
Abstract
BACKGROUND AND PURPOSE: Infantile hemangiomas are common lesions in the pediatric population; in rare cases, an infantile hemangioma can be detected along the neural axis. The purposes of our study included determination of the incidence, location, and imaging appearance of neuroaxial infantile hemangiomas and their syndromic association. We also assessed additional features of cerebral and cardiovascular anomalies that may be associated with neuroaxial lesions.
MATERIALS AND METHODS: A retrospective cohort study was performed, searching the radiology database for patients with segmental infantile hemangiomas referred for assessment of possible hemangioma syndromes. We retrospectively reviewed brain and spine MR imaging studies, with particular attention paid to neuroaxial vascular lesions, as well as the relevant clinical data. Neuroaxial hemangioma imaging findings were described, and comparison of segmental cutaneous infantile hemangioma location with the imaging findings was performed in patients with confirmed hemangioma syndromes and in patients with isolated skin infantile hemangioma.
RESULTS: Ninety-five patients with segmental infantile hemangioma were included in the study, 42 of whom had a hemangioma syndrome; of those, 41 had posterior fossa brain malformations, hemangioma, arterial lesions, cardiac abnormalities, and eye abnormalities (PHACE) syndrome and 1 had diffuse neonatal hemangiomatosis. Neuroaxial involvement was detected in 20/42 patients (48%) with hemangioma syndromes and in no subjects with isolated segmental infantile hemangioma (P < .001). The most common intracranial hemangioma location was within the ipsilateral internal auditory canal (83%).
CONCLUSIONS: Many pediatric patients with segmental infantile hemangioma in the setting of hemangioma syndromes, especially those with PHACE, had neuroaxial hemangiomas. This finding may potentially lead to requiring additional clinical evaluation and management of these patients.
ABBREVIATIONS:
- IAC
- internal auditory canal
- IH
- infantile hemangioma
- MC
- Meckel cave
- PHACE
- posterior fossa brain malformations, hemangioma, arterial lesions, cardiac abnormalities, and eye abnormalities
Infantile hemangiomas (IHs) are benign vascular tumors common in infants.1⇓-3 IHs express endothelial glucose transporter 1, differentiating them from other pediatric vascular tumors.4 Unlike congenital hemangiomas, IHs are not discernable prenatally because they are known to proliferate and evolve after birth.5 The clinical evolution of all IHs progresses through several predictable phases: faint pink/red patches during the nascent phase (shortly after birth), rapid proliferation (for the first 3–6 months), a plateau phase until approximately 12 months, followed by slow involution.6
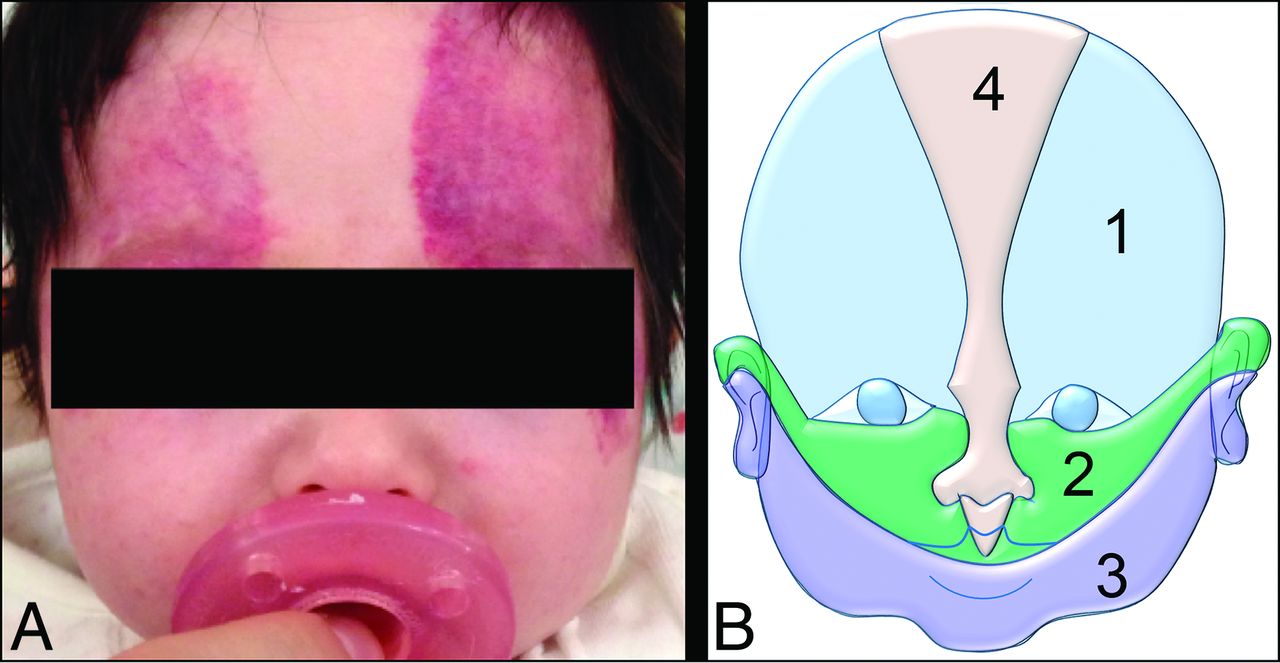
Infantile hemangioma lesions may differ by clinical presentation, location, and morphology; therefore, each lesion may require a different approach. According to the latest update of the International Society for the Study of Vascular Anomalies (2018), IHs are characterized by their distribution pattern: focal, multifocal, segmental, and indeterminate types.7⇓-9 Of the 4 types, focal IHs are the most common, with a round or oval shape representing the most common morphology. Segmental IHs appear as broader geometric lesions that correspond to the embryonic boundaries that exist among the various facial primordia derived from neural crest cells.10 Segmental IHs that cover a broad cutaneous territory (Fig 1) may be associated with hemangioma syndromes and may be detected immediately after birth.11 Deep cutaneous lesions may be diagnosed at several months of age, and they may appear as nonspecific soft-tissue masses.11,12 Segmental IHs may occur in multiple locations within the head and neck, extremities, and/or body.13

Segmental IH. A, A 3-month-old girl with PHACE syndrome. Clinical photograph shows a bilateral segmental IH in an S1 distribution predominantly and with minimal S2 involvement. B, Diagram of the Haggstrom classification, used for clinical assessment of superficial IH distribution. It divides the face on the 4 following segments: S1 = frontotemporal, S2 = maxillary, S3 = mandibular, S4 = frontonasal.
Segmental IHs are a requisite for the diagnosis of hemangioma syndromes, such as posterior fossa brain malformations, hemangioma, arterial lesions, cardiac abnormalities, and eye abnormalities (PHACE).14,15 PHACE syndrome denotes the following: posterior fossa and other structural brain malformations; large hemangiomas of the face, neck, and/or scalp; anatomic anomalies of the cerebral or cervical arteries; cardiac anomalies/coarctation of the aorta; and eye abnormalities.16⇓⇓-19 If sternal anomalies are present, the term “PHACES syndrome” is used, with S standing for sternal anomalies. PHACE syndrome is associated with segmental IHs in the head and neck region with a trigeminal nerve distribution.11,16,17 IHs within the lower body, especially involving the perineal region, may be a marker of the relatively recently defined LUMBAR, SACRAL, or PELVIS association/syndrome.20⇓⇓⇓⇓-25 Hemangioma syndromes are now perceived as a spectrum of manifestations rather than fixed imaging and clinical features.17 The exact criteria for these complex heterogeneous conditions are still under debate, though consensus guidelines for definite-versus-possible PHACE syndrome were introduced in 2016 (Online Supplemental Data).14,26 These consensus criteria may evolve with time as more data on etiology and pathophysiology become available. Nonetheless, the presence of a superficial segmental IH remains the dominant essential feature of these syndromes. Diffuse neonatal hemangiomatosis is another less common hemangioma syndrome with numerous IHs in the skin of the neonate, and it has a high association with visceral and neuroaxial lesions.
Although neuroaxial (intracranial and/or intra-/paraspinal) IHs are rare in the general population, occurring in 1% of all patents with skin hemangiomas,12 several studies have described an increased frequency in patients with hemangioma syndromes.12,27⇓⇓⇓-31 Additional intracranial abnormalities have also been described in PHACE syndrome, including midline anomalies, neuronal migration disorders, and asymmetric enlargement of Meckel's cave.14,32,33
The purposes of our retrospective study include determination of the incidence, location, imaging appearance, and natural history of neuroaxial infantile hemangiomas and their syndromic association. We also assessed additional cerebral and/or cardiovascular abnormalities that were associated with neuroaxial hemangiomas.
MATERIALS AND METHODS
Cohort Selection
After obtaining institutional review board approval, we searched the Children's Hospital of Philadelphia radiology database, Illuminate search software (Softek Illuminate), for patients with segmental IH referred to our institution for imaging and clinical evaluation of suspected underling systemic hemangioma syndromes between 2002 and 2017. We performed Boolean searches using the keywords “segmental,” “infantile hemangioma,” “hemangioma,” “PHACE,” “PELVIS syndrome,” and “MR imaging.” All patients were referred for initial imaging because of cutaneous hemangiomas. Inclusion criteria were the following: 1) the presence of subcutaneous/cutaneous vascular segmental lesions in the head, neck, or trunk; 2) available MR imaging of the brain and spine with contrast administration; and 3) younger than 12 months of age at the time of first imaging (the known timeframe for regression of superficial infantile hemangiomas). Exclusion criteria included technically suboptimal studies due to excessive motion and absence of contrast administration.
Image Interpretation
All imaging was performed on 1.5 or 3T MR imaging scanners, including Skyra, Prisma and Vario Scanners, (Siemens) during the course of routine clinical care. All patients were imaged with standard MR imaging protocol using multiplanar T1- and T2-weighted sequences, FLAIR, diffusion-weighted, arterial spin-labeling perfusion imaging, and multiplanar postcontrast T1-weighted sequences. Specific acquisition parameters varied across time and scanners. Vascular imaging was performed using TOF-MRA. Three pediatric neuroradiologists, blinded to the clinical history, independently retrospectively reviewed MR imaging of the brain and spine for all cases and recorded imaging findings, with a special focus on the following: 1) the presence and imaging characteristics of neuroaxial vascular lesions; 2) abnormalities of the posterior fossa; 3) head and neck vascular anomalies; and 4) additional brain anomalies, including the symmetry of the Meckel cave (MC). A consensus reading was then performed for potential discrepancies. In addition, in those cases that had serial imaging, the temporal evolution of neuroaxial and superficial IHs was assessed.
Clinical Evaluation
Cutaneous IHs involving the head and neck were evaluated by pediatric dermatologists, who used the classification described by Haggstrom et al10,34 (S1 = frontotemporal, S2 = maxillary, S3 = mandibular, S4 = frontonasal, Fig 1B), which corresponds with the embryonic boundaries that exist among the various facial primordia derived from neural crest cells. Additionally, the electronic medical record was queried to obtain relevant clinical and demographic data, specifically age, sex, cardiac history, and the diagnosis of systemic vascular hemangioma syndrome. Available information about the presence of developmental or hearing issues was obtained from patients' charts.
Statistical Analysis
We compared the imaging and clinical findings between the subjects with diagnosed hemangioma syndromes and those with isolated superficial segmental IHs. Continuous variables were not normally distributed and were, therefore, compared using the nonparametric Mann-Whitney U test. Categoric variables were compared using the Fisher exact test. Comparisons within the syndrome group were similarly analyzed. To assess the degree of agreement among the 3 readers, we calculated the Fleiss κ coefficients and interpreted them according to Landis and Koch.35 Statistical analysis was performed on STATA, Version 12.1 (StataCorp) and R statistical and computing software (http://www.r-project.org). A 2-tailed P value <.05 was used for statistical significance.
RESULTS
Subject Characteristics
Ninety-eight subjects with superficial IHs in a segmental distribution were identified from 2002 to 2017. We excluded 3 patients: 2 subjects, both with vascular lesions within the lower spinal canal and diagnoses of LUMBAR/PELVIS syndrome, did not have brain imaging, and 1 who was older than the defined inclusion criteria age range (3 years of age) at initial imaging. The final cohort, therefore, contained 95 subjects, including 42 subjects with diagnosed hemangioma syndromes (41 with a diagnosis of PHACE syndrome and 1 with diffuse neonatal hemangiomatosis) and 53 subjects with isolated segmental skin hemangiomas. The final diagnoses had been made on the basis of a multidisciplinary clinical team specializing in vascular malformations. Subject characteristics are summarized in Table 1.
Characteristics of subjects with IH as part of a hemangioma syndrome compared with isolated IH
Seventy-seven subjects (81%) were female, without a significant difference in rates between subjects with syndromic and isolated segmental IH (74% versus 86%, P = .12). The median age of the subjects at the time of imaging was 2 months (range, 0.5–11 months), and it was not significantly different between syndromic and nonsyndromic subjects (P = .53). Among the patients with identified hemangioma syndromes, 93% of patients (39/42) had segmental facial hemangiomas, 2 (5%) had body truncal surface hemangiomas, and 3 (8%) had hemangiomas of the tongue, subglottis, or upper airway (2 patients had IHs in multiple locations). Nonsyndromic subjects had a similar proportion of facial hemangiomas (96% [51/53], P = .65), with neck IHs in 4 subjects and a midchest IH in 1.
Neuroaxial IH
Twenty subjects were found to have neuroaxial IH, all of whom had identified hemangioma syndromes (20/42): 15 with only intracranial IHs, 1 with only a paraspinal IH, and 4 with both. The agreement among the 3 readers for the presence and location of neuroaxial IH was almost perfect for all locations, with κ ranging from 0.85 to 1.00 (Table 2).
Locations of neuroaxial IH and agreement between 3 readers
All intracranial lesions were ipsilateral to the cutaneous hemangiomas. Intracranial IHs were more prevalent in patients with S1 segment lesions compared with subjects without S1 segment IHs (59% versus 20%, P = .023). There were no significant differences in the prevalence of intracranial IH in subjects with S2 (62% versus 29%, P = .06), S3 (39% versus 50%, P = .54), or S4 (67% versus 39%, P = .26) segment IHs compared with those without those segmental lesions. The prevalence of intracranial IHs in syndromic subjects with all 4 facial segments involved unilaterally was found to be 83% compared with subjects with ≤3 segments (39%), though this was not statistically significant (P = .08).
Imaging Features
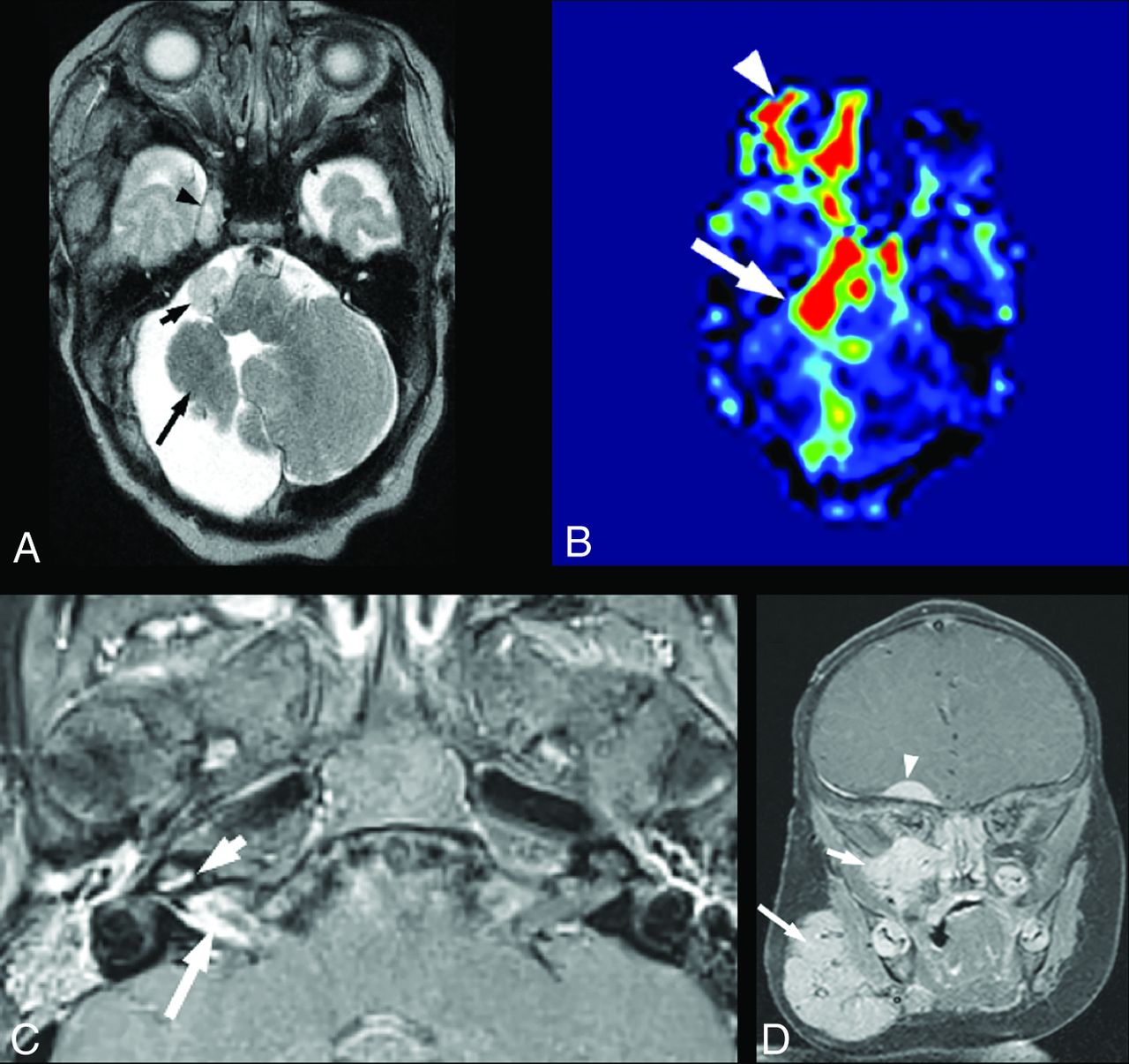
Imaging features of neuroaxial mass lesions were similar to those of superficial infantile hemangiomas. Briefly, the lesions were T1 isointense, T2 hyperintense compared with brain parenchyma, and enhanced diffusely, with markedly increased perfusion on arterial spin-labeling sequences (Fig 2 A, -B). None of the lesions demonstrated reduced diffusion.
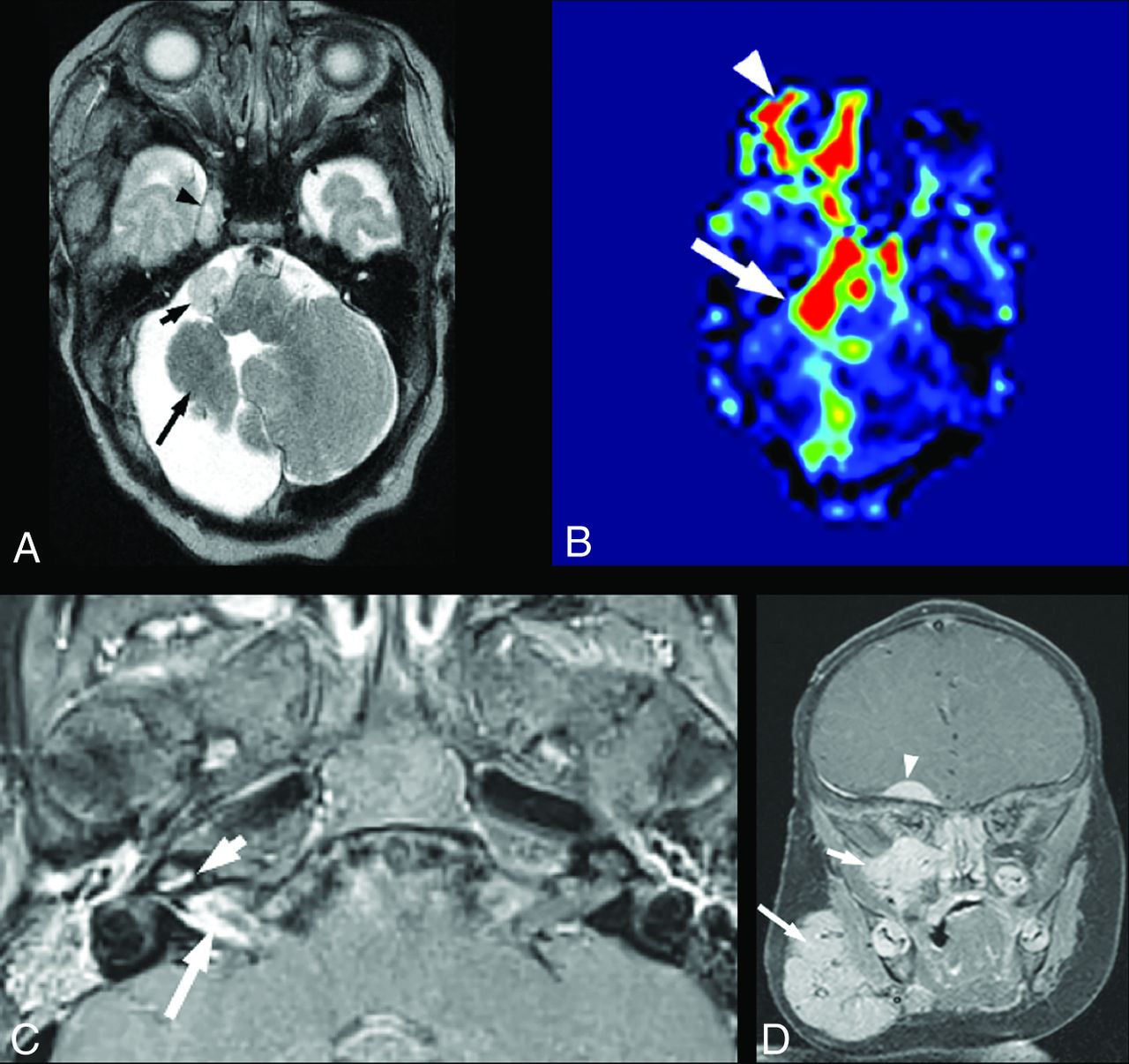
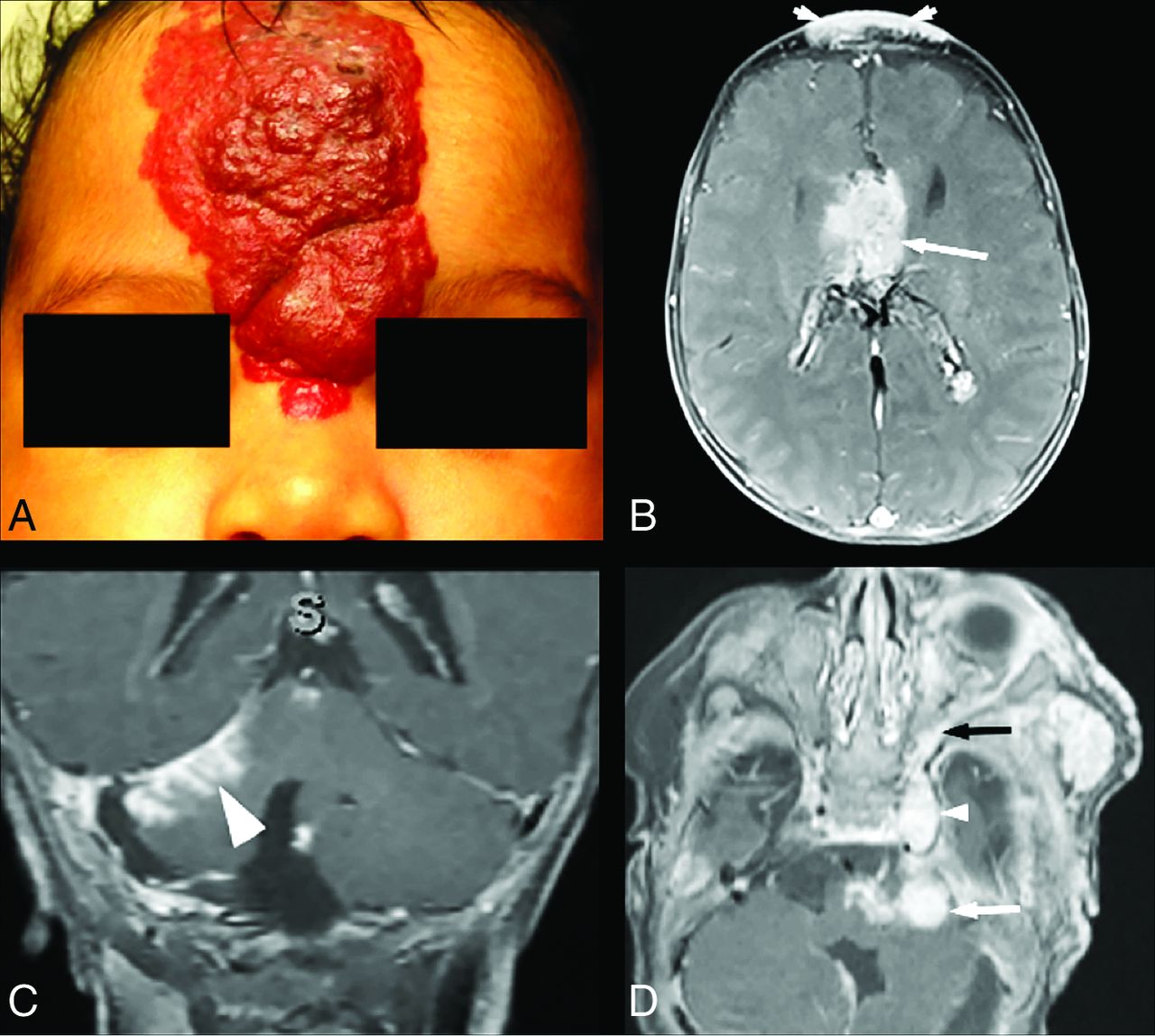
Intracranial infantile hemangioma. A and B, A 1.5-month-old girl with segmental IH of the right face and PHACE syndrome. A, Axial T2-weighted image shows an extra-axial T2-hyperintense mass in the right cerebellopontine angle cistern (small arrow) and a similar lesion in the enlarged right MC (arrowhead). A long arrow points to an asymmetrically small right cerebellar hemisphere, which is an additional common manifestation of PHACE syndrome. Both lesions reveal diffuse enhancement on postcontrast imaging and markedly increased perfusion on arterial spin-labeling imaging (B). C, A 3-month-old girl with right orbital segmental IH and PHACE syndrome. Axial postcontrast T1-weighted image with fat suppression shows linear enhancement in the right IAC (large arrow) and linear enhancement of the cochlear basal turn (arrowhead). D, A 2-month-old girl with segmental IH of the right face and PHACE syndrome. Coronal postcontrast T1-weighted image with fat suppression shows a dural base extra-axial enhancing mass in the right frontal lobe undersurface (arrowhead). Additional IHs are demonstrated in the right face (large arrow) and the right skull base and inferior orbit (small arrow).
Intracranial IHs most often presented as enhancing extra-axial masses in variable locations. The distribution of intracranial IHs is summarized in Table 2. Of the 19 subjects, the most common intracranial IHs were located within the internal auditory canals (IACs) (n = 15) and at the cerebellopontine angle (n = 5). There was substantial variation in size, ranging from a few millimeters of focal enhancement to rounded 1.5-cm tumors. Three of the lesions within the IAC demonstrated cochlear involvement of varying degrees (Fig 2C). Three of the 15 patients (20%) with IAC involvement had hearing loss. One had severe ipsilateral sensorineural hearing loss, 1 had mild sensorineural hearing loss at 6 months of age that resolved by 4 years of age, and 1 had early conductive hearing loss that resolved later. The cause of the conductive hearing loss is unknown. Five patients (33%) had normal hearing, and the hearing results of the remaining 8 patients were not available in our retrospective review.
The other intracranial masses were dural-based lesions in the anterior and middle cranial fossa (n = 4), extending along the anterior surface of the frontal or the temporal lobes (Fig 2D). Small masses in the sella turcica and basal cisterns were seen in 4 patients. In several cases, there was extension of vascular masses through the skull base foramina, which included MC (n = 2), cavernous sinus (n = 2), pterygopalatine fossa (n = 1), and vidian canal. One patient with an isolated large IH of the forehead in the S4 segment had complete agenesis of the corpus callosum and an interhemispheric vascular mass (Fig 3A, -B). An additional pattern of intracranial IH consisted of foci of leptomeningeal enhancement (Fig 3C), observed in 10 subjects. Intracranial IHs were found in multiple locations in 11/19 subjects. No definite connection between intracranial and superficial IHs was demonstrated in all cases, though skull base foraminal lesions involving the ipsilateral cavernous sinus, vidian canal, hypoglossal canal, or orbital fissures were in close proximity to the superficial cutaneous lesions (Fig 3D).

Intracranial infantile hemangioma. A and B, A 2-month-old girl, born with a very large segmental IH of the forehead. A, Clinical photograph shows an IH in the S4 segment (according to the Haggstrom classification). B, Axial postcontrast T1-weighted image with fat suppression of the same patient shows a lobulated enhancing interhemispheric mass (arrow). A superficial forehead IH is indicated by arrowheads. C, A different 2-month-old girl with right facial IH and PHACE syndrome. Coronal postcontrast T1-weighted image with fat suppression shows focal leptomeningeal enhancement along the right tentorium (arrowhead). D, A 1.5-month-old boy with left facial IH. Axial postcontrast T1-weighted image with fat suppression shows enhancing hemangiomas in the left cerebellopontine angle cistern (white arrow) and in the enlarged left MC (small white arrowhead) and enhancing vascular tissue along the lateral orbital wall (black arrow), which seems to communicate between the intra- and extracranial components.
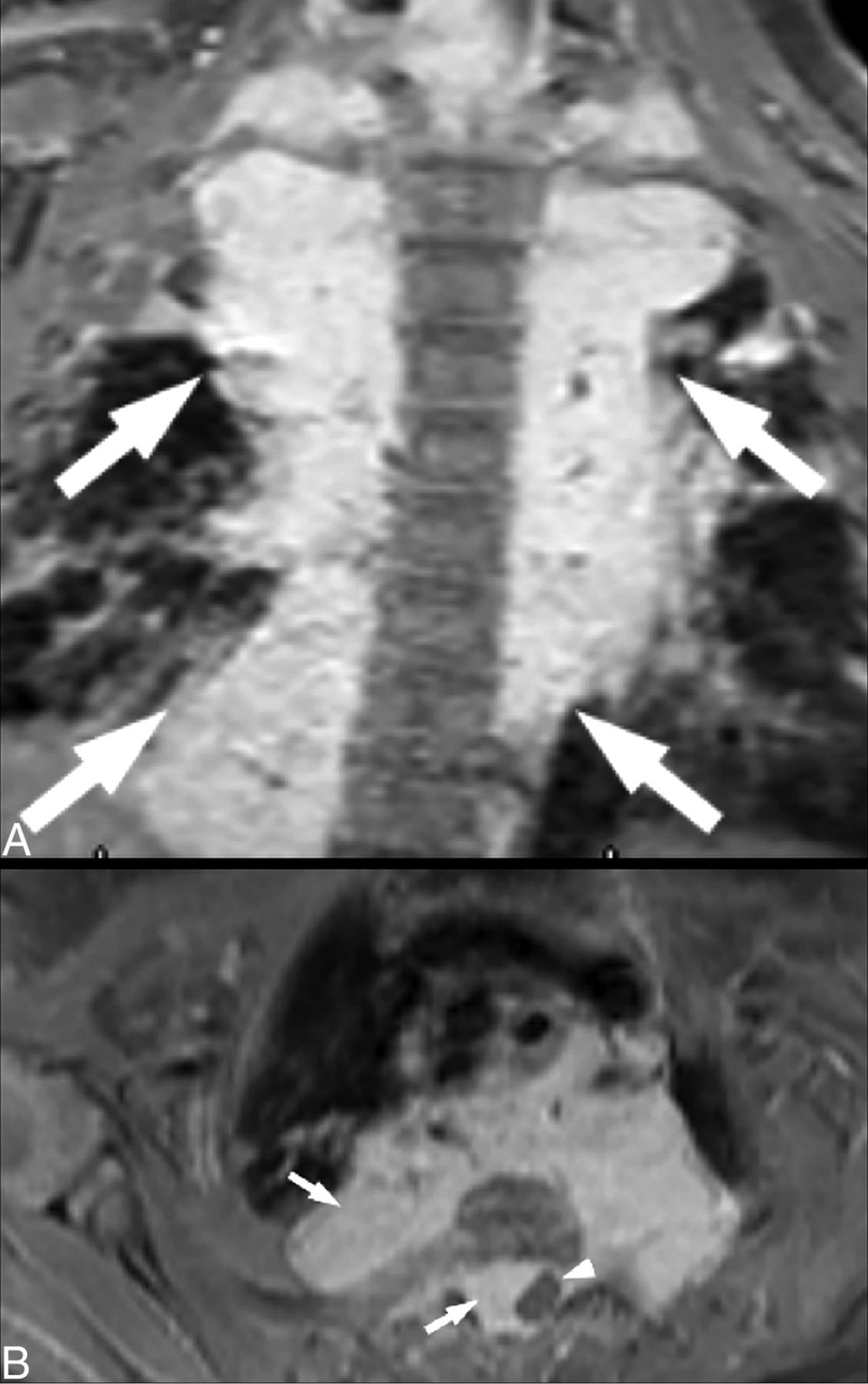
The intra-/paraspinal vascular masses were all extradural and varied from small unilateral lesions, spanning 1 or 2 vertebral segments, to large bilateral masses causing cord compression on imaging in 1 patient (Fig 4). None of the neuroaxial lesions originated in or invaded the cerebral parenchyma or the spinal cord.
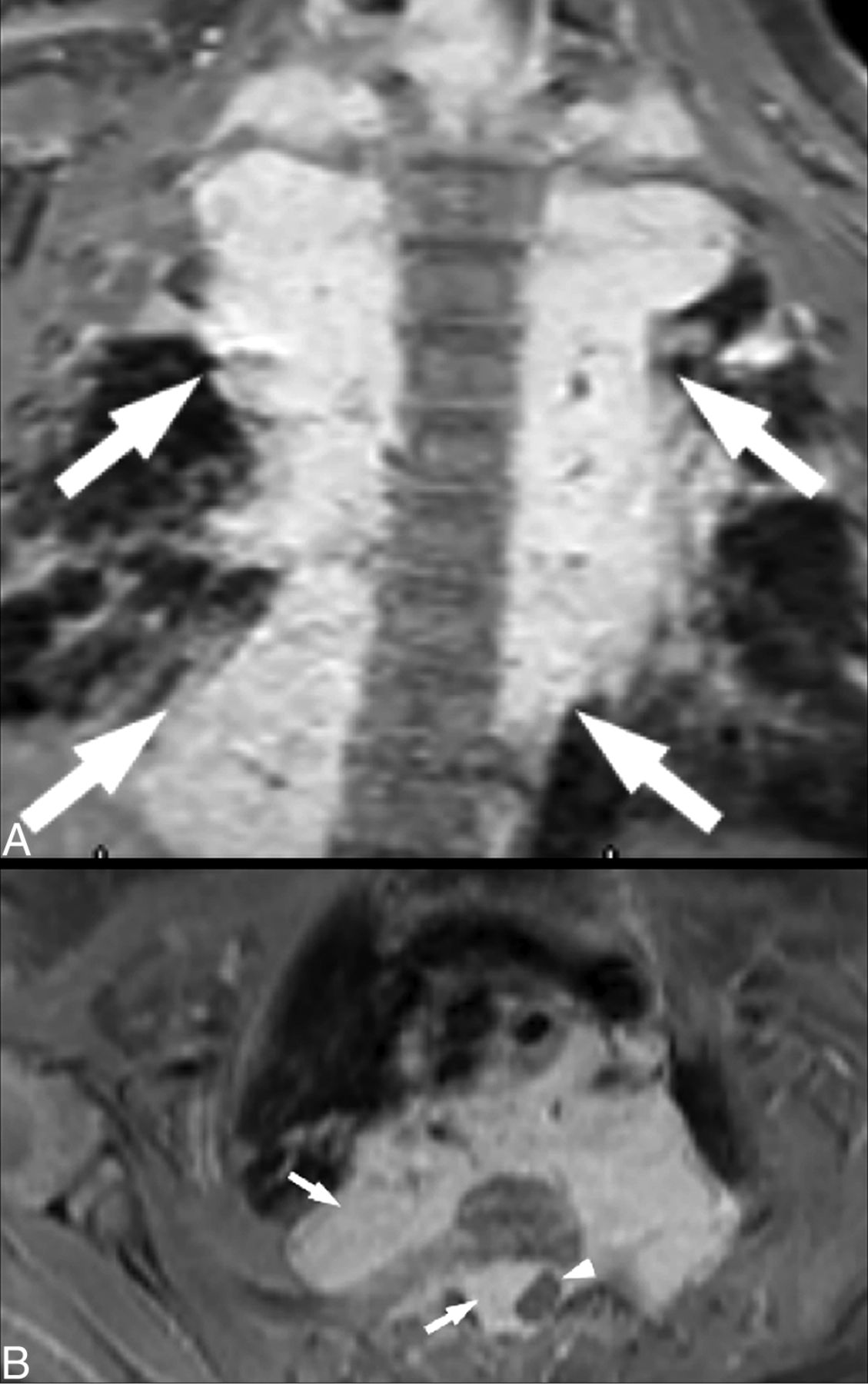
Paraspinal IH. A 2-month-old girl with face and neck segmental IH. Coronal (A) and axial (B) postcontrast T1-weighted images with fat suppression show extensive bilateral enhancing paraspinal masses along the thoracic spine (arrows), with extension into the spinal canal and focal cord compression (arrowhead).
Neuroaxial IH Follow-up
Of the 19 subjects with intracranial IHs, 10 underwent follow-up MR imaging with contrast and 3 underwent follow-up MR imaging without contrast. Of those 10, the median follow-up was 5 years (interquartile range, 2–7 years). Five intracranial IHs resolved completely, 4 demonstrated partial resolution, and 1 lesion in the IAC had no change during 2 years of monitoring. In the 1 subject with only a paraspinal IH, resolution was demonstrated after 12 years. Only 1 case of recurrence of an intracranial IH was demonstrated, which occurred simultaneous to the recurrence of skin lesions occurring after propranolol (beta blocker) therapy was weaned.
Meckel Cave Asymmetry
Unilateral asymmetric enlargement of the MC (Figs 2A, 3D, and 5A) was observed in 28/42 cases with an identified syndrome (67%), in 17/20 cases with neuroaxial vascular lesions (85%), and in no patients without an identified syndrome (0%) (P < .001). MC enlargement was associated with S1 segmental facial hemangiomas, occurring in 85% (23/27) of syndromic subjects with S1 IH, compared with 33% (5/15) of those with segments other than S1 (P = .001). No significant association was found with MC enlargement and S2–S4 segment involvement. MC enlargement was not noted in subjects with only para-/intraspinal neuroaxial IHs.

A, Asymmetrical enlargement of Meckel's cave in patients with PHACE syndrome, an illustration showing a relationship between skull base hemangioma and adjacent nerves and vascular structures. Modified from a previously published image.33 B, Posterior fossa abnormality in patients with PHACE syndrome. A 6-week-old girl with a left facial IH. An axial T2-weighted image shows an enlarged retrocerebellar CSF space (black arrow), an asymmetrically small left cerebellar hemisphere (white arrow), and a small posterior vitreous coloboma in the left globe (arrowhead), which is another infrequent feature of PHACE syndrome. C, Arteriopathy of PHACE syndrome. A 6-month-old girl with a right-face IH and PHACE syndrome. Coronal TOF-MRA reconstructed image shows the diffusely small caliber of intracranial right ICA (arrow). Fig 5A courtesy of Malhotra, A., Tu, L., Kalra, V.B. et al. Neuroimaging of Meckel's cave in normal and disease conditions. Insights Imaging 9, 499–510 (2018). https://doi.org/10.1007/s13244-018-0604-7.
Posterior Fossa Abnormalities
Twenty of 42 subjects with syndromic hemangiomas (48%) demonstrated anomalies of the posterior fossa. Those included inferior vermian hypoplasia (n = 14), hypoplasia of a cerebellar hemisphere (n = 13), and Dandy-Walker malformation (n = 4) (Fig 5B). No posterior fossa abnormalities were identified in the nonsyndromic patients (P < .001), which would be expected because they are part of the definition of PHACE. In patients with identified hemangioma syndromes, the prevalence of posterior fossa abnormalities was similar between patients with and without neuroaxial IHs (40% versus 50%, P = .55). No association was found between the location of the segmental facial IH or intracranial IH and the presence of posterior fossa abnormalities (P > .05 for all comparisons). Unilateral MC enlargement was found more frequently in syndromic subjects with posterior fossa abnormalities than in those without posterior fossa anomalies (85% versus 48%, P = .020) (Fig 5).33 Sex was not associated with the presence of intracranial IHs, an enlarged MC, or posterior fossa abnormalities (P > .05).
Cardiovascular Abnormalities
Ninety-five percent (40/42) of patients with hemangioma syndromes had cardiovascular anomalies, ranging from minor developmental variants to severe dysplastic vasculopathy of the large arteries (Fig 5B), including aortic arch anomalies and cardiac defects. We did not observe serious vascular events or ischemic lesions in our group, though 1 patient was treated with pial synangiosis in response to developing Moyamoya vasculopathy identified after presenting with headaches on presymptomatic brain MR imaging.
DISCUSSION
Most authors agree that infants presenting with large segmental hemangiomas of the head, neck, chest, and lower body may be manifesting an underlying hemangioma syndrome; hence, careful patient work-up is recommended.36 We found that 42% of patients referred to our institution with segmental IHs who underwent brain and/or neck and spine imaging were ultimately diagnosed with an underlying hemangioma syndrome, PHACE, and diffuse neonatal hemangiomatosis.
We detected a high rate of neuroaxial lesions in the group with confirmed hemangioma syndromes (48% of our subjects), substantially higher than reported in the general population.29⇓-31 The reason for this higher prevalence is not entirely clear, but possible reasons include the resolution of our multiplanar imaging, the presence of multiplanar postcontrast imaging in all cases, and the focus of the study team on the detection of neuroaxial lesions. The lesions were extra-axial without parenchymal involvement and extradural in location within the spine, corresponding to the existing literature.3,11,12,16,18,27⇓⇓-30,37 The most common location of intracranial hemangiomas in our cohort was the auditory apparatus. The degree of involvement varied from subtle linear enhancement of the vestibulocochlear nerve or basal turn of the cochlea to large masses extending from the cerebellopontine angle and filling the IAC and cochlea. Duffy et al38 reported an under-recognized association of hearing loss with PHACE syndrome in 6 patients, emphasizing the variety of clinical manifestations in patients with auditory lesions. The data from our series indicating a high prevalence of internal auditory canal involvement add to this literature. Some authors suggest dedicated imaging of the auditory apparatus, as well as thorough assessment of auditory functions in patients with superficial hemangiomas involving the external ear,27,39 though as we have shown, IAC hemangiomas can be seen in patients having segmental hemangiomas in segments not involving the external ear. Even subtle imaging findings of auditory apparatus involvement with hemangiomas may, therefore, result in a monitoring strategy toward a more detailed clinical evaluation and imaging follow-up. In one of our patients, there was improvement of sensorineural hearing loss. It is possible to speculate that the timing of auditory testing may influence the hearing test results because there are changes in the size of the IAC hemangiomas with time. The long-term effect of internal auditory apparatus involvement by IH is not fully known, to our knowledge.
Enhancing dural-based masses were present in approximately 12% of subjects, which demonstrated imaging features in some ways similar to meningiomas. This type of vascular lesion should be added to a list of differential lesions mimicking meningioma if visualized in the appropriate clinical setting.37 In 1 case, the small dural-based hemangioma was the only intracranial vascular mass present, representing the pertinent feature contributing to the diagnosis of PHACE syndrome.
Wright and Wycoco32 reported asymmetric MC enlargement as an imaging marker highly supportive a diagnosis of PHACE syndrome. They reported that 82% of patients with confirmed PHACE syndrome revealed asymmetric MC enlargement and that this finding has a positive predictive value of 100%, a negative predictive value of 91%, and an accuracy of 93% in predicting a clinical diagnosis of PHACE or possible PHACE syndrome. We found MC asymmetry in 67% (28/42) of patients with hemangioma syndromes, noting a particularly high frequency (85%) of unilateral MC enlargement in patients with coexisting intracranial lesions, without MC asymmetry in the isolated superficial IH group. We observed a statistically significant association of MC enlargement with superficial segmental facial IH in the distribution involving the frontotemporal segment (S1); this observation is concordant with the literature.32 Several theories have been suggested to explain this finding. Early hemangioma involvement of the trigeminal V1 division traversing the MC, which may be small or have regressed by the time of imaging, could influence fluid dynamics and may cause remodeling of the affected MC. Additionally, IHs secrete numerous signaling factors that affect multiple cell types, including osteoblasts and meningeal cells, as well as changes in local endothelial proliferation via the vascular endothelial growth factor, Insulin-like growth factor and other growth factors.40
Another theory of MC enlargement proposes an aberrant/deficient migration of the cephalic neural crest in a metameric distribution, noting a common origin of skull base tissues and trigeminal nerve ganglia. It assumed that a postzygotic mutation or early prenatal insult to the fetal skull base may cause dysplasia of the MC.32 Although being highly suggestive of the diagnosis of PHACE, this sign was not seen in all cases, especially in patients with symmetric or midline face or neck lesions. Most interesting, we found a higher rate of MC enlargement than posterior fossa abnormalities in PHACE syndrome. An additional study with follow-up monitoring of imaging findings and clinical data may elucidate the significance of an asymmetric MC. Overall, our findings support asymmetric enlargement of the MC as highly suggestive of an underlying diagnosis of PHACE syndrome in the appropriate clinical setting.
The pattern of facial segmental IH distribution may help in predicting underlying structural defects.41 We observed a high frequency of intracranial hemangiomas in patients with S1 segmental facial hemangiomas, as well as multiple segments involved, which is in concordance with literature data.17 Therefore, the presence of S1 and/or multisegmental superficial segmental IH mandates a careful imaging search for even subtle neuroaxial hemangiomas. Viswanathan et al12 reported clear continuity of neuroaxial lesions with subcutaneous/cutaneous lesions. In our cohort, a definite connection between intracranial vascular masses and its superficial counterpart was not demonstrated in all cases, though skull base foramina lesions were seen in close proximity to the superficial cutaneous lesions.
A high percentage of all patients had cardiovascular anomalies, ranging from minor developmental variants to severe dysplastic vasculopathy of large arteries, including aortic arch anomalies and cardiac defects. However, PHACE syndrome is rarely associated with progressive vascular disease, and we did not observe serious vascular events or ischemic lesions in our group, though 1 patient was treated with synangiosis in response to the development of Moyamoya vasculopathy (this patient had been treated with systemic steroids, not propranolol).42 Although the intracranial lesions mostly regressed on available follow-up imaging, some of the residual lesions remained visible at 4–5 years of age. One patient did have recurrence of intracranial IH at 3 years of age, which was simultaneous with the recurrence of skin lesions. Decisions regarding the scheduling of follow-up imaging may, therefore, be considered on a case-by-case basis rather than only in the event of new neurologic signs or symptoms.
Our study has limitations inherent to the retrospective design. Because our institution is a referral center, the overall rate of subjects with facial segmental IH with hemangioma syndromes may have been higher in our study compared with the general population. However, it is unlikely that this rate affected the differences in rates of neuroaxial IH and other findings associated with such syndromes. Imaging studies were retrospectively reviewed and could not be tailored to specific indications as needed. Neuroimaging of 2 subjects with LUMBAR/PELVIS syndrome was not available; therefore, these patients were excluded from the study. Additionally, follow-up imaging in the retrospective cohort was inconsistent, and a formal assessment of the longitudinal pattern of neuroaxial lesions was not possible. Clinical data were limited to what was available in the electronic medical record.
The results of our study suggest the necessity of a methodic approach in the evaluation of patients with segmental IH. These patients require a thorough imaging search for vascular lesions involving the neural axis. Imaging usually begins with brain MR imaging, occasionally neck MR imaging (if the superficial lesion involves the neck), and vascular MR imaging, including head and neck MRA with TOF or dynamic MRA with contrast if indicated. Contrast administration may be considered in cases of S1 and/or multisegmental distribution of IH, which is notable for a higher association of intracranial or intraspinal lesions. We demonstrate spinal involvement by neuroaxial hemangiomas in a subset of the patients. However at this point, beyond increasing awareness of spinal involvement, no firm conclusion can be drawn for changing clinical practice or the necessity of spinal imaging in this group of patients without further knowledge of the short- and long-term clinical implications of these spinal neuroaxial hemangiomas.
CONCLUSIONS
Although CNS involvement by IH is an overall unusual occurrence, a substantial number of pediatric patients with hemangioma syndromes, especially PHACE syndrome, have a high rate (48%) of neuroaxial lesions. Therefore, detection of neuroaxial IHs may be potentially considered as one of the criteria for diagnosis of this hemangioma syndrome. The neuroaxial lesions appear to behave similar to superficial lesions (imaging features and clinical course of development and regression). The neuroaxial IHs were not demonstrated in patients with isolated cutaneous segmental IHs. Further studies would be necessary to determine how these findings may influence the management and potential implications of neuroaxial lesions on patient development.
Footnotes
Disclosures: Tamara Feygin—UNRELATED: Employment: The Children's Hospital of Philadelphia. Aashim Bhatia—UNRELATED: Consultancy: Guerbet. Avrum Pollock—UNRELATED: expert testimony A. Pollock MD, LLC.
References
- Received November 24, 2020.
- Accepted after revision January 14, 2021.
- © 2021 by American Journal of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.