
Abstract
Summary: Bilateral mesiotemporal hyperintensity on T2-weighted and fluid-attenuated inversion recovery MR images of a patient with a clinical syndrome of encephalitis is considered to be a classic finding for herpes simplex virus infection. We report a case of neurosyphilis with identical MR imaging abnormalities and a similar clinical presentation. Because syphilis is not routinely tested for, awareness of this mimicry of herpes simplex virus encephalitis is important, considering the potential therapeutic implications.
During the last few decades, especially during the era of AIDS, there has been a significant rise in the number of cases of syphilis and a concomitant increase in the incidence of neurosyphilis (1). One third of patients who progress to tertiary syphilis develop neurosyphilis (2, 3). Because the disease is treatable with antibiotics, early diagnosis and treatment is critical. Making the diagnosis is often difficult, however, because most patients either are asymptomatic or present with nonspecific symptoms, such as headache, seizures, insomnia, personality change, decreased memory, irritability, emotional lability, visual complaints, and confusion (2, 4). Furthermore, the classic descriptions of neurosyphilis from the preantibiotic era, such as general paresis of the insane and tabetic neurosyphilis are now only rarely encountered (1, 4).
Another difficulty is the wide variety of CNS manifestations of neurosyphilis, both clinically and on neuroimages. The range includes normal results of MR imaging, CT, and angiographic studies, mild to moderate atrophy, cortical and subcortical infarction, white matter lesions, gummata, leptomeningeal enhancement, and arteritis (1, 2, 5).
We present a case to further expand the radiologic spectrum of neurosyphilis. To our knowledge, this represents the third report (6, 7) and the first in the radiology literature of neurosyphilis mimicking the neuroimaging characteristics of herpes encephalitis.
Case Report
A 50-year-old homeless man was brought to the hospital with a 3-month history of increasing memory difficulties and of recurrent 1- to 2-hour episodes of disorientation with increasing frequency. An examination revealed that he was afebrile and alert with a Mini-Mental State Examination score of 25/30 due to deficits in memory, writing, and calculation. The results of general physical and neurologic examinations were otherwise unremarkable. Soon after admission, the patient had a single witnessed generalized tonic-clonic seizure. Lumbar puncture revealed 19 WBC/μL, 93% of which were lymphocytes, hypoglycoracchia (45 mg/dL), and an elevated CSF protein count (87 mg/dL). EEG showed focal slowing over the left frontotemporal regions. There was subtle bilateral inferotemporal lobe hypermetabolism on interictal positron emission tomographic scanning. MR imaging of the brain revealed prominent cortical and subcortical confluent increased fluid-attenuated inversion recovery (FLAIR) and T2 signal in the right mesial temporal region, with mild bilateral temporal lobe atrophy and enlargement of the lateral ventricular temporal horns, more discernible on the left (Fig 1). There was also some subtle FLAIR and T2 hyperintensity in the left mesial temporal lobe. There was associated subtle T1 hypointensity, without evidence of petechial hemorrhage or mass effect. No contrast medium was administered for the initial MR imaging.
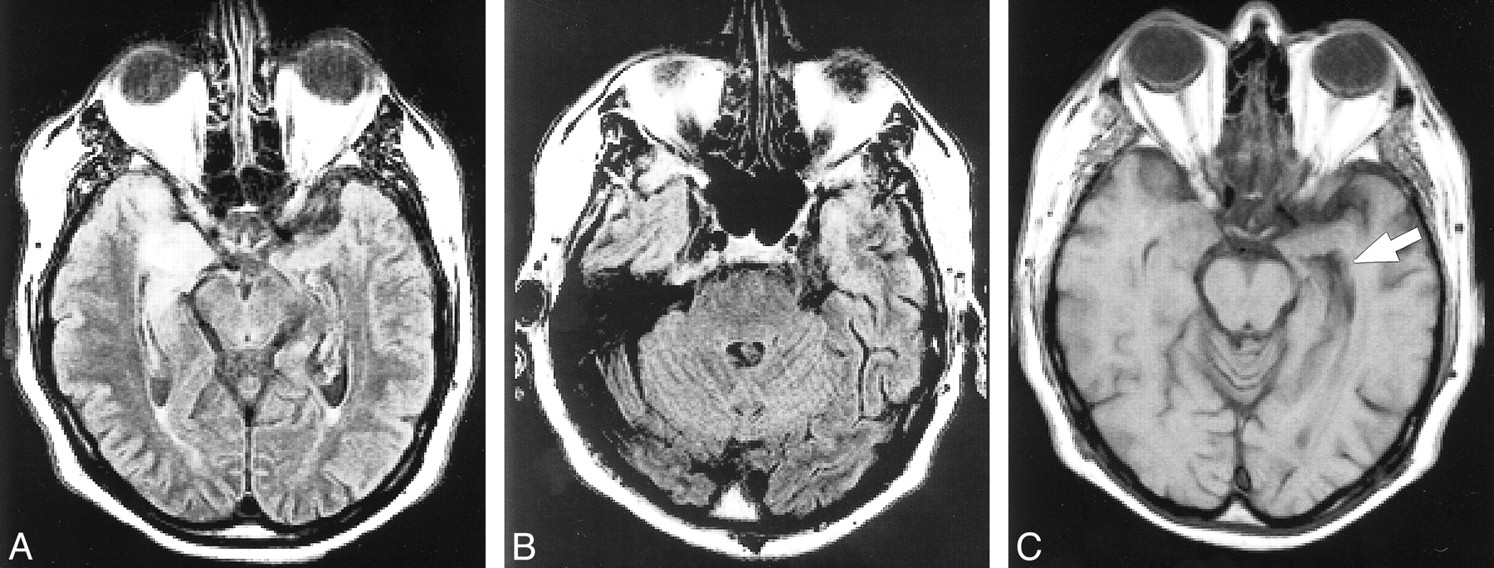
Images of a 50-year-old man with a 3-month history of progressive dementia, who presented with seizures. Serologic evidence of active neurosyphilis was present, and there was no evidence of herpes virus infection.
A, Axial FLAIR image obtained at midbrain level.
B, Axial FLAIR image obtained at the level of the pons. Asymmetrical bilateral signal hyperintensity in the mesial temporal lobes can be seen and is greater on the right side than on the left.
C, Axial T1-weighted image obtained at the level of the low midbrain. This image shows mild left temporal lobe atrophy, evidenced by dilation of the temporal horn (arrow).
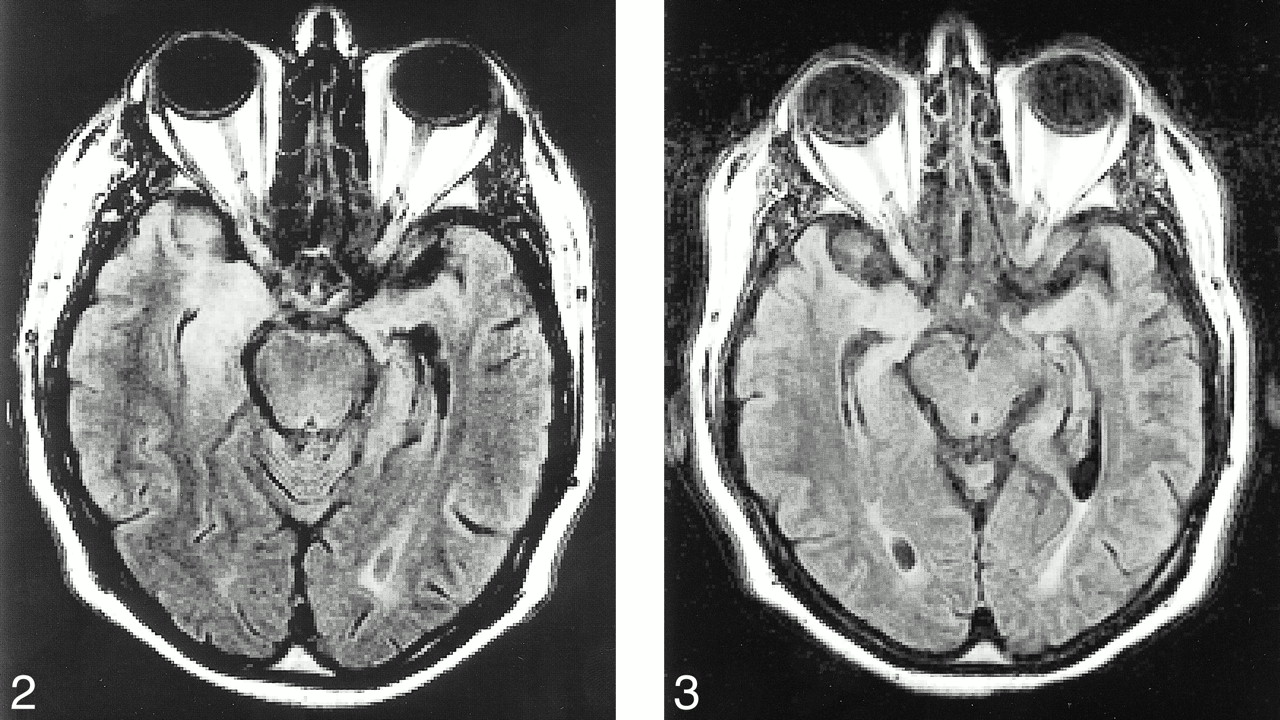
The patient was treated empirically for herpes encephalitis with acyclovir. However, when the results of CSF polymerase chain reaction for herpes simplex virus 1 and 2 DNA were found to be negative, an alternative diagnosis was sought. The CSF bacterial and fungal cultures and skin purified protein derivative of tuberculin remained negative. The results of the serum rapid plasma reagent test (titer, 1:64) and microhemagglutination-Treponema pallidum test (4+) were subsequently found to be positive, as were the results of the CSF Venereal Disease Research Laboratory test (titer 1:16) and the fluorescent treponemal antibody-absorption test. The patient received a 14-day course of penicillin, and at discharge 15 days later, there was minor cognitive improvement but essentially no imaging differences on the MR images (Fig 2). There was no evidence of mesial temporal enhancement revealed by the repeat study.

Axial FLAIR image of the same patient, obtained 10 days after treatment with penicillin. There are essentially no imaging differences as compared with the pretreatment images. fig 3. Axial FLAIR image of the same patient, obtained 4 months after treatment with penicillin. There is significant interval improvement in the previously noted mesial temporal signal abnormalities. There is also slight right temporal atrophy, with compensatory dilation of the temporal horn
Four months later, the patient returned for longer term follow-up and was found to have both significant cognitive and radiographic improvement. The patient was fluent, with completely intact immediate recall and only mild deficits in long-term recall. MR imaging indicated significant improvement as compared with the previously noted mesial temporal FLAIR and T2 hyperintensity (Fig 3).
Discussion
Bilateral mesiotemporal T2 hyperintensity on MR images, usually somewhat asymmetrical, is an imaging finding referred to as “virtually pathognomonic” for herpes encephalitis. It is thought to be secondary to intracranial spread of the herpes virus along the small meningeal branches of the trigeminal nerve from the trigeminal ganglion (8, 9). A few other uncommon to rare entities have been reported with similar imaging manifestations. They include paraneoplastic limbic encephalopathy, lupus erythematosus, Hurst hemorrhagic leukoencephalitis, and gliomatosis cerebri (9–12).
Because neurosyphilis most commonly takes the meningeal or vascular form, and these often occur together, the imaging findings of meningovascular syphilis have been well characterized (1, 2, 5). These findings include both cortical and subcortical infarcts, (which have been reported in nearly 25% of patients with neurosyphilis) (1), leptomeningeal enhancement associated with a clinical meningitis (1, 2), and arteritis. The arteritis is of two forms; Heubner arteritis, which is the more common form, affects the medium and large arteries, and the Nissl-Alzheimer form of arteritis, which affects the small arteries and arterioles (1, 2). Other manifestations of meningovascular syphilis include leptomeningeal granulomas, known as gummata (2). Rarely, cerebral gummata have also been reported (1). Meningoneuritis, with cranial neuropathies, most often involving the VIIth and VIIIth cranial nerves, has also been reported (2). Other intracranial manifestations include orbital gummatous periostitis and periostitis involving the otic capsule (2). Other nonspecific manifestations include atrophy and white matter lesions (1).
Within this broad array of imaging findings, mesial temporal involvement has, to our knowledge, been reported as occurring in only two patients previously (6, 7). The more recent report, by Denays et al (6), was of a 51-year-old woman who presented with acute disorientation and amnesia and who had bilateral asymmetrical mesiotemporal T2 hyperintense lesions on MR images of the brain. The results of CSF polymerase chain reaction for herpes simplex virus 1 and 2 were negative, but the results of the microhemagglutination-Treponema pallidum test and the fluorescent treponemal antibody absorption test were strongly positive (6). Penicillin therapy resulted in marked improvement in memory and in the lesions revealed by MR imaging.
The cause of the mesial temporal T2-weighted hyperintensity is unclear. However, considering that the most prevalent form of neurosyphilis is marked by meningovascular involvement, it is suggested that the signal changes represent a combination of edema and gliosis. The edema component itself most likely has multiple causes. With meningitis, there are changes in the meningeal and cerebral capillaries, with a possible increase in the permeability of the blood-brain barrier, leading to a component of vasogenic edema (13). There may also be some cytotoxic edema, both from the effect of the meningeal inflammatory reaction and from parenchymal hypoxia due to involvement of small vessels (13). Finally, there may be an interstitial edema component due to focal obstruction of the arachnoid villi from fibrin deposits and leukocytes (13). The presence of an edema component is further suggested by the imaging improvement noted after antibiotic therapy. The presence of gliosis may be present secondary to infection-induced small-vessel ischemic changes.
This unusual constellation of findings and the striking similarity in both clinical presentation and imaging findings between our case and the other two reported cases suggest the necessity of adding neurosyphilis to the short list of herpes mimicries. This is especially important considering that the clinical presentation of neurosyphilis may also seemingly mimic that of herpes encephalitis, albeit an unusual presentation (4).
The current case and the case reported by Denays et al (6) included a suggestion of some subtle temporal atrophy with slight enlargement of the temporal horns, rather than the mild mass effect that accompanies the profound cortical and subcortical edema in acute herpes simplex virus infection. This is perhaps expected, because the course of neurosyphilis is more indolent than the fulminant course of herpes encephalitis and atrophy on imaging has been reported in 37% of neurosyphilis cases (1). This distinction may be of help in suggesting neurosyphilis as a diagnostic possibility.
This report, in addition to those presented by Denays et al (6) and Angus et al (7), serves to establish the potential similarity in the imaging findings of neurosyphilis and herpes simplex encephalitis. Syphilis serology is not routinely tested and may escape detection unless suspicion of the disorder is raised by the radiologist.
Footnotes
↵1 Address reprint requests to Gasser M. Hathout, MD, Associate Professor, Division of Neuroradiology, University of California Los Angeles, Department of Radiology, UCLA CHS B2-220, 10833 Le Conte Avenue, Los Angeles, CA 90095.
References
- Received May 24, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Susceptibility-weighted imaging in parenchymal neurosyphilis: identification of a new MRI finding
- Mystery Case: A 64-year-old woman with subacute encephalopathy
- Clinical Reasoning: The "Great Imitator"
- Pearls & Oy-sters: Neurosyphilis presenting as mesial temporal encephalitis
- Perils of the prozone reaction: Neurosyphilis presenting as an RPR-negative subacute dementia
- Neurosyphilis with complex partial status epilepticus and mesiotemporal MRI abnormalities mimicking herpes simplex encephalitis