
Abstract
Summary: The case of a 61-year-old woman who presented with herpes labialis, subclinical meningitis, and sudden onset of bilateral sensorineural hearing loss is presented. Contrast-enhanced MR imaging showed marked bilateral enhancement of the intracanalicular portion of the eighth cranial nerve, right cochlea, and left vestibule. Polymerase chain reaction was positive for human herpesvirus 1 obtained from the cerebral spinal fluid, which suggested the diagnosis of viral neuritis.
Sudden sensorineural hearing loss (SSHL) presents a difficult clinical and diagnostic problem. Most cases are idiopathic; however, there is increasing evidence for the role of viral infections in the pathogenesis of this condition. Varicella-zoster virus, a member of the family of herpesviruses and which causes the Ramsay Hunt syndrome, is one example.
Human herpesvirus 1 (HHV-1) infection, although rare, has been associated with SSHL. Latent HHV-1 has been found in human geniculate and vestibular ganglia (1). We present a case of bilateral enhancement of the eighth cranial nerve and labyrinth in SSHL associated with HHV-1.
Case Report
A 61-year-old woman transferred from another hospital 7 days after the onset of sudden deafness. Her medical history was unremarkable. The patient was admitted to another institution with pyelonephritis complicated by non–Q-wave myocardial infarction. She was treated with levofloxacine and did not receive aminoglycosides or any other potentially ototoxic drugs. Two days later, vesicular lesions developed around her lips. The patient denied having a history of herpes labialis. Punch biopsy of the lesions yielded HHV-1. At approximately the same time, the patient noticed sudden onset of hearing loss that rapidly worsened over the next 2 days to the point of total deafness.
Upon admission to our institution, the patient reported mild pain and pressure in her ears and denied experiencing vertigo or tinnitus. Physical examination demonstrated mostly crusted perioral lesions. There were no vesicles in the external auditory canals, and the tympanic membranes were normal. With the exception of the hearing loss, a slight gait imbalance, and positive Rhomberg test findings, her neurologic examination was unremarkable. Of interest is that there was no facial nerve deficit. Audiometric tests demonstrated no measurable hearing bilaterally. Cerebrospinal fluid analysis performed 9 days after the onset of deafness showed a white blood cell count of 95 cells/ mm3, a protein concentration of 149 mg/dL, and normal glucose levels. Polymerase chain reaction was positive for HHV-1 in the cerebrospinal fluid. Serologic measurements in the acute phase demonstrated no marked elevation of immunoglobulin (Ig) M against HHV-1 with an IgG level of 4.46 mg/dL (normal range, 0–0.79 mg/dL), while convalescent serologic measurements 6 weeks later showed an IgG level of 3.28 mg/dL. The serologic findings were consistent with reactivation of HHV-1 infection rather than primary infection, even though the patient denied having such a history.
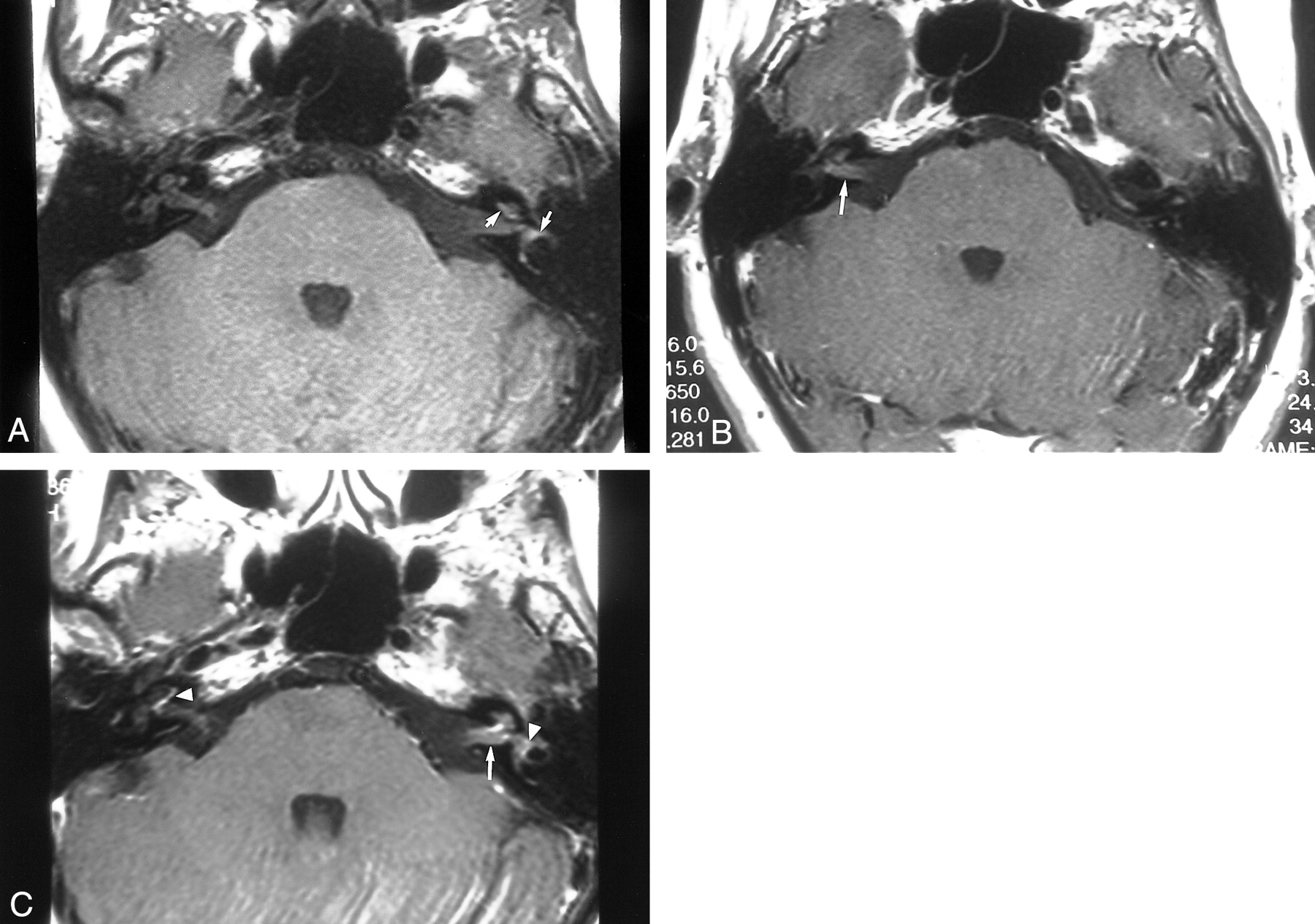
An MR study was performed with a 1.5-T MR unit (Eclipse; Picker, Highland Heights, OH). Fast spin-echo T2-weighted axial and fluid-attenuated inversion recovery axial images through the brain were obtained followed by 3-mm thick, pre– and post–gadopentetate dimeglumine T1-weighted axial and coronal images through the temporal bones. A xial images through the temporal bones also were obtained (Express; Picker). The examination demonstrated marked enhancement of the intracanalicular portion of the eighth cranial nerve. Also demonstrated was enhancement of the labyrinth involving the basal turn of the cochlea on the right and left vestibule. In addition, there was hyperintense T1 signal in the left cochlea, vestibule, and horizontal semicircular canal prior to contrast. There was no expansion of the internal auditory canal (Fig 1).
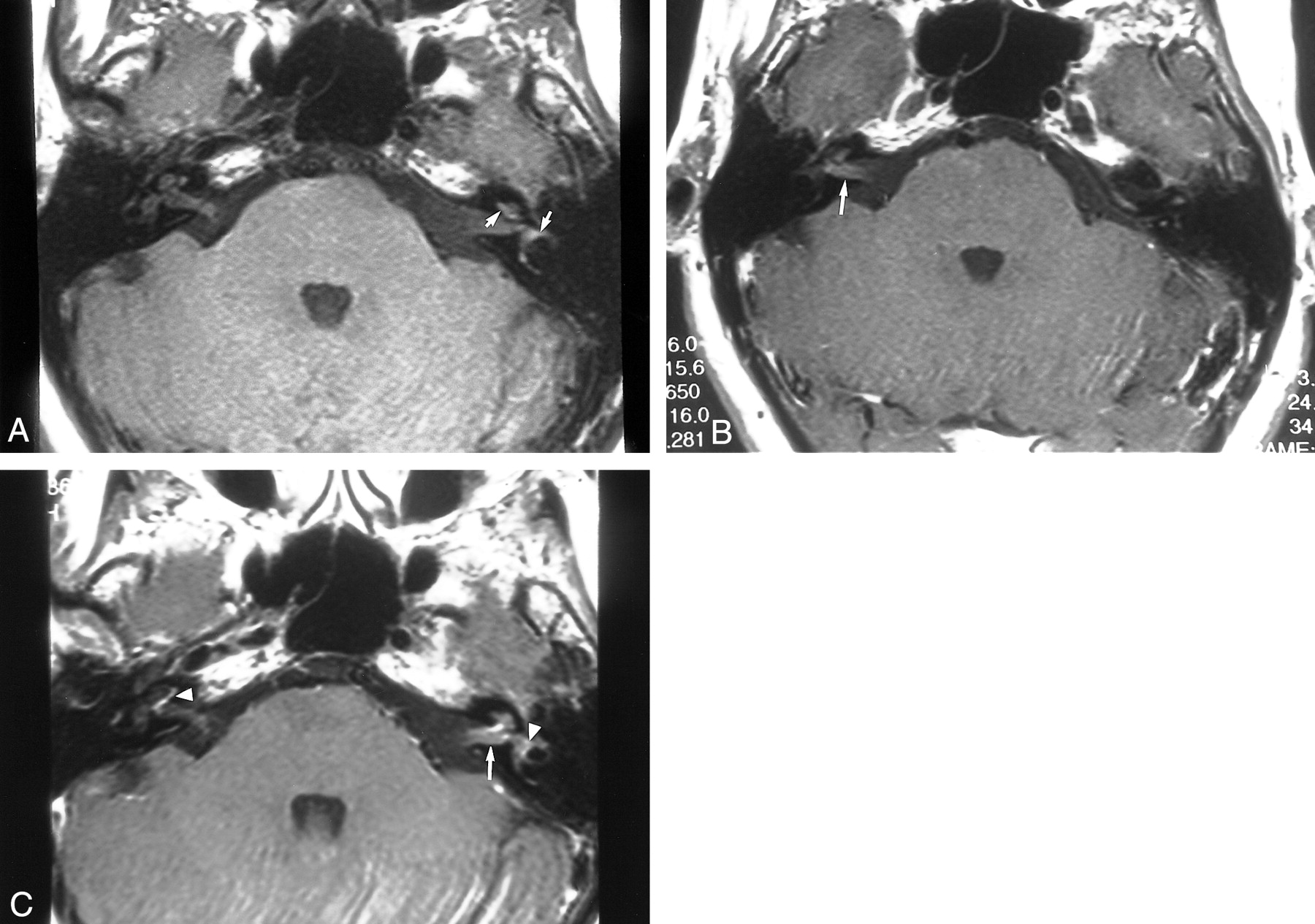
A, Precontrast T1-weighted image shows high signal from the left cochlea vestibule and horizontal semicircular canal. The signal is hyperintense with respect to brain tissue (arrows).
B and C, Contrast-enhanced T1-weighted images demonstrate bilateral enhancement of the divisions of the eighth cranial nerve (straight arrows). Also demonstrated is enhancement of the basal turn of the cochlea on the right and the vestibule on the left (C, arrowheads).
The patient was treated with intravenous acyclovir upon admission to our hospital. She also was treated with intravenous steroids for 2 days followed by a tapering dose of oral steroids for 7 more days. No significant hearing recovery was evident at discharge or during the subsequent 6 months of outpatient follow-up. Repeat audiometry showed no improvement, and brain stem evoked potentials revealed absent transmission of the auditory stimuli.
Discussion
Sudden sensorineural hearing loss is manifested by the sudden onset of unilateral or bilateral sensorineural hearing loss that is frequently accompanied by pressure in the ears, tinnitus, vertigo, and disequilibrium. Many etiologies have been suggested, such as infectious processes including viral causes (eg, varicella-zoster virus, cytomegalovirus, Epstein-Barr virus, rubella virus, parvovirus) , other infectious etiologies resulting in basal meningitis (tuberculosis, syphilis), autoimmune disorders (systemic lupus erythematosus), drugs (salicylates, aminoglycosides), and trauma.
MR imaging is an important tool for the examination of the intracranial structures. The main role of MR imaging for patients with sudden deafness is to exclude cerebellopontine angle masses and other brain lesions. MR findings in cases of SSHL have been correlated to the severity of the hearing loss, vestibular involvement, and time interval between the occurrence of SSHL and imaging. Results have indicated that the sensitivity of MR is low for detecting viral labyrinthitis in patients with SSHL (2). Strupp et al (3), in a study of patients with acute idiopathic vestibular neuritis confirmed by clinical examination and caloric irrigation, found that none of the patients' MR images exhibited contrast enhancement of the labyrinth, vestibulocochlear nerve, or vestibular ganglion even when high doses of gadopentetate dimeglumine were used.
Several other studies demonstrated contrast enhancement of the cochlea and/or vestibule in patients with sudden deafness where the etiology was proved to be viral (4). Ramsay Hunt syndrome is manifested by face and neck pain and facial palsy associated with the reactivation of varicella zoster virus. It has been reported that the geniculate ganglion is normal and the inflammatory process lies in the nerve trunks within the internal auditory canal (5). Contrast enhancement of the vestibulocochlear nerve and labyrinth has been reported in cases of Ramsay Hunt syndrome (6, 7). Tada et al (8) described enhancement of the eighth cranial nerve in addition to the seventh in only one of seven cases of cochlear and/or vestibular symptoms associated with Ramsay Hunt syndrome, which suggests scant correlation between the clinical symptoms and MR results. Dumas et al (9) reported that only three of 12 cases of vestibular neuritis demonstrated focal enhancement of the seventh and eighth nerves within the internal auditory canal. These cases were associated with an acousticofacial syndrome with severe hearing loss and facial palsy (two cases of herpes zoster oticus, one case of influenza). In these three severe cases, a meningeal reaction was revealed during cerebrospinal fluid examination.
Our patient presented with sudden SSHL with concurrent evidence of HHV-1 stomatitis and signs of meningeal irritation, the clinical aspects of which have been described by Rabinstein et al (10). Bilateral enhancement of the eighth cranial nerve within the internal auditory canal and enhancement within the labyrinth were demonstrated by MR imaging, which suggests the diagnosis of neuritis and labyrinthitis. Also shown was high signal in the left labyrinth prior to contrast media administration, likely a result of the effect of viral labyrinthitis. Weissman et al (11) reported high signal from the otic labyrinth on precontrast T1-weighted MR images of two patients who presented with sudden hearing loss and vertigo. It was suggested that the signal was caused by hemorrhage into the labyrinth in patients with viral labyrinthitis. On the basis of the literature and the data presented herein, we presume that the patient's hearing loss was a consequence of bilateral eighth-nerve neuritis secondary to HHV-1 infection, because polymerase chain reaction positive for HHV-1 in the cerebrospinal fluid is not specific for herpes encephalitis, but it is for any inflammatory process caused by HHV-1 such as meningitis and neuritis.
Conclusion
We present a case of bilateral sudden deafness in a patient with HHV-1 infection confirmed by polymerase chain reaction. The MR findings in this case of HHV-1 infection are reported, and the literature on the MR findings in cases of SSHL are reviewed.
Footnotes
1 Address reprint requests to Evelyn M.L. Sklar, M.D.
References
- Received October 16, 2000.
- Accepted after revision March 20, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.