
Abstract
Summary: We report on an 8-year-old girl with a typical attack of hemiplegic migraine, in whom MR angiography and perfusion MR imaging revealed unilateral dilation of branches of both the middle and posterior cerebral arteries and hyperperfusion of the ipsilateral hemisphere, respectively. The findings resolved spontaneously after the attack. These imaging techniques should be indicated for patients with migraine attacks and may play a role in assessing the vascular events in migraine headache.
There have been many reports on the changes in cerebral blood flow (CBF) in classic migraine attacks (1–4). Traditionally, it has been thought that a migraine headache occurs when CBF changes from constriction to dilatation of the intra- and extracranial vessels, and results from the dilatation of scalp arteries (2). On the other hand, Allan et al and Olesen et al (3, 4) reported that migraine headache is a primary pathogenic process that causes reduced CBF, and the subsequent increase in CBF is most likely a secondary phenomenon with no direct relation to the nociceptive mechanism. Thus, although the pathogenesis of the migraine remains unclear, some vascular events may be related to its etiology and symptoms. Therefore, the evaluation of cerebral perfusion during attacks is important not only to diagnose the migraine, but also to investigate its pathogenesis.
We report on a patient with hemiplegic migraine, in whom MR imaging revealed transient unilateral cerebral hyperperfusion associated with dilatation of the middle and posterior cerebral artery branches on the side contralateral to the aura during the headache phase.
Case Report
The patient was an 8-year-old right-handed girl. Although there was a family history of migraine, she had no history of migraine.
In September 1999, she presented with sudden-onset left-sided weakness during bathing, followed by a right-sided throbbing headache 2 hours later. The headache progressed into continuous severe migraine with vomiting and confusion. She was admitted to our hospital 4 hours after symptom onset. At admission, she developed intermittent headache, and neurologic examination showed left-sided hemiplegia. Blood pressure was normal. Fundoscopy revealed no evidence of papilloedema. Routine blood biochemical and hematologic indices were normal. Lumbar puncture revealed clear CSF under normal pressure with normal glucose, protein, lactate, pyruvate, and white blood cell count. During her hospital stay, further investigation was carried out to exclude a predisposing cause other than migraine for her symptoms: anti-nuclear factor, antithrombin III, lupus anticoagulant, and anticardiolipin antibodies were all within normal limits. Urinary analysis and ECG were also normal. EEG findings revealed poor organization and a lazy spindle in the right hemisphere, indicating cortical dysfunction. Left-sided hemiplegia resolved spontaneously 8 hours after onset. However, the headache remained on the right side for 3 days. On the basis of these clinical findings, a diagnosis of hemiplegic migraine was considered most likely.
MR imaging was performed when she had recovered from left-sided hemiplegia but still felt a right-sided headache 47 hours after onset and 39 hours after the resolution of left-sided hemiplegia. Routine T1-weighted images, T2-weighted images, and fluid-attenuated inversion recovery images showed no abnormalities. MR angiography (MRA) was also performed with a 3D time-of-flight sequence. This image showed dilatation of both the middle and posterior cerebral artery branches on the right side (Fig 1A). In addition, perfusion MR imaging with field echo type echo-planar imaging was performed. This image showed hyperperfusion of the right cerebral hemisphere compared with the left cerebral hemisphere (Fig 1B and C). One month later, when her symptoms were completely resolved, repeat MRA and perfusion MR imaging were performed. These images showed a symmetric appearance of the middle and posterior cerebral arteries, as well as symmetric perfusion of both cerebral hemispheres (Fig 2 A–C).

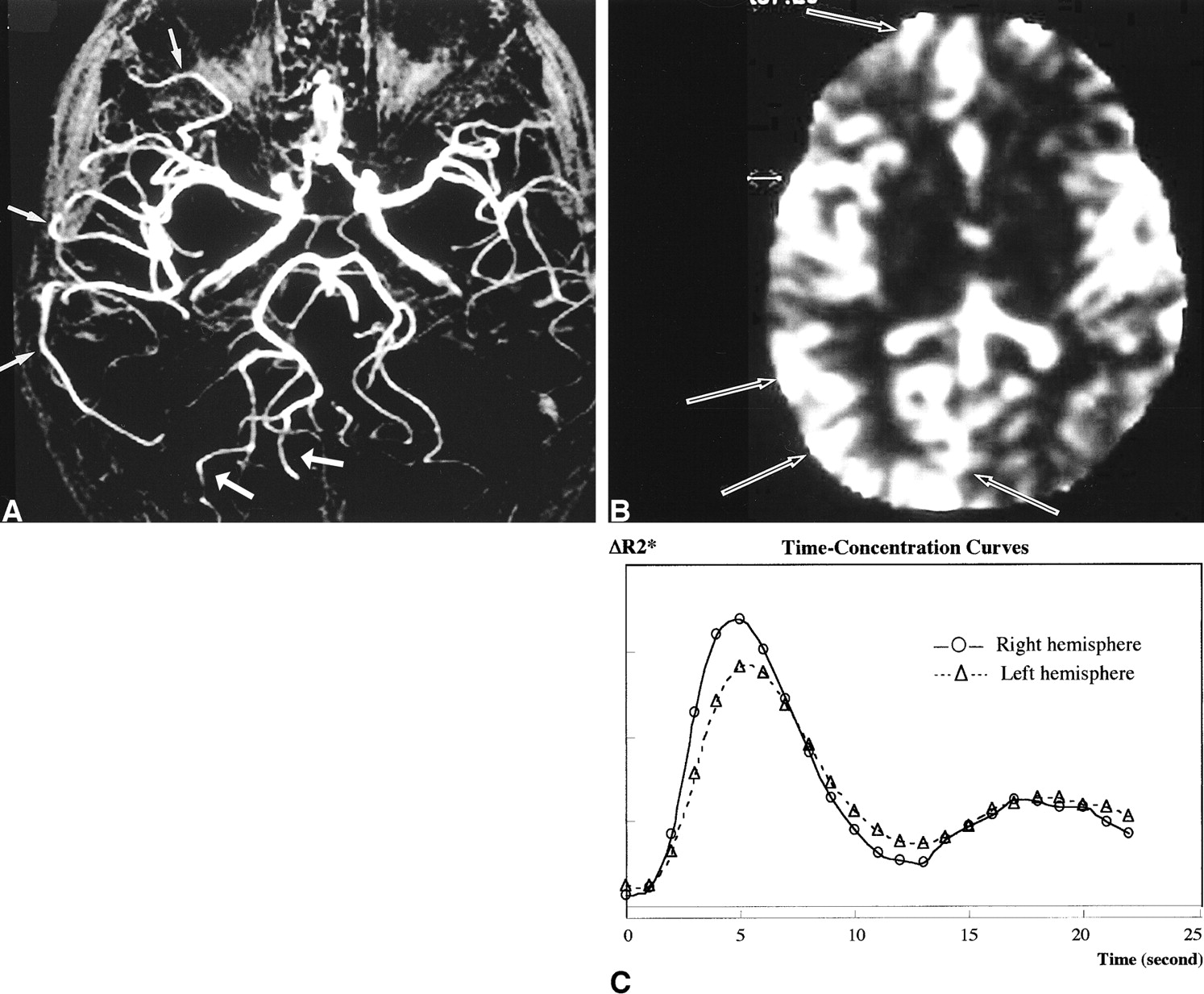
MRA and perfusion MR imaging during the headache phase.
A, MRA shows dilatation of the middle and posterior cerebral artery branches on the right side (arrows) compared with that on the left side.
B and C, Relative cerebral blood volume (rCBV) map (B), with time-concentration curves (C) based on perfusion MR imaging findings, shows hyperperfusion of the right hemisphere (arrows in B) compared with that of the left hemisphere.

Repeat MRA and perfusion MR imaging 1 month after the attack.
A, MRA shows a symmetric appearance of the middle and posterior cerebral artery branches.
B and C, rCBV map (B) with time-concentration curves (C) also shows symmetric perfusion of both cerebral hemispheres.
Since she had a recurrent attack of hemiplegic migraine 10 months after her first attack, the diagnostic criteria of this disease were satisfied.
Discussion
Classic migraine (migraine with an aura) is defined as a symptom complex that occurs periodically and is characterized by pain in the head (usually unilateral), vertigo, nausea and vomiting, photophobia, and a scintillating appearance of light. Complicated migraine, of which hemiplegic migraine is a variety, refers to the association of neurologic deficits, such as sensory, motor, or speech disturbances, with migraine headache. These neurologic deficits, which are called aura symptoms, usually precede the headache. When the attack is over, the neurologic deficit should resolve fully, but permanent neurologic sequelae may be seen (5, 6). The diagnosis of hemiplegic migraine is based on a history of recurrent attacks of weakness associated with a typical headache, as seen in the present case.
Recent studies have resulted in considerable but fragmented knowledge regarding regional variations in CBF in migraine with an aura. Skinhøj and Paulson (7) measured CBF quantitatively during the aura of a classic migraine and demonstrated a focal reduction in the hemisphere contralateral to the symptoms. Moreover, Wolff (2) mentioned that aura symptoms were associated with a reduction in CBF caused by vasoconstriction, and headache resulted from the subsequent dilatation of scalp arteries due to hyperperfusion of the extracranial vessels. These blood flow studies were conducted to support the vasospastic theory of migraine pathogenesis. Meanwhile, Olesen et al (4), using an intraarterial injection of xenon 133 for CBF studies in seven patients with classic migraine, found that CBF was reduced at the occipital pole before aura symptoms developed and spread gradually anteriorly to a varying extent, sometimes involving the whole hemisphere. They suggested that this phenomenon may be related to the spread of scintillating scotoma during a classic migraine, which is the so-called spreading depression of Leao (8). They also reported that the hypoperfusion during the aura persisted into the headache phase, and subsequent hyperperfusion usually outlasted the headache; therefore, they suggested that nociception may be initiated by a spreading depression that, by some unknown mechanism, triggers the painful phase of the attack and may be closely related to vasoactive events (1, 4). Thus, to understand the pathogenesis of a migraine headache, it is important to evaluate the changes in cerebral perfusion during the attack. However, considering the technical limitations of the previous CBF studies and inherent difficulty in studying acute migraine attacks, it is not easy to demonstrate the sequential changes in the cerebral perfusion during a migraine attack. Unfortunately, in our present case, MRA and perfusion MR imaging could not be performed during the aura phase, but they did reveal that cerebral hyperperfusion occurred during the headache, and that perfusion normalized between attacks.
One report has stated that MRA showed unilateral dilatation of middle cerebral artery branches in a patient with hemiplegic migraine (9). However, we could not find a previous report that described unilateral hyperperfusion during the headache phase by perfusion MR imaging.
Although the routine use of vascular imaging may not be necessary to assess a migraine headache, MRA and perfusion MR imaging can reveal the physiologic changes in a child with acute severe headache, in whom routine MR imaging has shown the absence of a well-defined lesion, such as a tumor or hydrocephalus. Furthermore, these imaging techniques can be easily added to routine MR and are an easy-to-apply method for evaluating cerebral perfusion in migraine attacks. Thus, we believe that these techniques are useful not only for diagnosing hemiplegic migraine, but also may play a role in our future understanding of the pathogenesis of migraine.
Footnotes
1 Address reprint request to Hidetsuna Utsunomiya, Department of Radiology, Fukuoka University School of Medicine, 7–45–1 Nanakuma, jonan-ku, Fukuoka 814–0180, Japan.
- Received October 24, 2000.
- Accepted after revision March 15, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Stroke Mimics in the Acute Setting: Role of Multimodal CT Protocol
- Biphasic neurovascular changes in prolonged migraine aura in familial hemiplegic migraine type 2
- Acute-Onset Migrainous Aura Mimicking Acute Stroke: MR Perfusion Imaging Features
- Neurovascular changes in prolonged migraine aura in FHM with a novel ATP1A2 gene mutation
- Susceptibility-Weighted Imaging in Migraine with Aura