
Abstract
Summary: We report the MR features in a previously healthy patient with mucosa-associated lymphoid tissue lymphoma of the pituitary gland. The MR images showed a homogeneously enhancing solid mass in the sellar region and both parasellar regions; this mass extended through the bilateral foramina ovale along the third branches of the trigeminal nerves. The mass completely encircled the cavernous segments of both internal carotid arteries without narrowing the lumen. Gadopentetate dimeglumine–enhanced T1-weighted MR images showed homogeneous, strong enhancement of the mass.
The number of primary CNS lymphomas have increased in both immunocompromised and immunocompetent subjects. However, only four cases of pituitary lymphoma have been previously reported: one case in a patient with acquired immunodeficiency syndrome, one case of T-cell lymphoma, and two cases of B-cell lymphoma (1–4). To our knowledge, no cases of mucosa-associated lymphoid tissue (MALT) lymphoma of the pituitary gland are reported. MALT lymphoma is an extranodal type of malignant lymphoma of B-cell origin. It tends to arise within tissues involved by chronic inflammatory disorders of autoimmune or infectious origin and remains localized for prolonged periods at the site of origin (5). We describe the MR features of MALT lymphoma that manifested as a sellar and parasellar mass extending through both foramina ovale along the third branches of the trigeminal nerves in a previously healthy patient.
Case Report
A 42-year-old man who had had no previous illnesses was admitted to the hospital because of blurred vision and a foreign-body sensation on his left eye lasting for 3 months. In addition, he also complained of the loss of libido of 2 month’s duration. Findings on physical examination were normal except for a visual-field defect on the temporal side of his left eye. No abnormalities were found in his bilateral ocular movement, facial sensory function, or motor function. His blood count and biochemical profile were normal. Results from the basal hormonal studies suggested panhypopituitarism with a slight elevation of the serum prolactin level and a decreased serum thyroid-stimulating hormone (TSH) level despite a low serum testosterone level.
MR examination was performed to evaluate a suspected parasellar lesion. MR imaging demonstrated a sellar mass with supra- and parasellar extension. This mass was isointense to gray matter on T1-weighted images (Fig 1A), slightly hypointense on T2-weighted images (Fig 1B), and homogeneously enhancing on contrast-enhanced T1-weighted images (Fig 1C). The optic chiasm was displaced in a cephalic direction, and both cavernous segments of the internal carotid arteries were completely encased by the mass, with mild narrowing of the lumen of the left internal carotid artery. It also extended extracranially along the mandibular branches of the trigeminal nerve through the widened foramina ovale. Additionally, coronal MR images demonstrated focal bony erosion due to the mass on the left side of the sphenoid body. Contrast-enhanced sagittal T1-weighted images (Fig 1D) showed an unusually long dural tail along the clivus. The differential diagnosis based on the MR imaging findings included invasive pituitary adenoma, meningioma, metastasis to the pituitary gland, lymphocytic hypophysitis, and granulomatous disease.

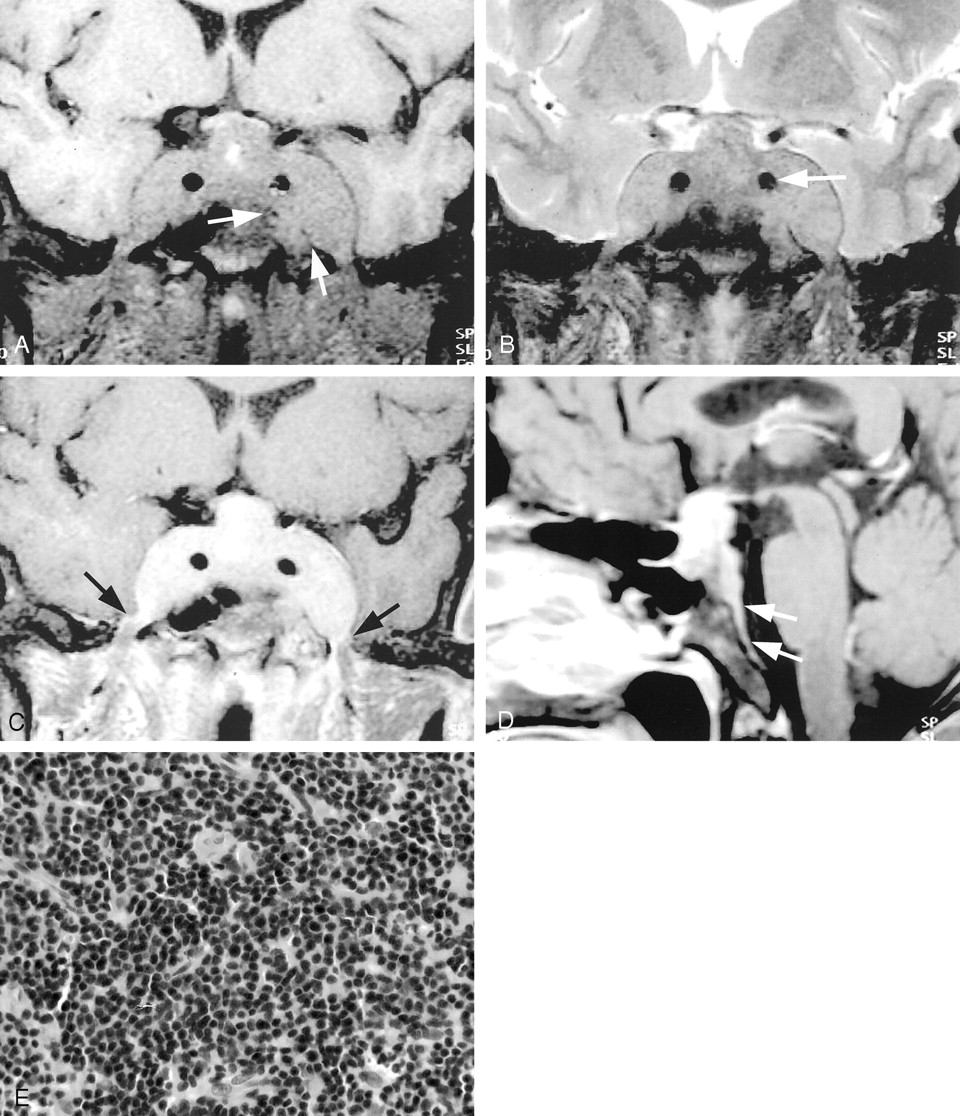
Images in a 42-year-old man with 3-month history of blurred vision and a foreign-body sensation in his left eye.
A, Coronal fat-saturated T1-weighted MR image (TR/TE/NEX, 645/14/2) reveals an isointense mass in the sellar and suprasellar areas. The mass invades both parasellar regions and extends extracranially along both third branches of the trigeminal nerves through the widened foramina ovale. Note the focal bony erosion due to the mass (arrows) on the left side of the sphenoid body. The high signal intensity in the sellar mass suggests focal hemorrhage in the residual pituitary gland.
B, Coronal fat-saturated T2-weighted MR image (4300/132/3) shows the slight hypointensity of the mass. Note the mild luminal narrowing of the cavernous segment of the left internal carotid artery (arrow) compared with that of the contralateral side.
C, Contrast-enhanced fat-saturated coronal T1-weighted MR image (645/14/2) shows homogeneous, strong enhancement of the mass. Diffuse thickening of the mandibular branches of both trigeminal nerves (arrows) within the widened foramina ovale is also demonstrated. Note the strong enhancement of the left side of the mandibular nerve.
D, Contrast-enhanced fat-saturated sagittal T1-weighted MR image (645/14/2) demonstrates tumor spread along the clival dura with a long dural tail (arrows).
E, Photomicrograph of the specimen shows a lymphoproliferative lesion composed of centrocyte-like lymphocytes and cells with plasmacytoid features (hematoxylin-eosin stain, original magnification ×400).
Endoscopic surgery was performed with a trans-sphenoidal approach. Microscopic examination of the surgical specimen (Fig 1E) demonstrated a lymphoproliferative lesion and some non-neoplastic tissue. The lymphoproliferative lesion had positive results with leukocyte common antigen CD79a and negative results with CD3, CD5, CD23, cycline D1, terminal deoxynucleotide transferase (Tdt), and kappa- and lambda-chain immunohistochemical tests. By combining these results, the mass was confirmed as a low-grade MALT lymphoma of the pituitary gland. A staging workup examination with physical examination and chest and abdominal CT were performed, but no primary site of the tumor was identified. The patient was offered systemic chemotherapy and was grossly free of symptoms for the 6 months of clinical follow-up.
Discussion
The incidence of CNS lymphoma has increased in both immunocompromised and immunocompetent subjects. Studies of CNS lymphomas demonstrate they have an affinity for meningeal surfaces, especially in periventricular regions (6). Frequent involvement of the third ventricle wall with extension to the suprasellar and hypothalamic regions has been described (6). Primary lymphoma of the pituitary gland is extremely rare, and an extensive search of the literature revealed only four cases of primary lymphoma of pituitary gland; one of these was found on postmortem examination of a patient with acquire immunodeficiency syndrome (1–4). To our knowledge, no cases of MALT lymphoma of the pituitary gland have been reported in the literature.
MALT is widely distributed in the aerodigestive tract and is composed of nonencapsulated localized aggregates of lymphocytes thought to be responsible for mucosal immunity (7). The category of MALT lymphoma encompasses a heterogeneous group of B-cell tumors that arise primarily within the extranodal tissues, such as the stomach, lung, orbit, skin, pancreas, breast, salivary glands, lacrimal glands, and thyroid. They are predominantly tumors that occur in middle-aged adults, and, compared with other types of B-cell lymphomas, they have unique clinical features. These tumors tend to arise within tissues involved by chronic inflammatory disorders of autoimmune or infectious origin. They remain localized for prolonged periods at the sites of origin, spreading systemically only late in their course. Also, they respond favorably to various treatment modalities, including chemotherapy and radiation therapy, with a highly favorable prognosis (8).
To our knowledge, the imaging findings of MALT lymphoma in the head and neck are not reported, and only a limited number of reports describe the radiologic findings of lymphoma of the pituitary gland (1, 3, 4). On T1-weighted MR images, primary lymphomas of the CNS are typically isointense or slightly hypointense relative to the gray matter, and they produce relatively little mass effect for their size (3, 9). The lesions appear hypo- to isointense relative to the gray matter on T2-weighted images, and they are strongly enhancing with the administration of contrast agents (9). In one report of a primary B-cell lymphoma of the pituitary gland, Singh et al (3) emphasized the finding of cavernous sinus invasion without narrowing of the carotid artery lumen as a helpful sign in differentiating lymphoma from meningioma.
The MR findings of MALT lymphoma in this case were similar to those of other types of lymphoma. In our case, contrast-enhanced T1-weighted MR images showed perineural spread of the tumor along the third branches of both trigeminal nerves. Perineural spread is a well-known property of head and neck tumors that invade the skull base. Tumor can selectively follow a nerve or the sheath of a nerve to reach and ultimately pass through a foramen of the skull base; this feature is well known in lymphoma (10). Another feature in this patient that deserves mention is the presence of a long dural tail. On MR images, the dural tail represents enhancement of the thickened dura adjacent to and tapering away from a dura-based lesion. The dural tail was first described as the thickening of dura surrounding meningiomas, but it is also seen when lesions are associated with the dura, whether they are primarily dura-based or whether they extend secondarily to the dura (11). However, in our case, the dural tail was unusually long compared with findings with other tumors (eg, meningioma), and it suggested the infiltrative nature of the lesion. To our knowledge, the MR features have not been previously reported for the other pathologic conditions involving the pituitary gland. Therefore, MR findings in a pituitary tumor with a propensity for perineural spread and an infiltrative growing pattern should be helpful in suggesting the possibility of lymphoma.
In our case, the differential diagnosis included invasive pituitary adenoma, meningioma, metastasis to the pituitary gland, lymphocytic hypophysitis and granulomatous disease, and Langerhans cell histiocytosis. Invasive pituitary adenoma and meningioma are the most common tumors of the sellar region in adults. They may have MR signal intensity characteristics that are similar to those of lymphoma; however, they do not spread perineurally, and they do not usually have a long dural tail. Metastasis to the pituitary gland was the second consideration of our differential diagnosis. On MR images, metastasis usually appears as a dumbbell-shaped intra- and suprasellar tumor with only a small indentation at the level of the diaphragm sellae, or it appears as a suprasellar tumor that invades rather than displaces the infundibular recess of the third ventricle. Metastasis usually does not show sellar enlargement because of the relatively rapid tumor growth (12). Lymphocytic hypophysitis is a rare inflammatory disease of the pituitary gland that frequently affects young women during late pregnancy or in the postpartum period. MR images usually show this as an intensely enhancing pituitary mass associated with strips of enhancing dura mater adjacent to the mass with or without extrapituitary involvement in the subarachnoid space, sphenoid sinus, or cavernous sinus. In this patient, lymphocytic hypophysitis could not be differentiated from lymphoma with only the MR imaging findings, but the clinical findings made lymphocytic histiocytosis less likely (13).
In summary, our MR findings in MALT lymphoma that involved the pituitary gland were similar to the findings in other types of lymphoma. For prognostic and therapeutic reasons, the identification of the MR findings in MALT lymphoma of the pituitary gland may be helpful in evaluating sellar and parasellar pathologies.
Conclusion
Despite the rarity of MALT lymphoma of the pituitary gland, the MR findings of a sellar and parasellar mass with perineural extension and a long dural tail should suggest the possibility of MALT lymphoma, as well as other more common pathologic entities.
References
- Received November 8, 2001.
- Accepted after revision December 19, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.