
Abstract
Summary: We report a case of sinonasal sarcoidosis with perineural spread along the trigeminal and vidian nerves in which primarily MR imaging but also CT allowed excellent visualization of this infiltration.
Sarcoidosis is an idiopathic multisystemic granulomatous disease characterized by the association of clinical signs with histopathologic evidence of noncaseating granulomas (1). While sarcoidosis is mainly a pneumologic disease, extrapulmonary locations (eg, peripheral lymph nodes, skin, liver, eye, spleen, brain, bones) are also seen, though less frequently (1). Severe sinonasal involvement occurs in 12% to 27% of patients, whereas CNS involvement occurs in only about 5% of patients (2–7).
We describe the CT and MR imaging findings of a patient with sinonasal sarcoidosis that spread in a retrograde fashion along the trigeminal and vidian nerves. To our knowledge, no previous report has documented the spread of sinonasal sarcoidosis or involvement of the vidian nerve.
Case Report
A 48 year-old man had undergone surgery for sinonasal polyposis associated with a frontal mucocele. Six months later he presented with deep facial pain, nasal obstruction, anosmia, and rhinorrhea.
CT scans showed postsurgical changes and abnormal soft tissue in the maxillary sinuses, in the residual ethmoidal cavities, in the sphenoidal sinus, and in the pterygopalatine fossae bilaterally. Coronal scans showed enlargement of the left pterygoid canal and foramen rotundum, while the infraorbital canals appeared enlarged bilaterally (Fig 1A–C).

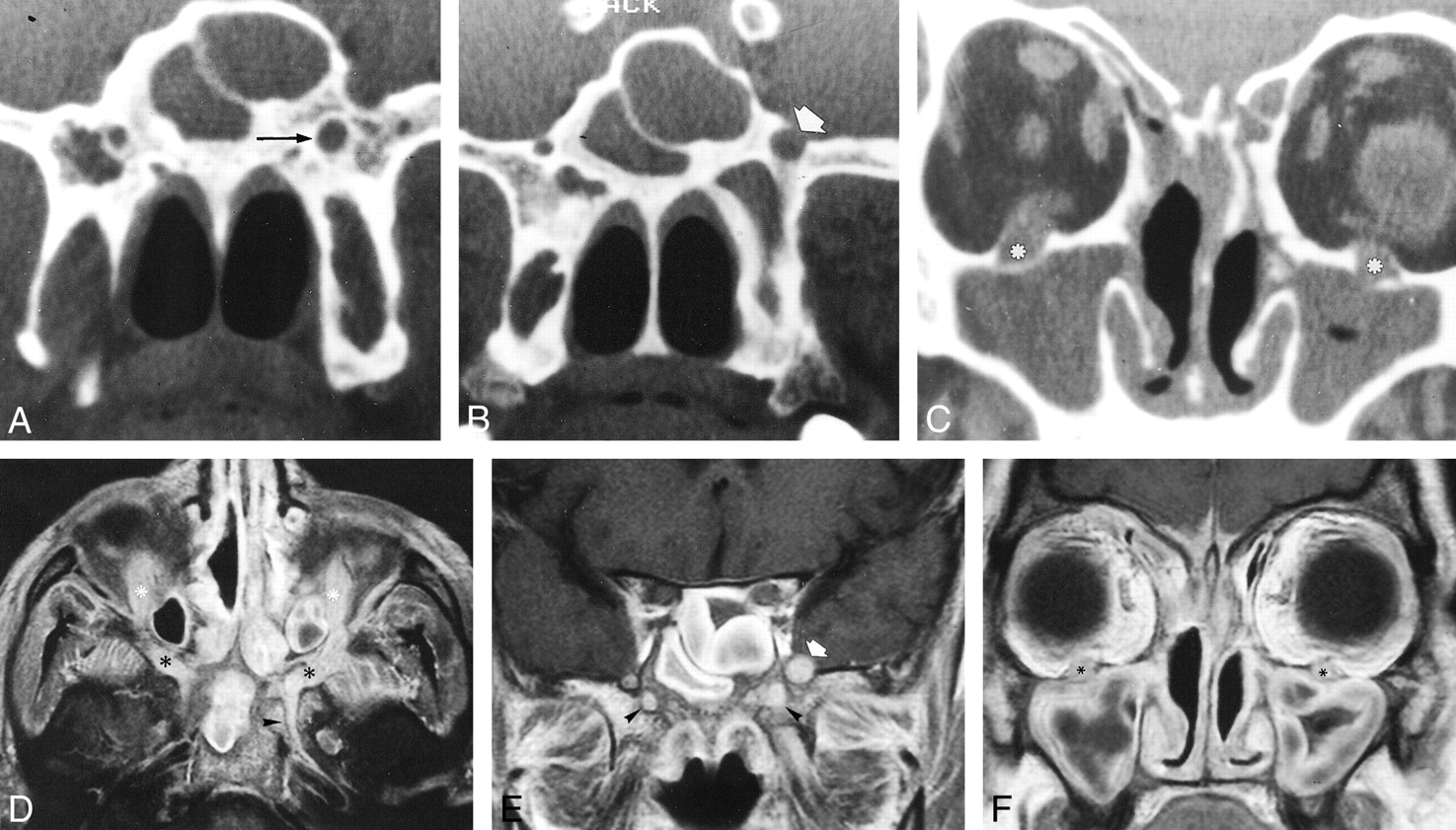
48-year-old man with deep facial pain, nasal obstruction, anosmia, and rhinorrhea 6 months after surgery for sinonasal polyposis associated with a frontal mucocele.
A–B, Coronal CT scans through the pterygoid process show enlargement of the left pterygoid canal (arrow, A) as well as enlargement of the left foramen rotundum (arrow, B).
C, Coronal CT scan more anterior than A and B shows widening and erosion of both infraorbital canals (asterisks). Note the presence of abnormal soft tissue in the maxillary and sphenoidal sinuses.
D, Contrast-enhanced axial T1-weighted MR image (700/12/6 [TR/TE/excitations]) through the base of the skull, obtained with a fat-saturation technique, shows abnormal enhancing tissue in the right and left upper pterygopalatine fossae (black asterisks). Enlargement and enhancement of the infraorbital nerves (white asterisks) and the left pterygoid nerve (arrowhead) can also be seen.
E, Contrast-enhanced coronal T1-weighted MR image (700/12/6) shows enhancement of the right and left vidian nerves (arrowheads), enlargement of the left vidian nerve, and left-sided maxillary division of the trigeminal nerve (arrow).
F, Contrast-enhanced coronal T1-weighted MR image (700/12/6) through the anterior part of the maxillary sinus shows enlargement and enhancement of both infraorbital nerves (asterisks). Abnormal enhancing tissue infiltrates through the skull base, involving the meninges in the anterior cranial fossa. Thickening of the sinus mucosa is visible on all images.
MR images obtained before and after intravenous administration of contrast material showed diffuse thickening and enhancement of the mucosa in the nasal cavities and in the maxillary, ethmoidal, and sphenoidal sinuses as well as abnormal tissue in the pterygopalatine fossa (Fig 1D–F). The residual lumen of the maxillary and sphenoidal sinus was filled with fluid. Abnormal tissue was spread along the infraorbital nerves, which were enlarged. On the left, perineural infiltration involved the pterygopalatine fossa, vidian nerve, and maxillary nerve, up to the gasserian ganglion. On the right, the pterygopalatine fossa and, to a lesser extent than on the left, the vidian nerve appeared involved, but not the maxillary nerve. Abnormal tissue infiltrated through the skull base, with involvement of the dura in the anterior cranial fossa (Fig 1F).
A biopsy sample of the nasal mucosa revealed multiple noncaseating granulomas, indicative of sarcoidosis. An increase in the erythrosedimentation rate and serum angiotensin-converting enzyme, together with radiographic findings of hilar adenopathy, confirmed the diagnosis of sarcoidosis.
Discussion
Sarcoidosis is an idiopathic, systemic, granulomatous disease whose onset is usually unifocal, but with a strong predilection for systemic involvement, characterized by alternating periods of remission and relapse (1). Sinonasal involvement is a relatively rare occurrence, with a frequency of 12% to 27% (3).
Several other diseases involving the sinonasal region are characterized by granulomatous lesions. Thus, the diagnosis of sinonasal sarcoidosis is often difficult, and is made by correlating clinical, radiologic, histologic, and laboratory findings (8, 9). Although cranial nerve involvement occurs frequently in neurosarcoidosis, the trigeminal nerve is rarely involved, and, to our knowledge, no report has documented involvement of the vidian nerve or perineural infiltration secondary to sinonasal sarcoidosis.
In our case, sarcoidosis had spread in a perineural fashion along the infraorbital and vidian nerves bilaterally as well as along the right maxillary nerve. This process resulted in enlargement of the bony canals and erosion of the cortical wall (10). MR imaging showed enhancement and enlargement of the involved nerves, providing direct evidence of neural spread and representing an advantage over CT in that it allowed complete evaluation of the stage of illness (10–12). It is important to remember, however, that the findings described are not specific, as they may also be seen in perineural spread of neoplasm (10–16).
Conclusion
The findings in our case enabled us to reach the following conclusions. 1) Perineural spread is a possible complication of sinonasal sarcoidosis; in fact, in our case, the process began presumably in the paranasal sinuses and spread upward along the cranial nerves, as suggested by the absence of neural involvement on the presurgical imaging studies. This is in accordance with the higher prevalence of sinonasal sarcoidosis as compared with CNS involvement (2–7). 2) MR imaging, but also CT, allows excellent visualization of this process. 3) Perineural spread of sarcoidosis along the trigeminal and vidian nerves may simulate perineural involvement by head and neck cancer, in particular when sarcoidosis is not confirmed by histologic studies.
Footnotes
1 Address reprint requests to Silvio Mazziotti, MD, Via Consolare Pompea, 45 (ex 23), 98168 Messina, Italy.
References
- Received October 26, 2000.
- Accepted after revision February 6, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.