
Abstract
Summary: We report an unusual case of Kimura's disease. An 81-year-old Japanese woman was shown to have bilateral auricular masses that had begun to enlarge 6 years before. On CT scans, slightly high-density masses with faint contrast enhancement were seen. The masses were heterogeneous and hypointense on T1-weighted MR images, were slightly hyperintense on T2-weighted MR images, and showed heterogeneous enhancement after the administration of contrast material. Kimura's disease should be included in the differential diagnosis of bilateral auricular tumors.
Kimura's disease is a chronic inflammatory disorder of unknown origin (1–8). The most common clinical feature of this disease is an asymptomatic unilateral soft-tissue mass in the head and neck, and major salivary glands and lymph nodes are frequently involved (1). Bilateral involvement is rare. We herein report an unusual case of this disease, which presented as bilateral auricular masses.
Case Report
An 81-year-old Japanese woman was admitted to our hospital with complaints of almost synchronous bilateral auricular masses that had begun to enlarge 6 years before admission and were accompanied by itchiness. At admission, the laboratory data showed 25% eosinophilia, zinc sulfate turbidity elevated to 15.5 U (normal range, 4.0–12.0 U), and alkaline leukocyte phosphatase elevated to 434 IU/mL (normal range, 85–340 IU/mL). There was no elevated tumor marker level, such as carcinoembryonic antigen, carbohydrate antigen 19-9, or α-fetoprotein. The serum immunoglobulin E level was not obtained.
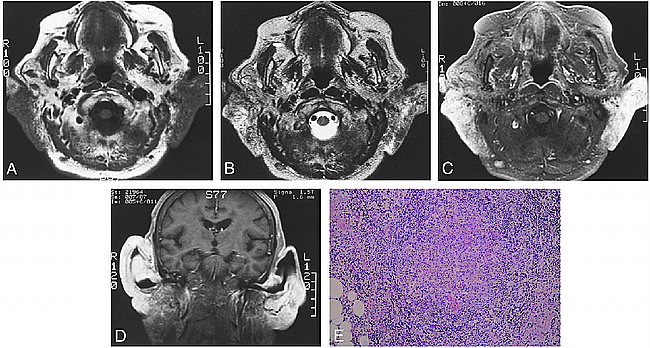
CT was performed with and without injection of contrast material and showed slightly high-density masses with faint contrast enhancement in the bilateral auricles, parotid glands, and retroauricular regions. MR imaging showed heterogeneous hypointense masses on T1-weighted images (Fig 1A) and slightly hyperintense masses on T2-weighted images (Fig 1B). The masses were heterogeneously enhanced with the administration of 0.2 mmol/kg gd-DTPA (Fig 1C–D). Enlarged bilateral cervical lymph nodes were also enhanced homogeneously. Surgical resection of the bilateral auricular masses was undertaken (Fig 1E). Microscopically, the masses had marked infiltration of eosinophils and lymphocytes with germinal centers and proliferation of many blood vessels and thick fibrotic tissues, compatible with Kimura's disease.
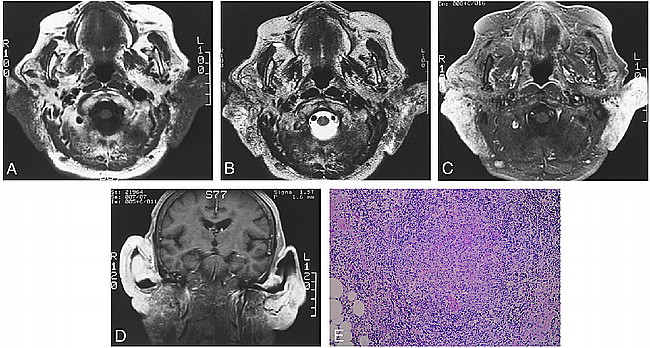
Images from the case of an 81-year-old Japanese woman who was admitted to our hospital with complaints of almost synchronous bilateral auricular masses that had begun to enlarge 6 years before admission and were accompanied by itchiness.
A, T1-weighted MR image (440/19/2 [TR/TE/excitations]) shows irregular masses in the bilateral auricles, parotid glands, and retroauricular spaces, which are heterogeneous and hypointense compared with the muscles.
B, T2-weighted MR image (4000/108/2) shows that the masses are hyperintense.
C, After the administration of contrast material, a T1-weighted axial view image (540/16/1.5) shows heterogeneously enhancing masses involving both auricles. Enlarged bilateral cervical lymph nodes were also noted and showed homogeneous enhancement.
D, Contrast-enhanced T1-weighted coronal view image (400/11/2) shows heterogeneously enhancing masses involving both auricles.
E, Microscopically, marked infiltration of eosinophils and lymphocytes with germinal centers and proliferation of many blood vessels and thick fibrotic tissues are seen, compatible with Kimura's disease (hematoxylin and eosin stain; original magnification, ×40).
Discussion
Kimura's disease is a chronic angiolymphoid proliferative disorder. This disease has male predominance and occurs mostly during the second and third decades of life, endemically in Asia, especially in Japan and China (2–4). As a clinical manifestation, asymptomatic unilateral soft-tissue swellings, such as salivary glands and local lymph nodes, are most common. Other less common involved areas include the axillary, inguinal, and popliteal regions (1). On the other hand, auricular involvement has been reported as a rare event. Kase et al (2) reported only one case involving mainly the auricle among 130 patients with this disease. Bilateral auricular involvement is thought to be extremely rare, and no such case has been reported in the English-language scientific literature. The histopathologic findings of this disease consist of hyperplasia of germinal centers and infiltrations of polykaryocytes, eosinophils, blood vessels, and fibrotic changes. These findings of Kimura's disease may mimic angiolymphoid hyperplasia with eosinophilia, but these diseases are thought to be different entities (5). The cause of Kimura's disease remains unknown but is thought to be related to allergic reaction, because the patients often have eosinophilia and high serum immunoglobulin E. Complications such as atopic dermatitis, allergic rhinitis, asthma, and urticaria occur among patients with Kimura's disease, but we cannot find any report of the incidence of the complications. Moreover, the histopathologic findings may support this opinion. In this case, eosinophilia and itchiness were observed. Three therapies are predominantly chosen: corticosteroid therapy, radiation therapy, and surgical resection. Recurrence is common, however, especially when only resection is used, and there has been no definitive treatment to cure this disease (2). We think the initial treatment should be conservative, such as corticosteroid therapy. If no effect is achieved, surgical or radiation therapy can then be considered. The recurrence rate is lower when two or more therapies are combined.
There are many reports concerning CT and MR imaging findings of Kimura's disease. On CT scans, irregularly shaped subcutaneous mass or masses and swelling of the salivary glands are typical findings (6). On contrast-enhanced CT scans, enlarged lymph nodes are enhanced homogeneously, although the salivary glands are enhanced heterogeneously (7, 8). The masses are iso- or hypointense on T1-weighted MR images and are hyperintense on T2-weighted MR images, compared with the parotid gland (2, 8). Nonetheless, there is a case report showing low signal intensity compared with normal parotid gland on T2-weighted images because of the fibrotic change (4). Thus, the MR findings of Kimura's disease are variable and are thought to depend on vascularity and fibrosis. The findings of CT and MR imaging in our case were compatible with Kimura's disease, except for bilateral involvement.
Many diseases involve bilateral auricles or surrounding tissue near the parotid glands. Differential diagnoses include parotid tumors, malignant lymphomas, neurofibromatosis, malignant tumors originated from cutaneous or subcutaneous tissues, metastatic tumors, and inflammatory diseases. Simultaneous occurrence of tumors in both parotid glands has been reported. These include Warthin's tumor, acinic cell carcinoma, and oncocytoma (9–11). These parotid tumors are usually encapsulated and are almost limited to the parotid gland, although the lymph nodes of the periparotid region can be involved. Lymphoma or metastatic lymphadenopathies may involve the neck bilaterally (12, 13). Long clinical courses, however, as in Kimura's disease, are unusual.
Among inflammatory lesions, tuberculosis and acquired immunodeficiency syndrome should be ruled out. On imaging studies, tuberculosis may show bilateral cervical lymphadenopathies, which tend to have a ring-like contrast enhancement. Bilateral parotid enlargement occurred in patients who had tested HIV-positive and were known to have bilateral parotid cystic lesions (14). Nevertheless, we cannot find any report of Kimura's disease accompanying a ring-like contrast enhancement or cystic components.
Although there are many diseases that are associated with bilateral cervical tumors, Kimura's disease should be included in the differential diagnosis. We think that it is not difficult to diagnose this disease by precise analysis of the characteristics of the clinical history and imaging findings.
Footnotes
↵1 Address reprint requests to A. Hiwatashi, Department of Radiology, Saiseikai Fukuoka General Hospital, 1-3-46 Tenjin, Chuo-ku, Fukuoka 810-0001, Japan.
- Received April 13, 1999.
- Copyright © American Society of Neuroradiology




{kind=link}