
Abstract
Summary: After experiencing gradual, progressive sensorineural hearing loss, a patient underwent cochlear implant (CI) surgery. Postoperatively, the patient experienced vestibular symptoms with no improvement in hearing. High-resolution temporal bone CT scanning demonstrated extracochlear positioning of the CI electrode in the superior semicircular canal.
High-resolution temporal bone CT scanning is often used to establish a cause of sensorineural hearing loss or to detail labyrinthine anatomy preoperatively in cochlear implant (CI) placement surgery. CT scanning is infrequently indicated postoperatively in CI surgery. Evaluation of position of the cochlear implant device may be indicated if conventional radiography is insufficient to determine the electrode position or if the patient experiences postoperative complications. Our case demonstrates improper positioning of a cochlear implant electrode.
Case Report
An 81 year-old female patient was referred to the otolaryngology department for sensorineural hearing loss with little or no improvement with the use of hearing-aid devices. She had experienced a gradual decline in hearing over a 15-year period. She was taking no ototoxic medications.
On physical examination, there was no response to tuning fork tests, even after cerumen disimpaction. The patient was sent for audiologic testing, which revealed a moderately severe to profound sensorineural hearing loss in the right ear and a severe to profound sensorineural hearing loss in the left ear in the 0.25–8-kHz range. Additional audiologic testing included the Central Institute for the Deaf everyday sentences in sound field at a 60-dB hearing level through a speaker at a 45° azimuth. Testing was completed with monaural right, monaural left, and binaural amplification with hearing set to desired sensation levels. The patient scored 0% based on the number of key words correctly identified in all conditions. On the basis of these test results, the patient was referred for cochlear implant surgery. Imaging was deferred at this time.
At surgery, after placement of a facial nerve monitor, the right posterior auricular skin was incised continuing superiorly to the temporalis muscle, where a pocket for the cochlear implant (CI) device was created. A mastoidectomy was created within the posterior auditory canal wall toward the antrum. Important mesotympanic landmarks including the incus, lateral border of the bony portion of the lateral semicircular canal, and the facial nerve recess were identified. The facial nerve recess was opened to expose the incudostapedial joint, cochlear promontory, round window, and round window niche. A cochleostomy through the round window allowed introduction of the CI electrodes. The cochleostomy was then sealed with a piece of fascia.
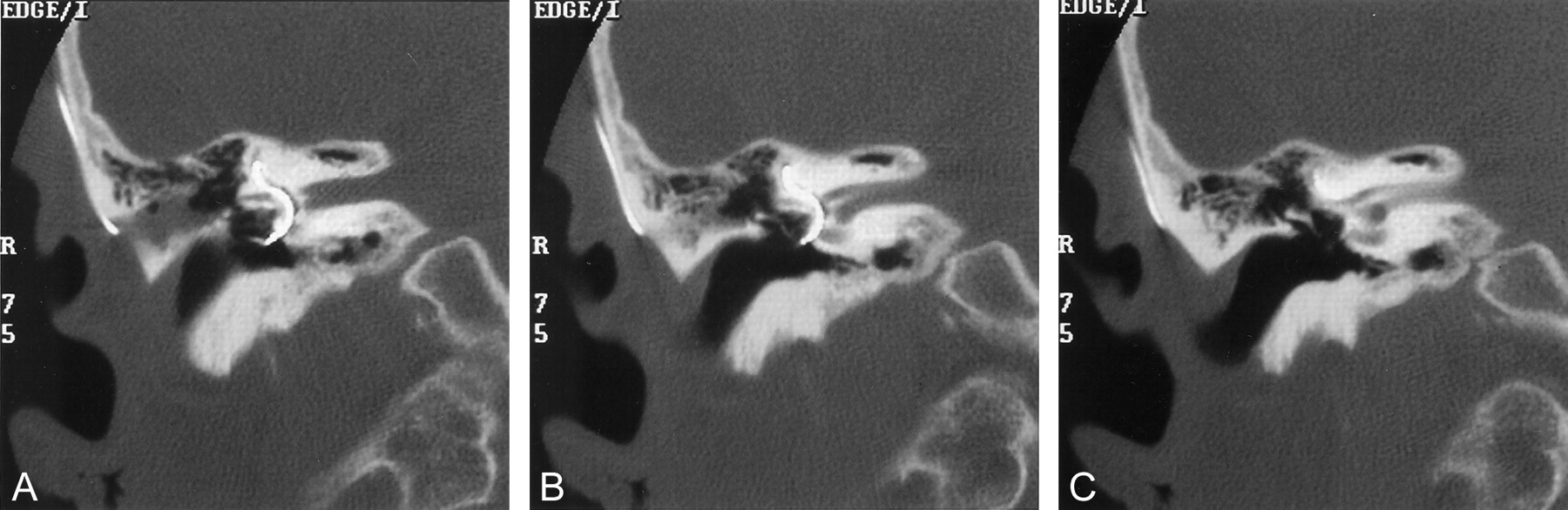
The patient’s postoperative course was complicated by unrelenting dizziness and poor hearing response. High-resolution temporal bone CT scanning using 1-mm sections was performed. Axial images (Fig 1) demonstrate mastoidectomy posterior to the external auditory canal and a CI electrode position at the round window. Superiorly the electrode is seen within the vestibule and continuing anteriorly at the level of the lateral semicircular canal.

High-resolution axial images of the temporal bone demonstrate correct positioning of the CI electrode proximally at the round window but then taking an abnormal course.
A, Mastoidectomy and CI electrode positioned at the round window.
B, The electrode is positioned within the vestibule.
C, At the level of the lateral semicircular canal and internal auditory canal, the electrode is seen anteriorly still within the vestibule.
Consecutive 1.0-mm coronal images (Fig 2) at the level of the internal auditory canal demonstrate the path of the electrode from the round window to the vestibule and then coiled in the superior semicircular canal. The basal and middle turns of the cochlea are seen with no electrode in place.
High-resolution coronal images of the temporal bone demonstrate the entire labyrinthine path of the CI electrode.
A, The electrode is seen entering the round window but then within the vestibule and continuing into the superior semicircular canal.
B, A portion of the extralabyrinthine electrode is seen along the junction of mastoid and squamosal portions of temporal bone, deep to the temporalis muscle.
C, The basal turn of the cochlear is seen with no electrode in place.
Dizziness resolved with improved hearing after revision of the CI. Postoperative audiology testing showed word discrimination and sentence recognition scores ranging from 80–100%. In addition, the patient was able to understand telephone speech. Overall, her performance showed that she was hearing a large portion of the speech signal intensity and interpreting it correctly.
Discussion
CI device implantation is indicated for profound sensorineural hearing loss. Preoperative high-resolution temporal bone CT can demonstrate cochlear patency and detail middle and inner ear anatomy (1). In particular, attention is paid to the posterior tympanum and inner ear structures to establish normal anatomy and avoid surgical pitfalls (2, 3). Detectable contraindications include obliterative labyrinthine ossification, severe cochlear or fenestral otosclerosis, congenital cochlear malformation, severe bilateral temporal bone fractures, and infected middle ear cavities (3). Preoperative CT scanning can be useful in selection of the better ear for implantation (3, 4).
Many centers obtain intraoperative radiographs for electrode position assessment. The generally low quality of portably acquired intraoperative radiographs and the detail required for fine labyrinthine structures, however, will often lead to postoperative imaging (5). Several radiographic techniques have been described that can adequately assess electrode position (1, 6). Radiographic techniques, however, rely on precise patient positioning and occasionally may be difficult, particularly with young children, and CT scanning may be required (5). In addition, certain unexpected postoperative complications may lead to postoperative CT scanning. Postoperative complications include facial nerve paralysis, infection, fluid drainage, meningitis, cochlear damage during insertion, osteogenesis, vestibular symptoms, malposition or breakage of the electrode, and damage to the mastoid segment of the facial nerve (2).
In a study of 141 patients receiving CIs, intraoperative or postoperative radiographic techniques were adequate to establish electrode position in 135 patients. Nine patients had postoperative temporal bone CT scanning to establish intracochlear electrode positioning, to evaluate for infection, or to address unexpected complications. CT scanning was useful in all cases to establish intracochlear versus extracochlear electrode positioning. In two patients, a fluid collection was found deep to the receiver/stimulator, and in one patient necrosis of the surgical flap was identified (7).
There is interest in developing speech-processing algorithms that map speech frequencies to specific intracochlear positions (8). For this purpose, precise position and insertion depth has been a subject of research using CT scanning with three-dimensional reconstruction (2, 8–10). Neither conventional radiography nor CT scanning has been deemed entirely adequate for precise localization of each intracochlear electrode. For this, a fusion technology of coregistration of CT scans and conventional radiographs has been investigated (11). The optimal position of the electrodes is thought to be along the inner wall of the cochlear (perimodiolar) and therefore closer to the spiral ganglion cells, the target of electrical stimulation, rather than more peripherally located in the scala tympani (12–15). Deeper insertion is desirable as well because lower frequency perception is conveyed in the apical spiral ganglion cells (6).
Ideal positioning is currently the subject of research, whereas correct positioning is the subject of this case and of clinical practice. As in our case, the cochlear implant electrodes may pass from the scala tympani into the scala vestibuli by piercing the basilar membrane. It may thus enter the vestibule and pass into the superior semicircular canal, which can cause significant vestibular symptoms. CT scanning was useful in our case to establish the extracochlear electrode position and to eliminate other causes of the patient’s symptoms, such as postoperative infection.
Conclusion
The indications for preoperative assessment of the temporal bone wiht HRCT for cochlear implantation are firmly established. Postoperative assessment with HRCT may be indicated in complicated cases and has been shown to be helpful, as in the present case. Current research indicates that precise electrode localization, as can be determined with HRCT and 3D reconstruction, may be important in hearing optimization.
References
- Received March 28, 2003.
- Accepted after revision April 6, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.