
Abstract
BACKGROUND AND PURPOSE: Currently available stents for intracranial use usually are balloon-expandable coronary stents that carry the risk of damaging a dysplastic segment of the artery, with potential vessel rupture. We assessed the technical feasibility and efficacy of the combined application of a flexible, self-expanding neurovascular stent and detachable coils in the management of wide-necked intracranial aneurysms in humans.
METHODS: Four consecutive patients with a wide-necked intracranial aneurysm were treated with a combined approach that consisted of delivery of a flexible self-expanding neurovascular stent through a microcather to cover the neck of the aneurysm and subsequent filling of the aneurysm with coils through the stent interstices. The aneurysms were located at the internal carotid artery (n=2) and the basilar tip encroaching the P1 segment (n=2). Previous attempts with conventional endosaccular coil packing alone failed in all cases.
RESULTS: Stent placement in the desired position with complete or nearly complete occlusion of the aneurysms was feasible in all patients. In one patient, aneurysm perforation with the microcatheter occurred and necessitated ventricular drainage, which led to a large parenchymal and intraventricular hemorrhage because of the strong anticoagulation regimen. Six-month follow-up demonstrated no focal neurologic sequelae in any of the patients, except slight memory dysfunction in the patient with bleeding.
CONCLUSION: Preliminary data demonstrate that this extremely flexible stent is technically easy to deploy and can be easily and safely maneuvered through severely tortuous vessels, enabling the treatment of intracranial wide-necked aneurysms. The combination of endovascular reconstruction of the parent vessel with use of a self-expanding stent followed by coil embolization offers a promising therapeutic alternative for wide-necked aneurysms not amenable to coil embolization alone. Although immediate angiographic results are promising, long-term angiographic and clinical follow-up is essential to determine permanent vessel patency and aneurysm occlusion rate.
The endovascular approach is an elegant alternative to craniotomy and neurosurgical clipping of cerebral aneurysms. In many aneurysms, endovascular therapy is feasible, specifically in those with a small neck. Despite enormous advancement in the development of flexible microcatheters, coil configurations, and embolic materials, wide-necked aneurysms still remain a therapeutic challenge. The geometry of wide-necked aneurysms sometimes makes it impossible to treat the aneurysm through the endovascular route or at least reduces the possibility of obtaining satisfactory coil packing. However, incomplete occlusion carries the risk of aneurysm recanalization, regrowth, and rerupture (1, 2).
The technique of using an intravascular stent to create a bridging scaffold followed by endovascular placement of coils through the interstices of the stent into a wide-necked or fusiform aneurysm has been described in experimental studies (3–5) and in humans (6–14). This technique may provide another treatment option for patients with wide-necked aneurysms in whom direct surgical clipping or conventional endovascular therapy would be difficult or impossible, and in whom parent artery occlusion is not a feasible option. However, currently available stents are not optimized for intracranial use. Stents used for intracranial treatment, usually coronary stents, are balloon expandable and carry the risk of damaging a dysplastic segment of the artery, with potential vessel rupture. In addition, the large profile and relative stiffness of the delivery systems, not intended for intracranial vessels, limit the locations that are safely accessible and increase the risk of vessel dissection.
We studied the technical feasibility and efficacy of a new, extremely flexible, self-expanding neurovascular stent in combination with subsequent coil embolization for the treatment of wide-necked intracranial aneurysms. To our knowledge, this is the first experience with this device reported in the literature.
Methods
Patients and Protocol
From August 2001 to October 2001, four consecutive patients (three women, one man; age range, 43–49 years) with a wide-necked intracranial aneurysm were treated with the Neuroform microdelivery stent system (Smart Therapeutics, Inc./Boston Scientific, San Leandro, CA) and detachable platinum coils. We obtained approval from our ethics committee to study the use of this new self-expanding stent to treat wide-necked aneurysms in which surgical clipping was not considered and in which coil treatment alone was impossible or failed previously. According to the study protocol, all aneurysms had to be additionally treated through the stent interstices with detachable coils even when stasis of contrast material was noted after stent placement. The reason for the combined treatment was the necessity for postprocedural antiplatelet therapy, which could interfere with aneurysm thrombosis.
The protocol inclusion criteria were a wide-necked intracranial saccular aneurysm (ruptured or nonruptured), defined as an aneurysm with a dome-to-neck ratio less than 2.0 and/or a neck length of 4 mm or more, confirmed at digital subtraction angiography (DSA) by using external fiducial markers on the patient’s head; parent artery with a diameter between 1.5 and 5.5 mm; patient age older than 18 years; and provision of written informed consent.
Exclusion criteria were fusiform or other nonsaccular aneurysms, neck length larger than 1.2 cm, pregnancy, medical condition not allowing follow-up, and contraindication to study medication (aspirin, heparin, clopidogrel, radiographic contrast agent).
In all patients, conventional endovascular embolization with Guglielmi detachable coils (GDCs) (Boston Scientific, Neurovascular Division, Fremont, CA) had been attempted at an earlier date but failed because of coil herniation into the parent vessel owing to the broad base of the aneurysm.
Aneurysms were located at the paraophthalmic and cavernous segment of the internal carotid artery in two patients and at the basilar tip incorporating the P1 segment on one side in the other two patients. According to the study protocol, all patients were premedicated with antiplatelet therapy consisting of aspirin 300 mg and clopidogrel 225 mg one day before the procedure. Clopidogrel 75 mg each day was continued for an additional 30 days, and aspirin 300 mg for life. All patients received heparin to raise the activated clotting time 2–3 times compared with the baseline during the procedure and for the following 24 hours.
Feasibility of stent deployment and the aneurysm occlusion rate were documented. Every patient underwent a cranial MR imaging examination including MR angiography within 3 days after the procedure to evaluate MR compatibility of the stent in combination with the GDC. We analyzed the clinical status in every patient at 3 and 6 months after treatment; three of four patients underwent follow-up angiography at 6 months. One patient (patient 3) denied follow-up DSA.
Microdelivery Stent System
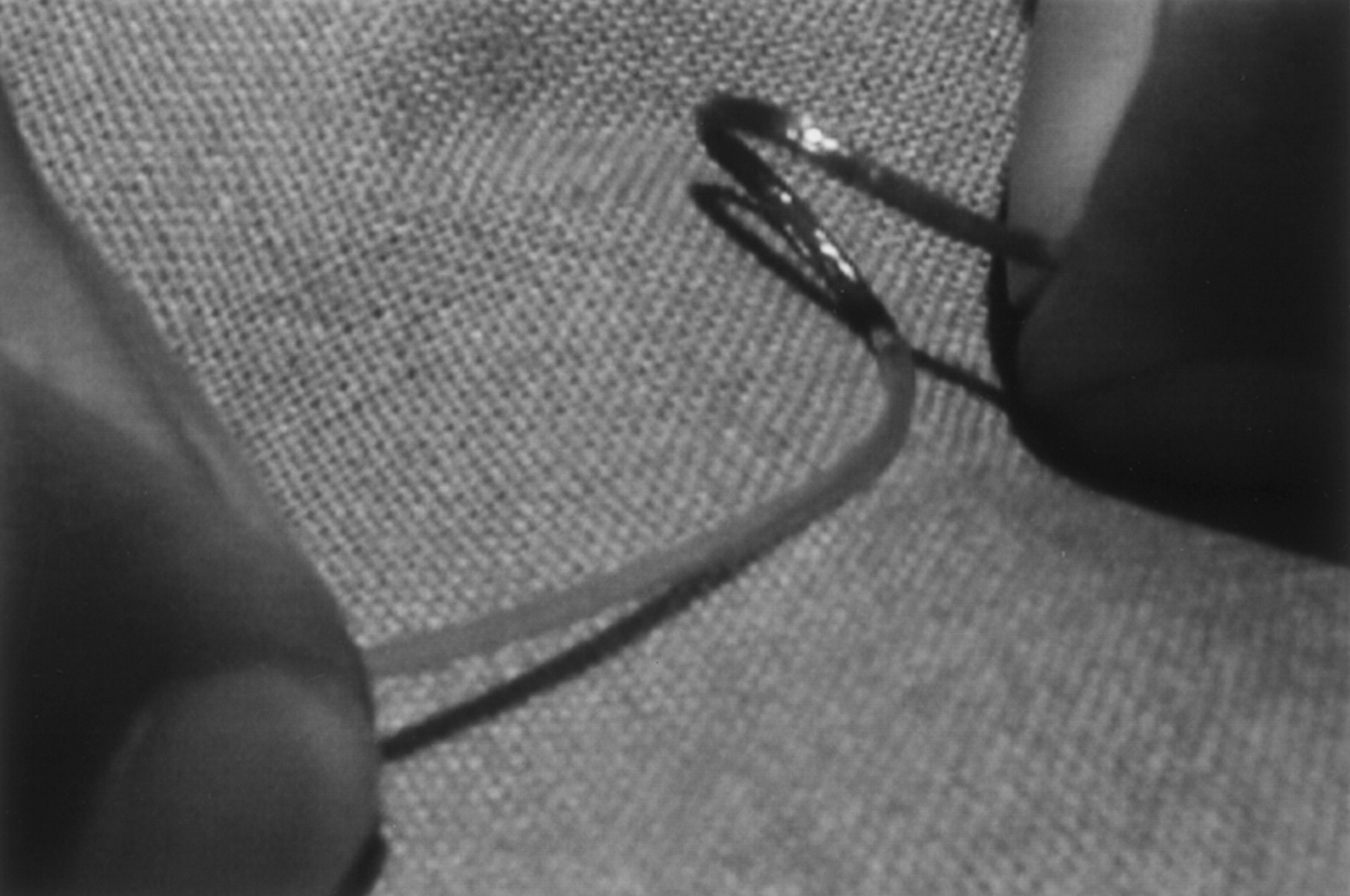
The self-expanding intracranial microdelivery stent system is divided into three parts: the self-expanding stent itself, a 3F delivery microcatheter, and a stabilizer. The stent consists of multiple segments, each consisting of interconnected beam elements in a circumferential array. Adjoining segments are connected with elements that allow rotation about the longitudinal axis, permitting high flexibility (Fig 1). Four platinum marker bands are placed at each end to delineate the proximal and distal parts of the stent under fluoroscopy. The system is compatible with guiding catheters that have a minimum diameter of 0.050 inch.
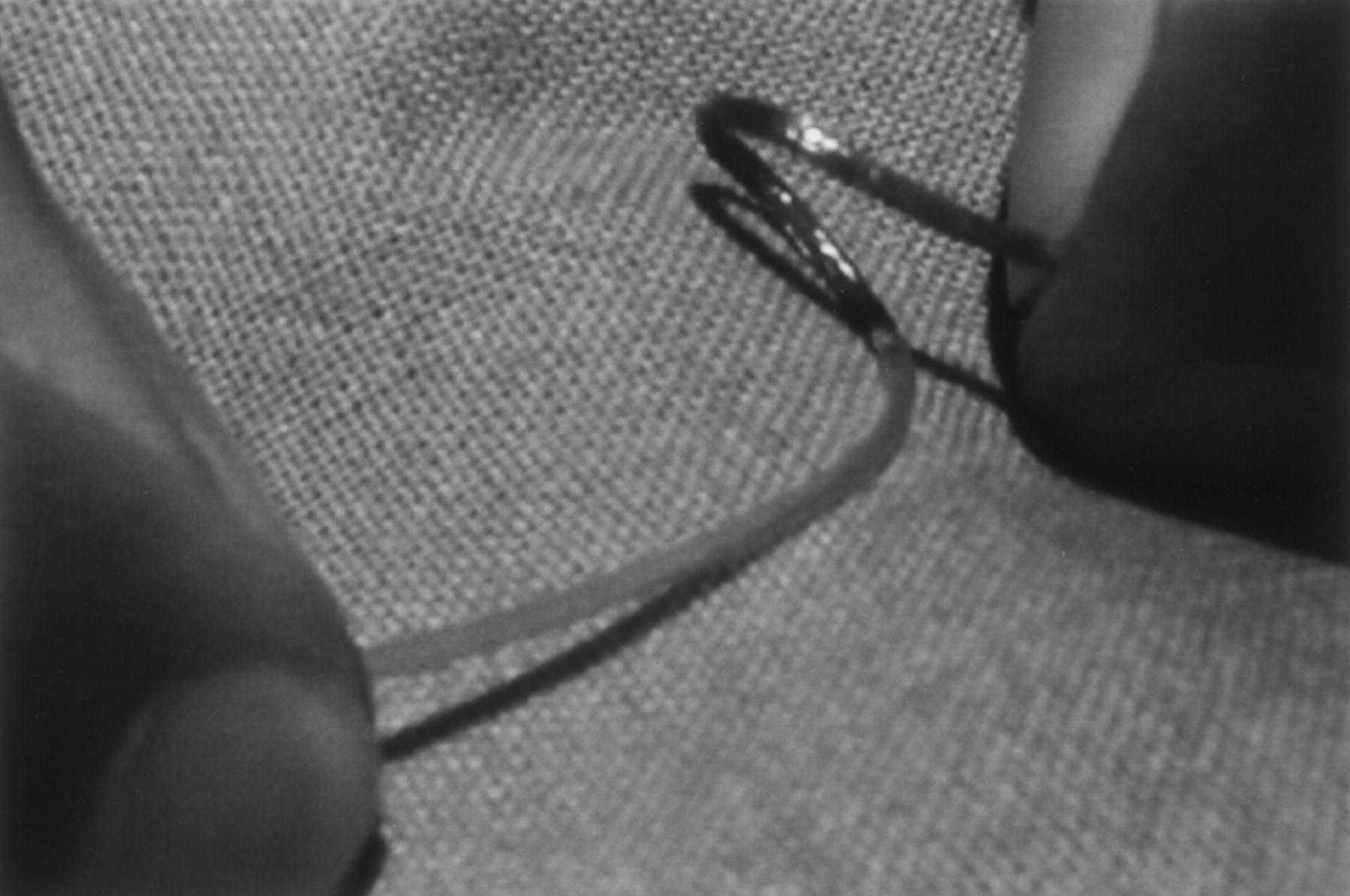
Photograph of the self-expanding stent demonstrates the extreme flexibility of the stent system.
Technique of Stent Deployment and Endosaccular Coiling
The stent is preloaded in a 3F delivery microcatheter. A separately packaged stabilizer is inserted through the hub of the stent delivery microcatheter until its tip abuts the stent. The stabilizer is essentially a 2F microcatheter that can be placed inside the 3F stent delivery microcatheter over a 0.014-inch wire. The stent delivery microcatheter and stabilizer are advanced over an exchange wire as a unit and positioned until the aneurysm neck is centered between the ends of the stent. The stent is deployed by gently retracting the microcatheter while holding the position of the stent fixed with the stabilizer. This unsheathes the stent and allows expansion within the vessel. As the stent deploys, the four marker bands on each end define the endoluminal surface. After deployment of the stent, the stent system with the exchange wire is removed, and a microcatheter with a preshaped soft microguidewire (Transend-14; Boston Scientific, Fremont, CA) can be used to enter the aneurysm through the interstices of the stent. Finally, detachable coils are introduced into the aneurysm and detached as usual until occlusion is achieved. After sufficient packing of the aneurysm, the microcatheter is pulled back (Fig 2).

Schematic illustrates the combined treatment of primary stent placement and subsequent coil embolization for wide-necked aneurysms.
Case Reports
Case 1 (Fig 3).

Case 1. Wide-necked paraophthalmic aneurysm (dome, 5.5 × 8 mm; neck, 5 mm).
A and B, DSA images obtained before (A) and after (B) combined therapy with the self-expanding stent and GDCs demonstrate complete obliteration. The patient had two additional aneurysms (at the AcomA and basilar artery) previously treated with GDCs alone.
C and D, Source images of time-of-flight MR angiography reveal no stent-related artifacts and normal flow-void signal intensity of the internal carotid artery. Arrows in D indicate coil mass.
E, Follow-up angiogram after 6 months reveals complete aneurysm occlusion.
A 49-year-old woman presented with dizziness. On cranial MR images, there was suspicion of an aneurysm of the anterior communicating artery (AcomA). DSA revealed three aneurysms located at the AcomA, at the basilar tip, and at the paraophthalmic segment of the right internal carotid artery (Fig 3A). Except for the paraophthalmic aneurysm, all aneurysms were treated with endosaccular packing alone. The broad-based paraophthalmic aneurysm (dome, 5.5 × 8 mm; neck length, 5 mm) was impossible to coil with the conventional technique because coils did not remain within the aneurysm. Because the patient refused neurosurgical treatment, stent implantation and secondary coiling were planned. We implanted a 4.5 × 15-mm self-expanding stent and then introduced six detachable platinum coils (GDC 10: 7/30, 4/10, 3/8, 3/8, 3/4 ultrasoft, 3/4 ultrasoft) (Fig 3B). Clinical examination at discharge and during follow-up revealed no neurologic deficit. No stent-induced artifacts were noted on MR images (Fig 3C and D). Follow-up angiogram after 6 months revealed complete aneurysm occlusion (Fig 3E).
Case 2 (Fig 4).

Case 2.
A, Angiogram reveals previously coiled recurrent aneurysm (arrows) of the cavernous internal carotid artery.
B, Angiogram obtained after stent deployment shows immediate stasis of the contrast material.
C, Angiogram obtained after coiling through the stent interstices shows that the aneurysm is subtotally occluded.
D, Further thrombosis is noted after 6 months.
A 46-year-old woman had a subarachnoid hemorrhage due to a cavernous (C3–4) aneurysm 2.5 years ago; clinically, she was Hunt and Hess grade 1, with complete recovery. Follow-up angiogram 2 years after treatment showed regrowth of the initially incompletely coiled aneurysm (Fig 4A). Because of enlargement of the residual aneurysm (aneurysm neck, 5 mm; dome, 4.5 mm) and because the patient insisted on treatment, we attempted endosaccular coil embolization, but different sizes and configurations of coils (two- and three-dimensional) did not remain within the aneurysm. We introduced a 4.5 × 20-mm self-expanding stent and deployed it over the aneurysm orifice, with immediate contrast material stasis in the residual sac (Fig 4B). In total, four detachable platinum coils (GDC 10 ultrasoft: 4/8, 3/8, 3/8, 3/6) were detached. The aneurysm was subtotally occluded (Fig 4C) and showed further thrombosis after 6 months (Fig 4D). The patient′s clinical status was unchanged during the entire follow-up period.
Case 3 (Fig 5).
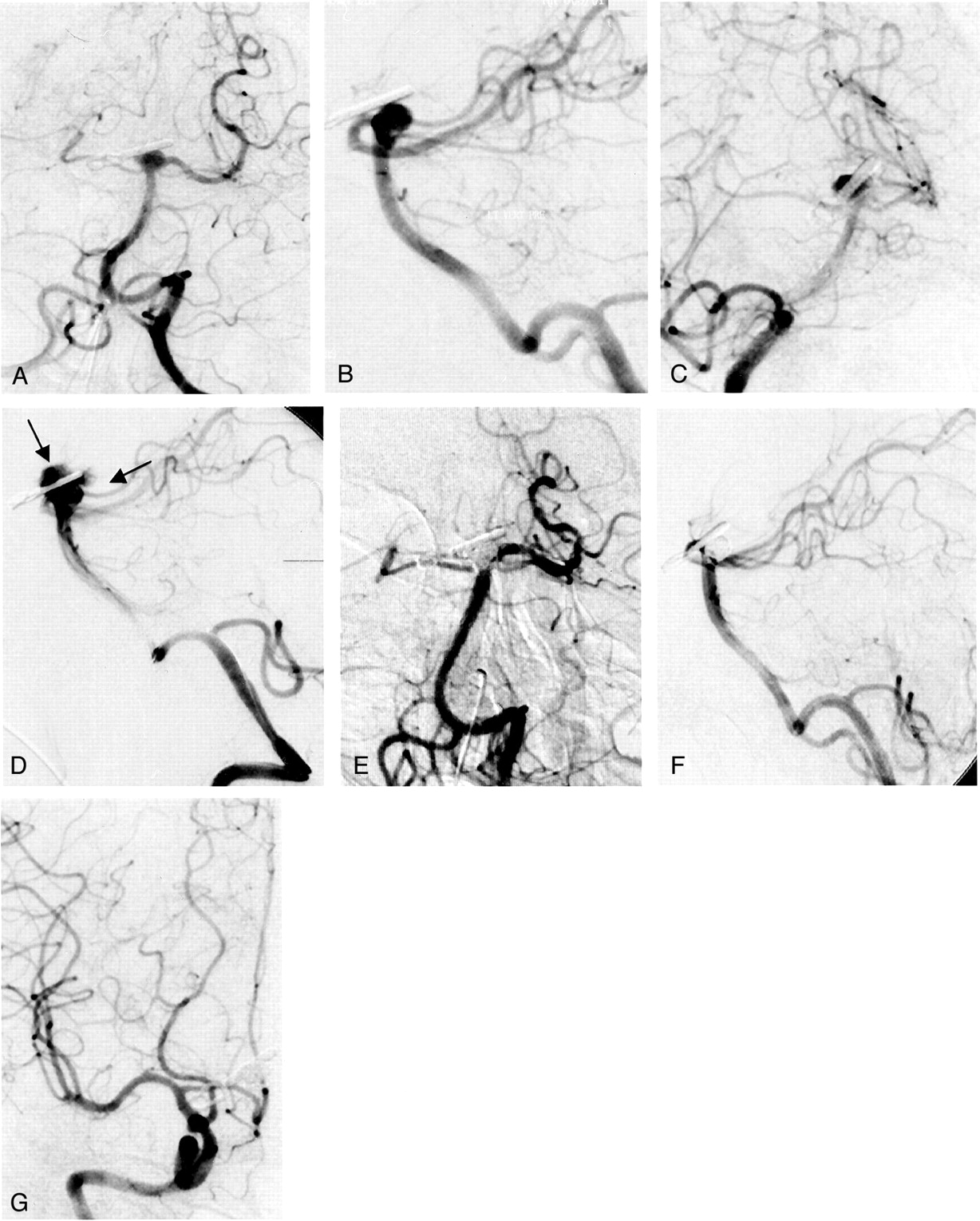
Case 3.
A, Anteroposterior and B, lateral DSA views demonstrate a broad-based, previously clipped, recurrent basilar tip aneurysm encroaching on the left P1 segment.
C, Angiogram reveals immediate stasis of contrast material in the aneurysm after stent deployment.
D, Angiogram reveals extravasation of contrast material after aneurysm perforation with the microcatheter (arrows).
E, Posteroanterior and F, lateral final angiograms after treatment show complete obliteration.
G, Angiogram shows that the right posterior cerebral artery is opacified via the internal carotid artery.
A 43-year-old woman had a basilar tip-P1 aneurysm clipped at an outside hospital 10 years previous, after presenting with symptoms of subarachnoid hemorrhage. She still had oculomotor palsy on the right. She recently presented with dizziness. Conventional angiography was recommended to exclude de novo aneurysms. DSA revealed a large recurrent aneurysm (Fig 5A and B) at the previously clipped basilar tip-P1 segment (dome width, 5.8 mm; neck length, 5.0 mm). Endosaccular coil embolization failed because of coil herniation into the parent vessel. Neurosurgical intervention was not considered because of previous clipping. Bridging of the aneurysm neck was achieved with a 3.5 × 20-mm self-expanding stent by positioning the stent from the left P1 segment to the distal basilar artery. Follow-up imaging with contrast material injection revealed immediate stasis of the contrast material in the aneurysm (Fig 5C). During navigation of the microcatheter through the interstices of the stent, the dome of the aneurysm was perforated with the microcatheter, probably because of increased tension within the system owing to the severely elongated vertebral artery. However, we cannot rule out that navigating the microcatheter through the stent struts needed an increased tension compared with a non-stent-covered aneurysm; thus, the perforation may have been related to the stent, at least in part. Although heart rate and blood pressure remained stable, contrast material extravasation was noted (Fig 5D). Heparin was reversed with protamine chloride, and immediate coiling of the aneurysm with complete obliteration (Fig 5E and F) was performed by using six detachable platinum coils (GDC 10: 5/8, 4/8, 4/8 ultrasoft, 3/8 ultrasoft, 3/8 ultrasoft, 2/6 ultrasoft). Contrast material extravasation stopped with insertion of the first coil. The right posterior cerebral artery was supplied via the right internal carotid artery (Fig 5G).
Postprocedure CT scan showed moderate extravasation of blood and contrast material into the subarachnoid space and slight dilatation of the ventricles. A ventricular drain was inserted from the left side immediately after the intervention; administration of low-dose heparin (15,000 U/day) was continued after surgery. Another CT scan after surgery revealed a left frontal hemorrhage along the ventriculostomy tract, with additional blood in the ventricles. At this point, the patient had a right hemiparesis. Besides the bleeding, MR imaging did show an artifact due to the clip at the basilar tip. Therefore, the stent could not be evaluated, but there was no evidence of infarction, specifically not in the brain stem. After 8 weeks of rehabilitation, the patient was doing well without any motor deficits, although slight memory dysfunction persisted 6 months after the intervention. The patient denied follow-up angiography.
Case 4 (Fig 6).

Case 4.
A, Posteroanterior and B, oblique DSA views show a previously coiled, multilobulated, recurrent basilar tip aneurysm encroaching the left P1 segment.
C, Unsubtracted image demonstrates the proximal and distal markers (arrows) of the self-expanding neurovascular stent positioned with the distal end in the left P1 segment and with the proximal end in the midbasilar artery.
D, Final oblique angiographic view after treatment demonstrates complete obliteration of the aneurysm.
E, Follow-up angiogram reveals that the aneurysm remained occluded 6 months later
A 47-year-old man had a subarachnoid hemorrhage (Hunt and Hess grade 1) due to rupture of a basilar tip aneurysm 4 years previously. The initial aneurysm of 3 mm was treated with endosaccular coil embolization, but only a single detachable coil could be introduced at that time (GDC 18: 3/4). The patient recovered completely, but the first follow-up angiogram 4 years after treatment showed recanalization with regrowth of the basilar tip aneurysm now incorporating the left P1 segment (dome width, 3.0 mm; neck length, 3.5 mm) (Fig 6A and B). A 3.5 × 20-mm self-expanding stent was deployed from the P1 segment into the distal basilar artery (Fig 6C). No stasis of contrast material was observed in the aneurysm lumen. Two detachable coils (GDC 10: 3/8, 2/4) were easily introduced without coil herniation into the parent artery, and complete obliteration of the aneurysm was achieved (Fig 6D). Postprocedural MR image was normal and revealed no stent artifacts, and the patient’s clinical status was unchanged. Despite the stent’s position with bridging pontine branches originating from the basilar artery, there was absolutely no evidence of any ischemic brain stem infarction. After 6 months, the aneurysm remained completely occluded (Fig 6E).
Results
Technical Aspects
In all patients, even when severe vessel tortuousity was present, the microdelivery stent system was easy to handle and introduce. The stent could be safely and accurately deployed at the desired location in every case. The wide neck of the aneurysm was accurately and completely covered in all patients. There were no difficulties in navigating the microcatheter through the interstices of the stent. However, owing to tension in the microcatheter system, aneurysm perforation with the microcatheter occurred in one patient.
Complete or nearly complete occlusion of the aneurysm was achieved in all four cases. However, when inserting small coils (diameter 2 mm), we saw that the loop can in part herniate back through the mesh. The loop can be easily repositioned before its detachment.
Clinical Aspects
No evidence of vessel thrombosis was noted within the 6-month observation period. One procedure-related complication occurred, with aneurysm perforation resulting in subarachnoid hemorrhage. It was difficult to determine whether this event was related to the extremely tortuous vertebral artery, which required an increased tension to navigate the microcatheter into the aneurysm, or to the stent itself, which might lead to an increased navigational pressure. Because of slight hydrocephalus, the patient required ventricular drainage, which led to intraparenchymal bleeding and right hemiparesis that resolved completely after 2 months. The patient′s condition was probably exacerbated by the strong antiplatelet regimen necessary to prevent stent thrombosis.
At 6-month follow-up evaluation, all patients did well without focal neurologic deficits. One patient (patient 3) had slight memory and concentration problems.
Imaging Findings
Although we did not really force attenuated packing, immediate angiographic results showed complete (patients 1, 3, and 4) and nearly complete (patient 2) occlusion of the aneurysm. Stent placement prevented coil herniation into the parent artery in all patients. No angiographic evidence of thrombosis of any vessel or stent migration was observed during the procedure.
In three of four patients, MR angiography allowed excellent visualization of the vessel with the stent, without any artifacts. In one patient, MR angiography was not diagnostic because of the previously clipped aneurysm at the basilar tip.
Discussion
In many intracranial aneurysms, endovascular filling of the aneurysmal lumen is feasible, specifically in those with a small neck. In those aneurysms with an unfavorable dome-to-neck-ratio or a wide neck, endosaccular embolization with preservation of the parent artery still remains a challenge for the neurointerventionalist.
To support coil deposition in wide-necked aneurysms, different coil designs and endovascular techniques have been developed. Moret et al (15) pioneered the neck-remodeling technique for aneurysms with a wide neck or unfavorable geometry. This adjunctive method requires simultaneous use of an additional microcatheter with a nondetachable balloon and consequently involves a higher level of technical complexity. Our search revealed only a few reports in the literature, and the number of treated aneurysms with this technique is fairly small (16–22). Complete aneurysm obliteration rates vary between 67% and 83%, and the technical failure rate, if mentioned, is up to 23%. This technology may produce a temporary increase of pressure within the aneurysm while occluding the aneurysmal neck during coil delivery. The sudden change of intraaneurysmal pressure may potentially be the cause of aneurysm rupture, which is reported in about 5% of cases with use of this technique.
Another treatment option for wide-necked aneurysms are three-dimensionally shaped coils. These coils have a omegalike memory and thus configure a basket for subsequent coils (23, 24). In our experience, these coils do not work well in small aneurysms and do not always allow attenuated packing down to the base without risk of coil protrusion into the parent vessel.
The combination of bridging the aneurysm neck with a stent and subsequent coiling through the stent interstices provides another treatment alternative. Our literature search found only a few reports about this technique published so far (6–13). Most authors deployed coronary stents in proximal intracranial segments of the internal carotid artery, the vertebral artery, or the basilar trunk.
In our series, we used a self-expanding, highly flexible stent system that, even in curved vessels, conformed to the endoluminal contour without straightening the parent artery. Even when the stent bridged very tiny vessels, like pontine branches originating from the basilar artery, we did not observe any ischemic event in these vascular supply areas. In all patients, the stent prevented coil herniation into the parent vessel.
Although the mesh of the stent is hardly visible under fluoroscopy, the platinum markers at the distal and proximal ends enable sufficient visualization to position the stent properly. Because there is no superimposition by a metallic stent mesh, deployment of the coils could easily be seen.
The major advantage of this stent is its self-expanding character, allowing deployment without balloon assistance, and its distinctively characteristic flexibility.
In three of the four patients in our study, we observed immediate stasis of the contrast material in the aneurysmal sac, probably due to flow alterations at the inflow zone. These hemodynamic alterations may promote thrombosis within the aneurysm, even without subsequent coiling. However, antiplatelet therapy may result not only in significant reduction of stent thrombosis, but also in reduced thrombus formation in the aneurysmal sac. Therefore, coiling was considered to be an effective and necessary therapeutic adjunct in these patients. The single major complication we had was intracerebral bleeding after ventricular shunt surgery. Anticoagulation with heparin and aspirin alone can be reversed to a reasonable amount by using protamine chloride and minirin. However, the additional treatment with modern antiplatelets like clopidogrel or ticlopidine cannot be reversed and may cause severe problems if subsequent surgery is necessary. The results from a comparative study, after stent implantation in coronary vessels, evaluating aspirin alone versus combined ticlopidine and aspirin did not show significant differences in stent thrombosis or other adverse clinical outcomes between the two groups (25). Anticoagulation, therefore, should be a focus of ongoing research on this new type of therapy. If there is any evidence that the patient will need ventricular shunt surgery because of the subarachnoid hemorrhage, this should be done before interventional therapy. On the basis of our experience, this might not only prevent fatal increase of intracranial pressure in all cases of intraprocedural aneurysm rupture, but might also reduce subsequent bleeding complications if the patient is on a strong anticoagulation regimen.
In our small series, the self-expanding stent did not cause any artifacts on MR images and MR angiograms. Therefore, these imaging techniques can be used, as in patients treated with coils alone, for follow-up imaging. Longer follow-up and a larger group of patients are needed to establish the true efficacy of the Neuroform microdelivery stent system in treating wide-necked intracranial aneurysms.
This new generation of extremely flexible, self-expanding neurovascular stents and the use of the described technique may initiate the next step of endovascular management of intracranial aneurysms. Nevertheless, we underline that this treatment option should be reserved for patients without other options, because we do not have adequate basic science or controlled clinical information to support the routine use of stents in intracranial vessels. The treatment risk of increased morbidity due to a higher probability of aneurysmal perforation and a higher probability of intracerebral bleeding, if subsequent surgery is necessary, seems to be increased, at least during the initial learning curve.
Conclusion
Our preliminary data reveal that this self-expanding stent designed for intracranial vessels is technically easy to deploy and can be easily, accurately, and safely maneuvered even through severely tortuous vessels, enabling the treatment of wide-necked aneurysms. The combination of endovascular reconstruction of the parent vessel by using a neurovascular stent followed by coil embolization offers a promising therapeutic alternative in the treatment of wide-necked aneurysms not amenable to coil embolization alone. Although immediate angiographic results are promising, long-term angiographic and clinical follow-up is essential to determine parent vessel patency and aneurysm occlusion rate.
References
- Received November 5, 2002.
- Accepted after revision January 13, 2003.
- Accepted after revision January 13, 2003.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Wide-neck bifurcation aneurysms of the middle cerebral artery and basilar apex treated by endovascular techniques: a multicentre, core lab adjudicated study evaluating safety and durability of occlusion (BRANCH)
- Endovascular treatment of complex intracranial aneurysms using Acandis Acclino stents
- Stent-Assisted Coiling of Wide-Neck Intracranial Aneurysms Using Low-Profile LEO Baby Stents: Initial and Midterm Results
- Dual Stenting Using Low-Profile LEO Baby Stents for the Endovascular Management of Challenging Intracranial Aneurysms
- Safety and Efficacy of Neuroform for Treatment of Intracranial Aneurysms: A Prospective, Consecutive, French Multicentric Study
- Treatment of basilar tip aneurysms with horizontal PCA to PCA stent-assisted coiling: case series
- Stent assisted coiling of the ruptured wide necked intracranial aneurysm
- Stent-Assisted Coiling of Complex Middle Cerebral Artery Aneurysms: Initial and Midterm Results
- Bailout Stent Deployment during Coil Embolization of Intracranial Aneurysms
- Stent Conformity in Curved Vascular Models with Simulated Aneurysm Necks Using Flat-Panel CT: An In Vitro Study
- Interventional Neuroradiology