
Abstract
Summary: A case of primary malignant melanoma of the conus medullaris depicted at MR imaging is presented. Tumoral histoimmunologic analysis revealed features of malignant melanoma. Because findings for primary melanoma outside the spinal cord were negative, the diagnosis of primary intramedullary malignant melanoma was established. This rare tumor should be suspected when T1-weighted images show signal hyperintensity and T2-weighted images show signal iso- or hypointensity, with mild contrast enhancement of the lesion. However, these features may vary depending on intratumoral bleeding and melanin content.
Primary malignant melanoma in the CNS is unusual and accounts for approximately 1% of all melanoma cases. The occurance of this lesion in the spinal cord is extremely rare (1–5). The pigmented tumors may have varied appearance on MR image because of their different degrees of melanin or hemorrhagic foci. Thus, pathologic examination is critical for correct diagnosis.
Case Report
An 80-year-old woman with a history of back pain and slight weakness in the lower extremities was admitted. The symptoms had progressively worsened. A few days before admission, the back pain and bilateral leg weakness increased so that she was unable to walk, and she had recent urinary and anal incontinence.
Neurologic findings were consistent with compression of the lower spinal cord. Therefore, MR imaging was performed, and images revealed an intramedullary mass arising in the region of the conus medullaris at the level of the T12 through L1 vertebrae, which had a homogeneous appearance on all images. The cord was slightly swollen adjacent to the upper border of the mass. The tumor margins appeared distinct on all images. The lesion had slight signal hyperintensity on T1-weighted images (Fig 1) and was somewhat hypointense on T2-weighted images (Fig 2) relative to the signal intensity of the spinal cord. After intravenous injection of a gadolinium-based contrast agent, a moderate homogeneous enhancement of the entire lesion was noted (Figs 3 and 4).

Sagittal T1-weighted MR image shows the spinal cord tumor at the level of the conus medullaris, which has a slight and homogeneous signal hyperintensity relative to that of the cord.
fig 2. Sagittal T2-weighted MR image shows that the mass, compared with the spinal cord, is somewhat hypointense.
fig 3. Sagittal contrast-enhanced T1-weighted MR image shows mild homogeneous enhancement in the tumor
These findings were compatible with those of an intramedullary tumor, with the possibility of intratumoral bleeding or the presence of a pigmented tumor. Bone marrow alteration was present in the posterior aspect of the vertebral bodies of L1 and L2, which showed low signal intensity on T1-weighted images, high signal intensity on T2-weighted images, and slight enhancement after the injection of a gadolinium-based contrast agent (Figs 1–3). The rapid evolution of neurologic symptoms and the importance of the pain justified the intervention peformed in the lesion.
At surgery, a T11–L1 laminectomy was performed. After the dura was opened wide, the tumor was exposed. It was firm, deep black, and hypervascularized; it infiltrated the conus medullaris and invaded the nerve roots of the cauda equina. No clear limits of the tumor could be found in the spinal cord or on the nerve roots. Myelotomy was performed, several histologic samples were removed, and sonographic aspiration of the tumor was attempted. Unfortunately, diffuse tumoral infiltration of both conus medullaris and cauda equina did not allow aggressive removal of all the melanocytic tissue. Although the resection was subtotal, it allowed some decompression of the neurologic structures.
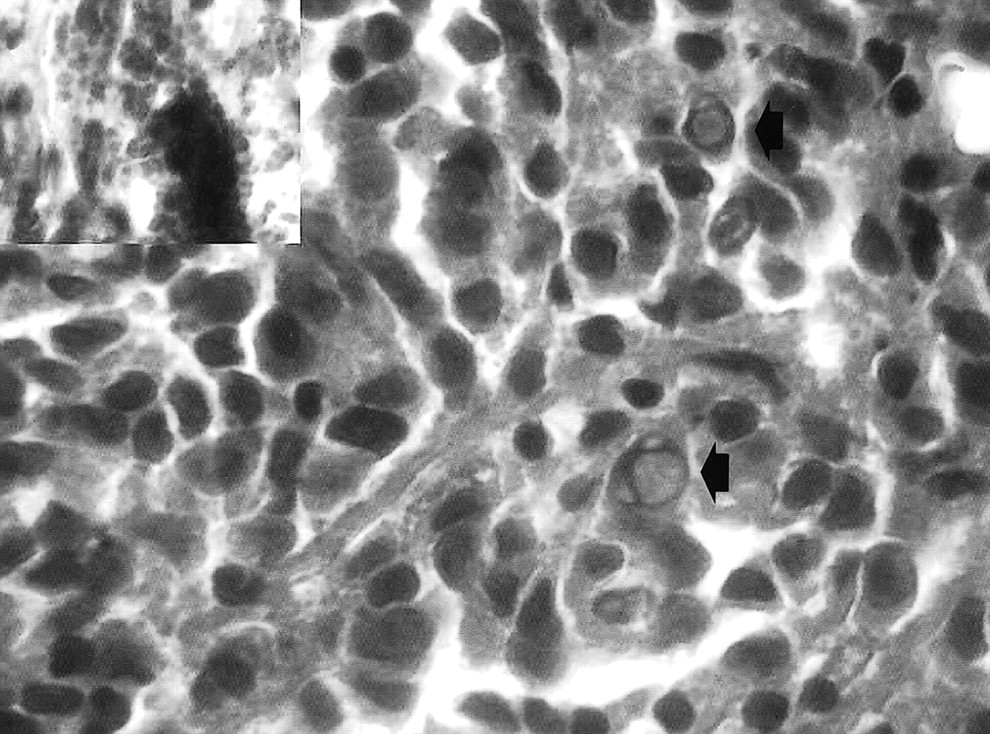
The macroscopic aspect of the lesion was that of a malignant pigmented tumor. Histologic analysis revealed a highly cellular tumor, which was depicted as a clustering growth pattern that diffusely invaded the spinal cord (Fig 5). The tumor was composed of large epitheloid or spindle cells that frequently had intranuclear vacuoles (Fig 6). These particular cellular patterns, enriched with golden-brown granular cytoplasmic pigmentation (Fig 6), were highly suggestive of malignant melanoma. Strong immunohistochemical reactions for S100 protein and HMB45 confirmed the diagnosis.

Axial T1-weighted images demonstrate the intramedullary position of the tumor, which occupies nearly the entire spinal canal.
A, Nonenhanced image.
B, Gadolinium-enhanced image shows mild homogeneous enhancement in the lesion

Low-magnification photomicrograph shows that the tumor is highly cellular. Nuclear anaplasia has a tendency to form clusters of cells resembling the structure of a nevus (hematoxylin-eosin, magnification × 250). The inset shows the tumor invading the nervous structures (stars)

Photomicrograph shows that some nuclei of the epitheloid malignant cells contain nuclear inclusions (arrows) (hematoxylin-eosin, magnification × 1000). The inset shows that a large amount of melanin pigment masks the spindle-shaped malignant cells
After surgery, the patient underwent other radiologic studies of the head and body, as well as dermatologic and ophthalmologic examination, which did not reveal any other foci of melanoma. With these data, the diagnosis of primary intramedullary malignant melanoma was established. The postoperative course was followed with a progressive resolution of back pain, but no improvement in the patient's neurologic status occured. Because of the patient's age and poor prognosis, it was decided, with the family's consent, to transfer the patient to a rehabilitation center. The patient did not receive adjuvant radiation therapy. At the time this article was written, about 9 mo after surgery, the patient is still alive and is receiving clinical follow-up.
Discussion
Primary pigmented tumors of the CNS are unusual; they include melanotic schwannoma, meningeal melanocytoma, blue nevus of the CNS, and primary melanoma (3–6). Among these lesions, primary malignant melanoma of CNS is rare and accounts for about 1% of all melanomas. Primary malignant melanoma of the spinal cord is a very rare entity, occuring most often in the middle or lower thoracic cord (1–8). Among the 27 cases of CNS malignant melanoma that Hayward (1) reported, only four lesions were in the spinal cord. Hirschberg (9) first reported primary spinal cord melanoma in 1906. Since then, a few cases have been reported in the literature; these involve intra- or extramedullary, leptomeningeal, and extradural lesions (1–3, 5, 7, 8).
A malignant melanoma can occur in any organ in which melanin-containing cells are present. Two theories have been proposed for the origin of the rare cases of CNS melanoma. Primary melanoma in the CNS may originate from melanoblasts accompanying the pial sheaths of vascular bundles or from neuroectodermal rest cells during embryogenesis (1, 2, 6, 8). According to the Hayward classification (1), the diagnosis of primary spinal cord melanoma is based on an absence of melanoma outside of the CNS, an absence of this lesion in other sites in the CNS, and histologic confirmation of melanoma. According to these classification criteria, our case was thought to involve a primary malignant melanoma of the spinal cord. This lesion occurs most often in middle age and can affect both sexes equally. The presenting symptoms of this lesion are predominantly those of spinal cord compression (2–4).
At present, MR imaging is the method of choice in the diagnosis of spinal cord tumors, but the distinction of the kinds of tumors based on their morphologic or signal intensity characteristics at MR imaging remains difficult (3, 10). This technique may be used to demonstrate the varied appearance of spinal cord melanoma. Moreover, the MR imaging pattern may correspond to that of other pigmented tumors, such as meningeal melanoma, melanotic schwannoma, or a tumoral hemorrhagic lesion (3, 11, 12). Spinal cord melanoma usually shows slightly increased signal intensity on T1-weighted images relative to that of the spinal cord. On T2-weighted images, it can demonstrate the same or low signal intensity compared with that of the normal cord. After the intravenous administration of a gadolinium-based contrast agent, the lesion most often shows mild and homogeneous enhancement (3, 5, 8, 13, 14). In our case, the appearance of the lesion on MR images was in accordance with the reported findings in the literature.
Generally, hyperintensity on T1-weighted images may be due to the presence of melanin, as well as hemorrhage or fat (3, 4, 13). The signal intensity features of melanoma on T1- and T2-weighted images are thought to be caused by the paramagnetic stable free radicals that exist within melanin or the paramagnetic products of hemorrhage (5, 11, 12, 14). Foci of hemorrhage also may occur in malignant melanoma and can modify the signal intensity features on MR images. Moreover, a subacute or chronic hemorrhage in the tumor may influence the the MR imaging pattern to a greater extent than does melanin, resulting in variable signal intensity in the tumor (5, 10–12, 15).
Melanoma does not always have a homogeneous pattern on MR images; its appearance may depend on the degree of melanin or previous hemorrhage within the lesion. The distinction between melanin and methemoglobin based on MR images is difficult, because both have similar relaxation characteristics (8, 11, 15). Foci of hemorrhage may occur not only in melanoma but also in other malignant tumors of the spinal cord; thus, the differentiation of such a tumor from other types of intramedullary malignant lesions is difficult, and the MR pattern easily can suggest an erroneous diagnosis (5, 10, 12).
The MR imaging appearance of intramedullary metastatic melanoma also may be similar to that of a primary tumor; therefore, careful examination of skin, squamous mucosa, and eyes must always be performed to exclude a primary melanoma in these sites (4, 10).
The treatment of intramedullary malignant melanoma is difficult. The best treatment may be a total surgical excision of the lesion, whenever possible, but removal of the tumor generally is incomplete, and radiation therapy often is recommended after surgery (2–5, 10). Chemotherapy is another complementary treatment that may be used after surgery and postoperative radiation therapy (3, 5).
In conclusion, awareness of the unusual presence of melanoma within the spinal cord is important, and the possible presence of this lesion must be considered when MR images depict a spinal cord tumor with paramagnetic properties. The final diagnosis, however, is based on the results of pathologic examination.
Footnotes
1 Address reprint requests to Dordaneh Farrokh, Avenue de Broqueville, 157/1, 1200 Bruxelles, Belgium.
References
- Received March 28, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}