, even with widely available, outdated, 16–detector row multidetector CT hardware.
Therefore given the radiation-exposure reduction, BSCTA could replace diagnostic DSA. More advanced CT technology will probably perform as well or even better.
CTA has a high sensitivity and specificity in detecting intracranial aneurysms,8,9,11,12,17,19,20 but skull base structures can hide adjacent aneurysms.17,21 Bone-subtraction CTA22,23 has been developed to overcome this problem. A feasibility study22 and a study with 100 patients24 showed that BSCTA can improve the detection of vascular pathology closely adjacent to bony structures. These studies, however, did not use DSA as the reference standard to determine the diagnostic accuracy of BSCTA under clinical conditions. A recent 320–detector row BSCTA study evaluated the diagnostic accuracy of nonsubtracted and subtracted volumetric CTA data.12 The sensitivity for nonsubtracted CTA was 96.7% compared with 99.2% for subtracted CTA with 100% specificity for both.
Our findings are concordant with those in previous reports8⇓⇓–11 and compare well with a meta-analysis of twelve 16–detector row BSCTA studies.10 The sensitivity and specificity of BSCTA for small aneurysms (<3.0 mm) were lower than those in our population.
Our study results also compare well with 8 pooled 64–detector row BSCTA studies.10 Similar results were seen in a 64–detector row multidetector CT study with 89 patients.7 Our study results are also in line with those in 2 other studies by using modern dual-source and 320–detector row BSCTA.12
In our study, 1 aneurysm of <3 mm (2.5 mm) in diameter was missed by DSA (Fig 3). Another <3-mm (1.7 mm) aneurysm was initially missed by BSCTA (Fig 2). In both cases, these findings did not change the treatment strategy. Both methods have a small risk of missing small aneurysms. The diagnostic accuracy of DSA was limited by complex vascular anatomy (vessel trifurcation, small diameter of <3 mm) and inadequate projections due to patient motion. In a study with 50 patients presenting with diffuse aneurysmal pattern, 2 aneurysms were missed initially by DSA and BSCTA.25
False-positive cases on both 16– and 64–detector row BSCTA can be explained a by focal venous plexus overlying the MCA.17 Venous contrast has been described as a potential source of error.26,27 Venous enhancement is, however, not a crucial factor in the detection of cerebral aneurysms, except for extensive enhancement of the cavernous sinus.28 In contrast, with 16–detector row CTA and bolus triggering, arterial and venous structures can be distinguished by their different attenuations. Whether modern, wide-detector (>64–detector row), multidetector CT is capable of further improving the diagnostic accuracy of BSCTA, beyond the known 16– and 64–detector row multidetector CT results, needs to be investigated. With wider z-coverage, the negative effect of scatter radiation and conebeam artifacts increases and may not lead to a further gain in accuracy.29,30
The most common and well-studied geometric determinant of treatment decisions and outcome is the dome-to-neck ratio.21 Aspects of aneurysm geometry such as shape, size, dome-to-neck ratio, and location and the relationship to the parent vessels all may impact treatment decisions.31,32
Interobserver agreement in our study was somewhat higher than that reported previously.11,17,19,26 Intraobserver agreement was excellent as in another study by Lu et al.11
We had excellent interreader agreement for aneurysm identification and configuration. Our results are in line with those in other studies,17,26 even with a recent study with 320–detector row BSCTA33 comparing CTA with intraoperative observations.
Only 1 study evaluated the D/N ratios in a comparable fashion, but not in the same level of detail.26 In contrast to our results, this study reported a general overestimation of D/N ratio with 16–detector row BSCTA due to partial volume sampling effects.24 Considerable overestimation of the D/N ratio of aneurysms may have led to therapeutic option changes.26 Endovascular treatment of wide-neck or “difficult” aneurysms requires special techniques such as balloon- or stent-assisted coiling.21 Because we did not document the decisions of our interventionists and neurosurgeons, we do not know to what extent the information provided by BSCTA has influenced patient management. We can state, however, that BSCTA assessed the site and shape of cerebral aneurysms as accurately as DSA.
Radiation is an important factor for patients with SAH,34 because many are younger and need repeat brain imaging. Our BSCTA dose values were below the European reference value (2.4 mSv) for CT angiography of the brain.35 Our average DSA radiation dose remained at the lower limit of doses reported for DSA (3.5–6.5 mSv).36 A disadvantage of BSCTA is the radiation dose, due to 2 consecutive scans, which means an increase of exposure by 20%–25% above the level of standard CTA according to our and others' experience.37,38 Low-dose settings for nonenhanced CT are acceptable in achieving an effective dose below 3 mSv. Recently new approaches are being evaluated to replace the low-dose NECT with either a standard-dose NECT or a late venous CT dataset, to receive the subtraction bone mask.39⇓–41 Optimally, the work-up of SAH before the selection of a method of aneurysm treatment should be exclusively noninvasive diagnostics. In contrast to diagnostic DSA, BSCTA can reduce the door-to-treatment time by providing the relevant information instantly.17,26 It may even prevent DSA in cases with a clear indication for clipping.26,27,42 The accuracy of BSCTA being comparable with DSA now allows clipping of these aneurysms without additional DSA when transarterial intervention is not possible. In cases where the first CTA does not show the cause of SAH, it is not necessary to perform DSA. A second CTA is sufficient.
Moreover, BSCTA can exclude an aneurysm as the cause of spontaneous SAH.17
Our study has limitations. Although BSCTA was feasible in almost all patients, we could recruit patients only when the involved neuroradiologist was on duty and had ordered the new BSCTA protocol. We cannot safely exclude the possibility that the patients identified by study neuroradiologists were different from those with SAH seen by a radiologist not familiar with the study. We aimed to consecutively identify all patients with acute SAH and without previous aneurysm treatment, which means we had no knowledge of the source of bleeding. We thought this population was the best to study the accuracy of BSCTA. We lost patients for the study when radiologists on call were not yet familiar with the study protocol. We think, however, that the patients we recruited represented the population typical for acute SAH. Consequently, we extended the observation period to reach the planned sample size.
In our institution, we now recommend BSCTA in addition to NECT as the first imaging technique in patients with acute SAH. Our neurosurgeons clip aneurysms solely on the basis of this information in urgent cases that cannot be coiled. We have reduced the DSA protocol before intervention to the artery affected and do not further perform panangiographies. We further recommend repeat BSCTA in cases of CTA with negative findings in patients with SAH, but we admit that not all of our neurosurgeons consistently follow this advice.
Conclusions
The widely available 16–detector row BSCTA allows reliable and accurate detection and characterization of cerebral aneurysms in patients with acute SAH and thus can guide treatment decisions faster and more efficiently. If the location and shape of aneurysms favor surgical clipping, an additional DSA is no longer necessary because all information needed by neurosurgeons is provided. If coiling is preferred, complete diagnostic 4-vessel panangiography is no longer routinely required. Interventionists can focus DSA on the site of the symptomatic aneurysm. This new strategy will not only reduce the risks and radiation dose for patients and physicians, but also reduce cost and time. More modern CT technology may make BSCTA more efficient, more standardized, and finally easier to apply.
Footnotes
Disclosures: Peter Aulbach—RELATED: Support for Travel to Meetings for the Study or Other Purposes: Siemens, Comments: Siemens, as my employer, supports my studies through payments for traveling to the university and back. It is just the cost for hotel, car, and fuel; UNRELATED: Employment: Siemens, Comments: I am an employee of Siemens. My PhD is tolerated there as part of my personal development. My employer just compensates the cost for me to travel to the University (car, fuel, and hotel). Additionally, Siemens allows me to spend time at the university if it is not too many days. As long as my work output does not suffer, they tolerate it. Rüdiger von Kummer—UNRELATED: Board Membership: Lundbeck; Consultancy: Lundbeck, Penumbra, Covidien, Boehringer Ingelheim; Payment for Lectures (including service on Speakers Bureaus): Penumbra; Royalties: Elsevier, Springer, Comments: book chapter authorship.
Indicates open access to non-subscribers at www.ajnr.org
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- Received January 29, 2015.
- Accepted after revision June 22, 2015.
- © 2016 by American Journal of Neuroradiology