
Abstract
BACKGROUND AND PURPOSE: To our knowledge, sonographic findings in the neopharynx have not been well characterized. We describe our results and assess the role of sonography versus CT in patients who have undergone total laryngectomy.
METHODS: We examined 25 patients (24 men and one woman; 44–78 years old) who had had a total laryngectomy. Sonography (with a 10-MHz transducer) and contrast-enhanced CT were performed in all patients. We evaluated the normal shape of the neopharynx and assessed the accuracy of sonography versus CT in detecting tumor recurrence in the neck.
RESULTS: The neopharynx appears as a round or ovoid structure on imaging studies. On sonograms, the neopharyngeal wall has five layers of alternating echogenicity: an innermost hyperechoic layer of superficial mucosa, an inner hypoechoic layer of deep mucosa, a middle hyperechoic layer of submucosa, an outer hypoechoic layer of muscle, and an outermost hyperechoic layer of adventitia. On CT scans, the neopharynx appears as a three-layered structure, with an inner hyperdense layer of mucosa, a middle hypodense layer of submucosa, and an outer isodense layer of pharyngeal constrictor muscles. Nine pathologically proved recurrences were found: three local recurrences, one local recurrence with lymph node metastasis, and five cases of lymph node metastasis only. One instance of false-negative lymph node metastasis was seen at sonography and one case of false-positive local recurrence was seen at CT.
CONCLUSION: The neopharynx has a unique sonographic appearance, and this imaging technique is useful for detecting local tumor recurrence in the neopharynx in patients who have had a total laryngectomy.
Radiologic studies are helpful in the evaluation of patients who have undergone total laryngectomy, because clinical evaluation is limited by postsurgical scarring and radiation fibrosis. CT and MR imaging are the most common techniques used for follow-up studies (1–4), whereas sonography has been used primarily for the detection and guided biopsy of neck nodes (5–7) and for the evaluation of the larynx in infants and children (8). The normal larynx is difficult to evaluate with sonography, owing to the interposed laryngeal skeleton, but there are no obstacles to sonographic evaluation in patients who have had a total laryngectomy. We describe the sonographic appearance of the neck after total laryngectomy and compare these findings with the appearance on CT scans.
Methods
Twenty-five patients (24 men and one woman; 44–78 years old; mean age, 63 years) who had had a total laryngectomy between September 1997 and June 1998 were included in this study. Primary tumors included 21 laryngeal carcinomas (11 supraglottic, seven glottic, and three transglottic), three hypopharyngeal carcinomas, and one oropharyngeal carcinoma. Twenty-two patients had stage IV disease, two had stage III, and one had stage I. One patient with stage I disease underwent total laryngectomy because of verrucous hyperplasia of the entire glottis with associated verrucous carcinoma. Eleven patients underwent postoperative radiation therapy (5940–6480 cGy).
Two radiologists performed the sonographic examinations with a 10-MHz transducer (VST Master Series, Diasonics, Milpitas, CA) immediately after the CT studies; neither was aware of the CT findings or the clinical data. The entire neopharynx and lymph node groups were evaluated, including the bilateral internal jugular, the spinal accessory, the submandibular, and the submental chains. Axial CT scans were obtained after the patients were given an intravenous bolus injection of 100 mL of contrast material. Scans were performed with contiguous 7-mm-thick sections from the hard palate through the upper thorax. The same radiologists assessed the CT scans, with knowledge of the sonographic findings, and the sonograms and CT scans were interpreted in concert by consensus. The interval between total laryngectomy and imaging ranged from 4 to 96 months (mean, 33 months). The follow-up period ranged from 18 to 27 months (mean, 22 months).
The shape of the neopharynx and the thickness and echogenicity/density of the neopharyngeal wall were evaluated. We also evaluated the ability of sonography to depict recurrent disease. A lesion was considered to be a locally recurrent tumor if sonograms and CT scans showed focal neopharyngeal wall thickening or a mass abutting the neopharynx. Criteria for establishing metastatic lymph nodes were as follows: a round shape, a size greater than 1 cm, a grouping of three or more lymph nodes on sonograms and CT scans, effacement of the fatty nodal hilum on sonograms, and rim enhancement on CT scans (5).
Results
On axial images, the neopharynx appeared as an ovoid-to-round structure located between the subcutaneous tissue of the anterior part of the neck and the prevertebral muscles. It often contained air within its lumen, especially at the level of the tongue base. The thickness of the neopharyngeal wall was 4 to 11 mm (mean, 5.6 mm), with the proximal portion thicker than the distal portion.
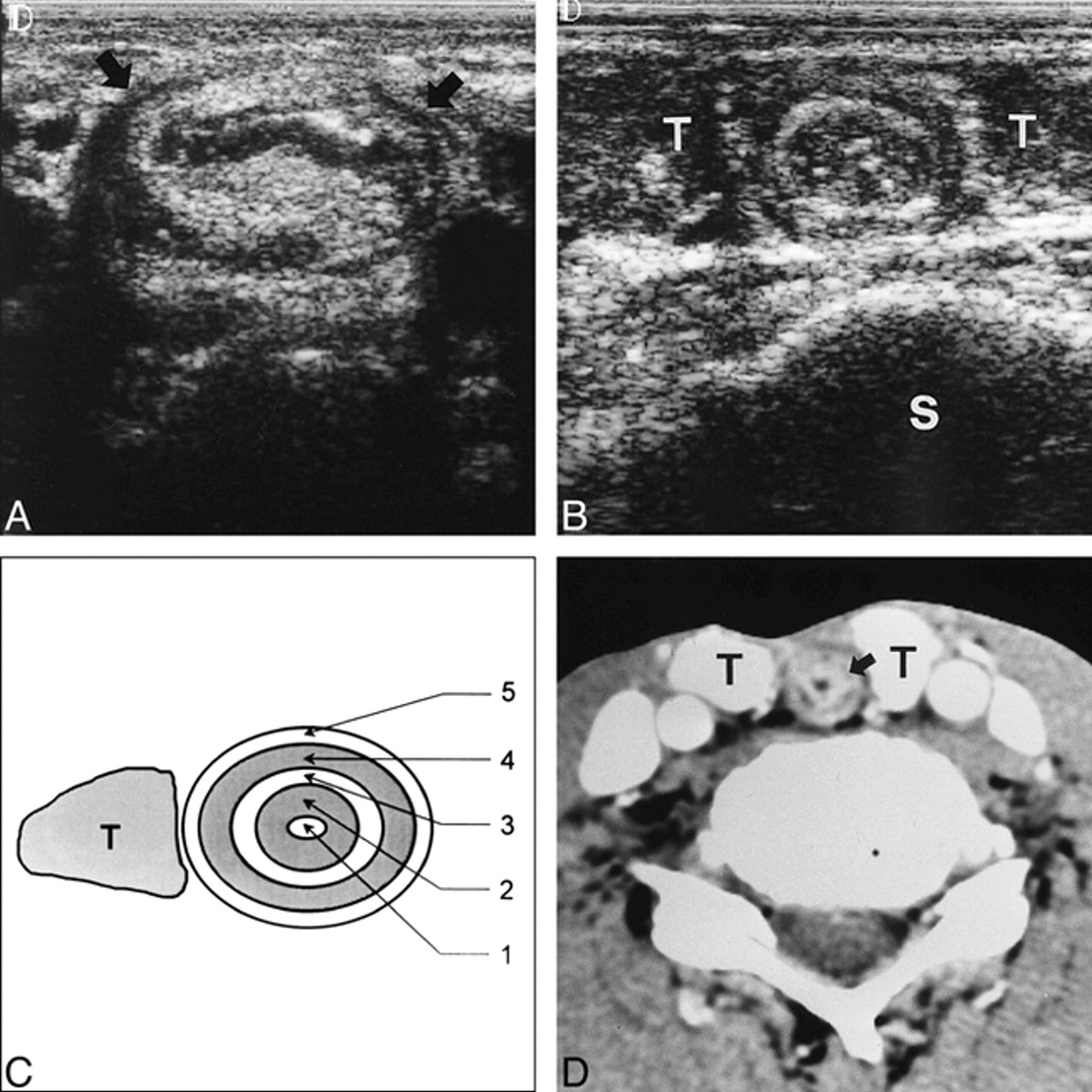
On sonograms, the neopharyngeal wall had five layers of alternating echogenicity (Fig 1A–C). Beginning with the inner wall, the first, third, and fifth layers were hyperechoic, whereas the second and fourth layers were hypoechoic. All five layers could be seen in 17 patients; the outermost layers were indistinct in eight patients.
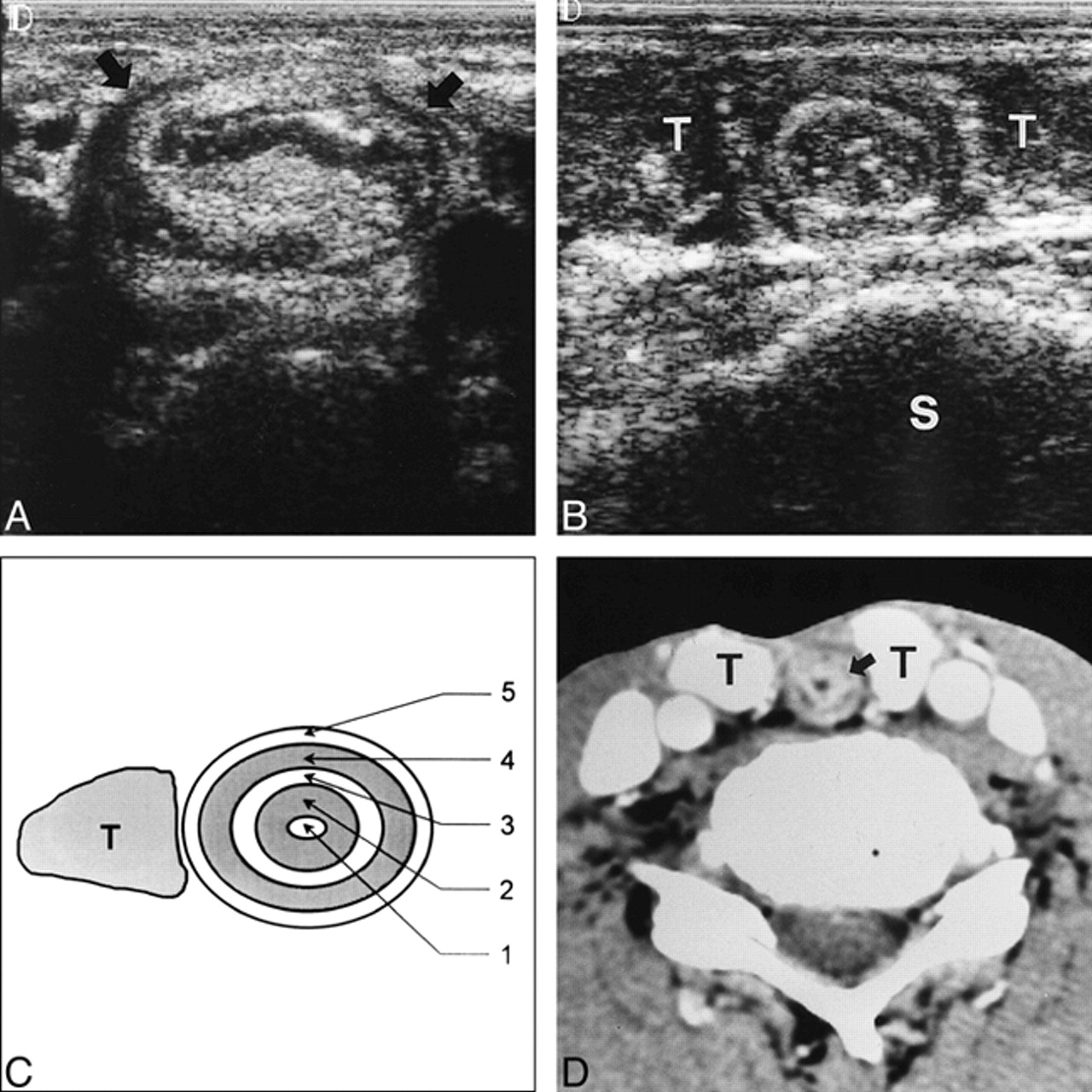
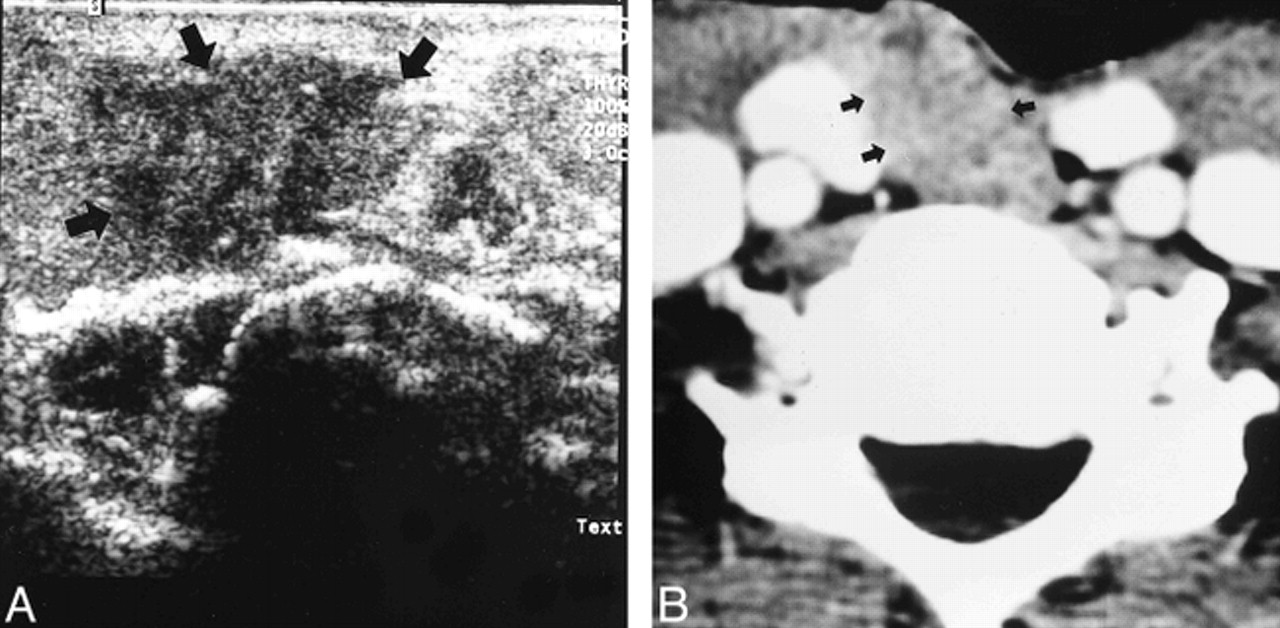
Normal neopharynx in a 64-year-old man who underwent total laryngectomy 5 years earlier.
A, Sonogram at mid-neck level shows the ovoid neopharynx (arrows) between the subcutaneous layer of the anterior part of the neck and the cervical spine.
B, Sonogram 3 to 4 cm caudal to the level of A shows five layers around the neopharynx with alternating echogenicity. S indicates cervical spine; T, thyroid gland.
C, Diagram of B. 1 indicates innermost layer of interface and superficial mucosa; 2, inner layer of deep mucosa; 3, middle layer of submucosa; 4, outer layer of pharyngeal constrictor muscles; 5, outermost layer of adventitia; T, thyroid gland. Shaded areas are hypoechoic.
D, Axial CT scan at the same level as B shows a three-layered, round neopharynx. The thin hypodense middle layer corresponds to the submucosa (arrow). T indicates thyroid gland.
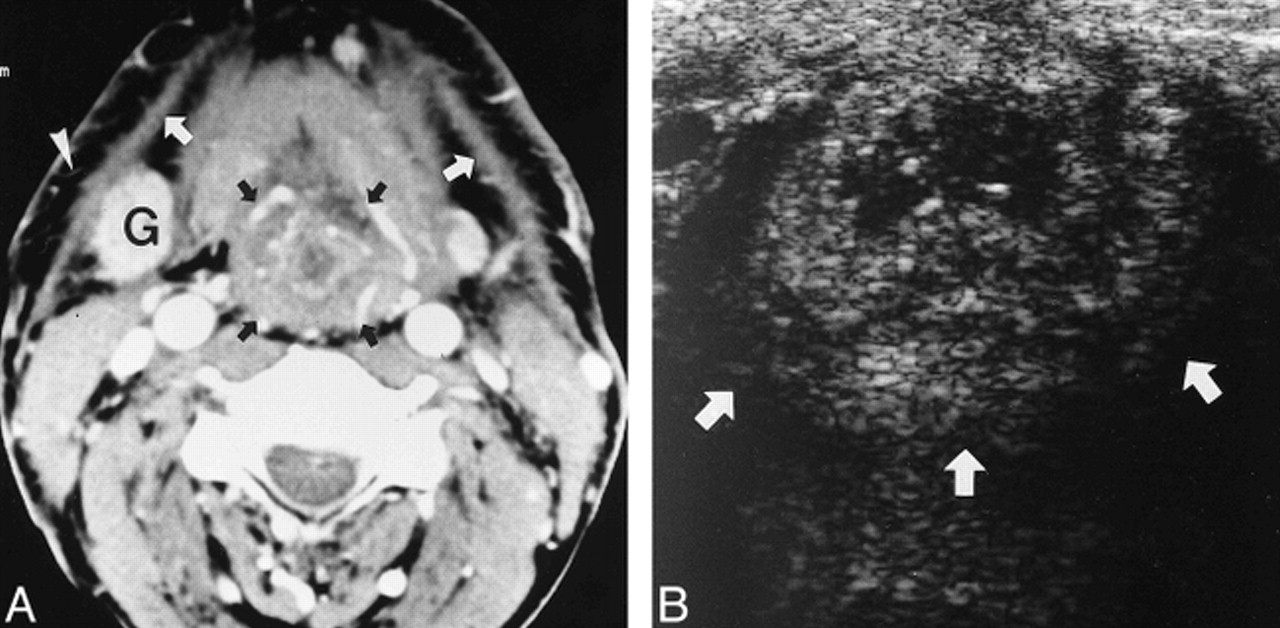
On CT scans, the neopharynx appeared as a three-layered structure (Fig 1D). The inner layer was iso- or hyperdense relative to muscle, depending on the degree of enhancement. The middle layer was hypodense and the outer layer isodense. In six patients, the middle layer could not be seen, and in four of them only a single-layered neopharynx was visible, owing to inadequate enhancement of the inner layer. In four of 11 patients who had undergone radiation therapy, radiation-induced changes of the neck were evident on CT scans, including platysmal thickening, reticulation of subcutaneous fat, and exaggerated enhancement of submandibular glands (Fig 2A). The mean interval between completion of radiation therapy and CT scanning for the patients was 8.5 months. These findings were indistinct on sonograms. The neopharynx also reflected radiation-induced changes on both sonograms and CT scans, including a diffusely thickened neopharyngeal wall and a globular shape of the neopharynx, even at the level of the tongue base (Fig 2).

Radiation-induced changes in a 54-year-old man who underwent radiation therapy 9 months earlier.
A, Axial CT scan shows diffusely thickened neopharynx (black arrows), platysmal thickening (white arrows), reticulation of the subcutaneous fat (arrowhead), and exaggerated enhancement of the submandibular gland (G), all consistent with benign radiation changes.
B, Sonogram at level of tongue base shows globular-shaped neopharynx (arrows).
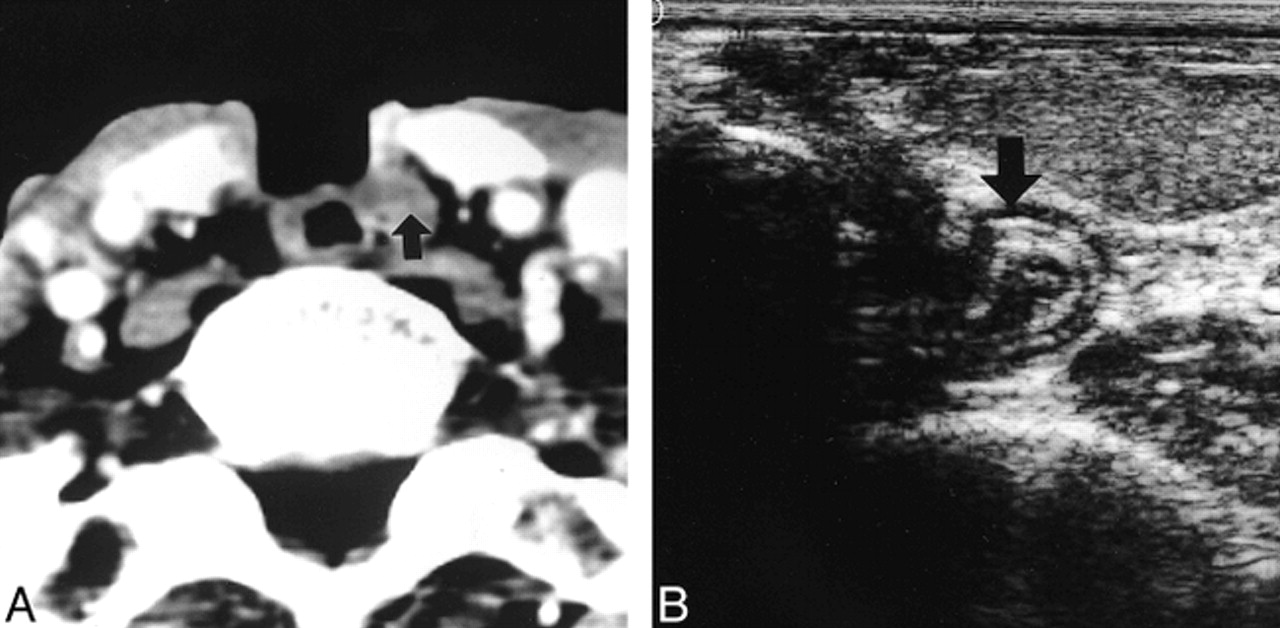
Nine patients (36%) were found to have recurrent tumor, all in stage IV. Four of nine recurrences were clinically occult. Sensitivity was 88.9% for sonography and 100% for CT; specificity was 100% and 93.8%, respectively. The interval between total laryngectomy and recurrence was 4 to 21 months (mean, 8 months). Locally recurrent masses (10–50 mm in size) were at the level of the tongue base (n = 2) and peristomal area (n = 2). Sonography showed hypoechoic homogeneous (n = 1) or heterogeneous (n = 3) masses abutting the neopharynx (Fig 3A). CT studies showed isodense (n = 3) or hypodense (n = 1) masses that were homogeneous in nature (Fig 3B). CT scans showed two of them as focal thickening of the neopharyngeal wall rather than as a mass; however, sonograms revealed discrete masses (Fig 4). One false-positive finding of local recurrence on CT appeared as a horseshoe-like folded neopharynx on axial plane sonography (Fig 5). There was no clinical evidence of recurrence. All patients with local recurrence underwent surgery, and squamous cell carcinomas were all confirmed pathologically.

Locally recurrent tumor in a 61-year-old man who underwent total laryngectomy 7 months earlier.
A, Sonogram at the level of the stoma shows poorly defined hypoechoic mass (arrows) on the right side of the neopharynx with obliteration of outermost layer.
B, CT scan shows a poorly defined, enhancing solid mass (arrows), which obliterates the fat plane between the mass and neopharynx. Recurrent squamous cell carcinoma was confirmed pathologically.

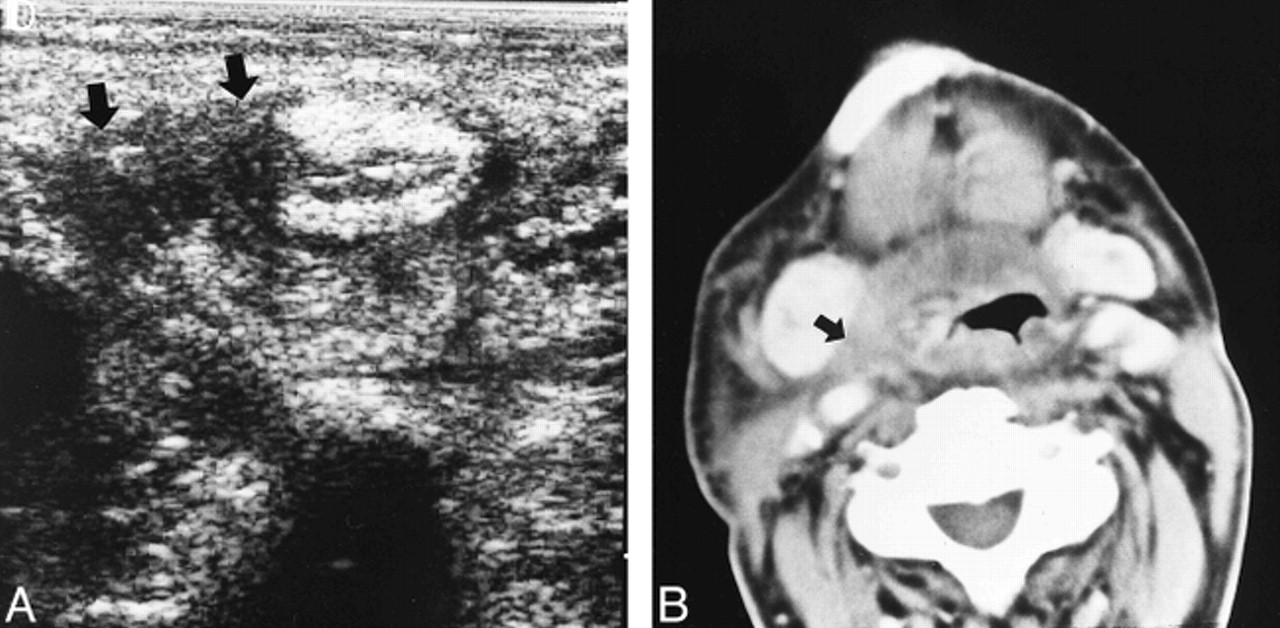
Locally recurrent tumor in a 44-year-old man who underwent total laryngectomy 14 months earlier.
A, Sonogram shows a poorly defined hypoechoic mass (arrows) on the right side of the neopharynx, which obliterates the outer three layers of the neopharynx.
B, CT scan shows a less discrete isodense mass (arrow) on right side of the neopharynx. Recurrent squamous cell carcinoma was confirmed pathologically.
False-positive CT finding in a 68-year-old man who underwent total laryngectomy 5 years earlier.
A, Axial CT scan shows a well-defined isodense mass abutting left side of neopharynx (arrow). Preservation of surrounding fat plane is notable.
B, On axial sonogram, the mass shows horseshoe-like folded neopharynx (arrow). There was no clinical evidence of recurrence. Note the even thickness of each of the neopharyngeal layers.
Metastatic lymph nodes (11–40 mm) were located in the internal jugular chains. It was impossible to count the exact number of nodes, because they were often conglomerated. All metastatic lymph nodes showed rim enhancement on CT scans and low echogenicity with lack of hilar fat on sonograms. Obliteration of the fat plane deep to the sternocleidomastoid muscle and concomitant infiltrative thickening of the muscle were present in three patients at both sonography and CT. One false-negative sonographic finding of nodal metastasis was seen in a jugulodigastric node. All nodal metastases were confirmed by fine-needle aspiration cytology. Four of these patients underwent neck dissection and the others were treated by chemotherapy. None of the patients had distant metastasis.
Discussion
CT has proved to be a valuable tool for both diagnostic and follow-up imaging in patients with laryngeal carcinomas (1–3, 9, 10). On the other hand, few reports have addressed the usefulness of sonography in patients with advanced laryngeal carcinoma, especially in the evaluation of extralaryngeal spread and detection of metastatic lymph nodes (11, 12). Our study evaluated the normal sonographic appearance of the neopharynx and assessed the accuracy of sonography as compared with CT in the detection of tumor recurrence in 25 patients who had undergone a total laryngectomy.
The normal sonographic appearance of the neopharynx is similar to findings at endoscopic sonography of the esophagus. Beginning at the inner wall, the endoscopic sonographic findings are as follows: an interface between the luminal surface and the superficial mucosa (hyperechoic); the deep mucosa, including the muscularis mucosae (hypoechoic); the submucosa and an interface with the muscularis propria (hyperechoic); the muscularis propria (hypoechoic); and an interface between the adventitia and the periadventitia (hyperechoic) (13). The mucosa and submucosa of the neopharynx are continuous with those of the esophagus, so the innermost hyperechoic layer, the inner hypoechoic layer, and the middle hyperechoic layer of the neopharynx correspond to the superficial mucosa, deep mucosa, and submucosa of the esophagus, respectively. The outer hypoechoic layer corresponds to the pharyngeal constrictor muscles, and the outermost hyperechoic layer corresponds to the adventitia and fatty tissue. The cervical esophagus of a healthy volunteer scanned with the same transducer appeared similar to the multilayered structure of the neopharynx. CT studies, however, showed the neopharyx as a three-layered structure: an inner enhancing layer, a middle hypodense layer, and an outer isodense layer, corresponding histologically to the mucosa, submucosa, and muscularis propria (pharyngeal constrictor muscle), respectively, of the stomach (14).
The mean interval between the completion of radiation therapy and CT scanning was 8.5 months (range, 5–13 months) for the patients in whom radiation changes were seen, and 50 months (range, 10–84 months) for the patients with no radiation changes. This result is similar to that reported by Mukherji et al (15). In the irradiated group, an indistinct, enhancing middle hypodense layer was thought to represent edema, thickening of connective tissue, and enhancement resulting from formation of telangiectatic vessels. In the nonirradiated group, these findings were thought to be the result of technical factors, including window selection or volume averaging of the relatively thin middle layer.
Lutz et al (16) reported that all recurrent supraglottic and glottic carcinomas occurred within the first 2½ years after laryngectomy. Large primary tumor size (≥1.5 cm) and stage N2 and N3 nodal disease were most frequently associated with regional recurrence (16, 17). Our data also support these results. Nine patients with recurrence had large primary tumors (2.7–5.5 cm) and eight had stage N2 nodes. The presence of a mass that effaces the fat plane around the neopharynx is a reliable sign of local recurrence on both sonograms and CT scans. A local recurrent mass seems to be more distinct on sonograms than on CT scans because of contrast between the mass and neopharynx. In our study, CT scans were obtained with a section thickness of 7 mm, which reduces the ability to detect subtle changes within lymph nodes as well as reduces the resolution of the scan with regard to the neopharynx. On review of the false-positive CT representation of local recurrence, a finding different from other true lesions was preservation of the fat planes surrounding the masslike lesion. Thus, obliteration of the fat plane around the mass can be added to the criteria of local recurrence.
Although sonography is operator-dependent, it is valuable in the routine follow-up of patients with total laryngectomy because of its easy accessibility and cost-effectiveness as well as its ability to delineate the normal neopharynx and recurrence. It is important to make an effort to evaluate neck nodes and the neopharynx sonographically, especially within 2 years after initial treatment. Further research with large series comparing sonography with CT or with MR imaging will be required to clarify the role of sonography.
Conclusion
This prospective study evaluated the sonographic findings in the normal neopharynx and in the neopharynx after tumor recurrence. The normal neopharynx has five ultrasonic layers of alternating echogenicity: an innermost hyperechoic layer, an inner hypoechoic layer, a middle hyperechoic layer, an outer hypoechoic layer, and an outermost hyperechoic layer. A locally recurrent lesion is usually seen as a hypoechoic mass that effaces the fat plane around the neopharynx. Sonography is valuable for the routine follow-up of patients who have had a total laryngectomy.
References
- Received October 14, 1999.
- Copyright © American Society of Neuroradiology
In this issue








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.