
Abstract
BACKGROUND AND PURPOSE: In patients with epidural lipomatosis, axial lumbar spine CT and MR images occasionally reveal a geometric, polygonal or stellar, shape of the dural sac. The purpose of this study was to define the anatomic structures responsible for this radiologic appearance. We hypothesized that meningovertebral ligaments could anchor the dura mater to the osteofibrous walls of the spinal canal and account for the geometric deformation of the dural sac.
METHODS: The epidural spaces were examined in 15 adult cadaveric and seven aborted fetal lumbar spines. For macroscopic studies, 70 adult vertebral segments were separated and dissected by removing the extradural fat. For microscopic examination, axial histologic sections were obtained from 35 fetal and five adult undissected vertebral segments.
RESULTS: Meningovertebral ligaments were observed in the median, paramedian, and lateral aspects of the anterior and posterior epidural spaces of both adult and fetal lumbar spines. These ligaments anchor the outer surface of the dura mater to the osteofibrous walls of the lumbar canal. They may form an irregular longitudinal septum partitioning the epidural space. Histologic examination demonstrated the fibroelastic composition of these ligaments and suggested their possible perivascular morphogenetic origin.
CONCLUSION: The morphologic and topographic features of the meningovertebral ligaments explain the polygonal, stellar, or Y-shaped deformation of the dural sac observed on axial CT and MR images in patients with lumbar epidural lipomatosis.
Epidural lipomatosis, which is a rare complication of chronic corticosteroid therapy or endogenous Cushing syndrome, is characterized by the abnormal accumulation of unencapsulated adipose tissue in the extradural space (1, 2). Idiopathic cases also have been described, occurring most frequently in obese patients (3). Clinical manifestation depends on disease severity and vertebral level. Patients with involvement of the lumbosacral spine may either be asymptomatic or present radicular symptoms or neurogenic claudication.
Since fat has a characteristic low attenuation on CT images and a high signal intensity on T1-weighted MR images, both modalities enable detection of increased proportion of extradural fat (4). When examining axial CT and MR images of the lumbar spine in patients with epidural lipomatosis, we frequently observed a polygonal spiculated, Y-shaped, or stellar deformation of the dural sac in association with epidural fat overgrowth. Although this geometric appearance had already been reported in the radiologic literature (5), we found no anatomic explanation for it (6–9).
Such a geometric dural deformation could be explained hypothetically by the presence of structures connecting and anchoring the outer surface of the dura mater to the osteofibrous walls of the lumbar spinal canal. Although meningovertebral ligaments have been described in the anterior and lateral lumbar epidural spaces (7, 10–13), such ligaments have not been reported in the posterior lumbar epidural space.
The aims of this study were to find the explanation of the dural sac deformation observed on axial MR images in patients with lumbar epidural lipomatosis, to confirm the existence of anterior meningovertebral ligaments and assess the hypothetic presence of similar ligaments in the posterior lumbar epidural space, and to describe the morphologic features of these ligaments.
Methods
Imaging Studies and Observations
During a 2-year period (January 1999–January 2001), CT and MR images of the lumbar spine that showed dural sac deformation in relation to epidural lipomatosis were prospectively collected in the department of radiology and medical imaging at our institution. Inclusion criteria were the presence of dural sac deformation with a polygonal (hexagonal or pentagonal), stellar, or Y-shaped sac due to the presence of unusually abundant epidural fat, seen at at least one spinal segment. Other causes of dural sac deformation were excluded (ie, discal or osseous causes).
CT examinations were performed on a dual-detector CT unit (Twin RTS; Marconi Medical Systems, Cleveland, OH) by using either a sequential acquisition mode (2.5-mm contiguous sections) or a spiral scanning mode (native section thickness, 2.7 mm; pitch, 0.7).
MR examinations consisted of T1-weighted spin-echo and T2-weighted fast spin-echo MR images obtained in the sagittal (lower thoracic and lumbosacral spine) and axial (last three lumbar disks) planes on a 1.5-T unit (Gyroscan NT; Philips Medical Systems, Best, the Netherlands or Signa; GE Medical Systems, Milwaukee, WI). Sagittal T1-weighted MR images were obtained by using the following parameters: 400–500/12–20 (TR/TE), 359 × 512 matrix, 2–4 signals averaged, nine sections, 4-mm thickness, 0.4-mm intersection gap, and 300 × 200 field of view. Sagittal T2-weighted fast spin-echo MR images were obtained with the same parameters except for 4000–5000/112–120, echo train length of 8–12. Axial T1- and T2-weighted MR images of the L3–4, L4–5, and L5-S1 levels were obtained with the same parameters except for 192 × 512 matrix and 300 × 200 field of view.
Anatomic Study
The lumbar spines of 14 embalmed adult cadavers (eight male and six female; age range, 62–95 years; mean age, 78 years) were collected. The 70 vertebral segments were separated from each other by transecting the corresponding intervertebral disks and dural sac with a saw cut and by opening the zygapophyseal joints. The global shape of the dural sac was then noted and rated as being either polygonal (hexagonal, pentagonal, or square), or triangular or Y-shaped. Later, the extradural fat was cautiously removed with small forceps to respect nonfat tissue. Finally, the presence and location of meningovertebral ligaments within these spaces were recorded, and each segment was photographed.
Microscopic Study
Lumbar spine specimens were obtained from seven aborted fetuses (three male and four female), aged 11, 27, 30, 31, 33, 35, and 38 weeks, and from an embalmed 63-year-old male cadaver. The vertebral segments were individualized in the same way as in the adult spines for the anatomic study. The 40 vertebral segments were fixed in formalin for 5 days. Transverse, 5-μm-thick sections of each segment were obtained after decalcification in formic acid (1%) and inclusion in paraffin. Of the four sections examined per vertebral level, three were stained with Goldner trichrome to color collagen fibers and the fourth with orcein to highlight elastic fibers.
Immunohistochemistry with anticollagen type I antibodies (dilution 1:500, Chemicon, Temecula, CA) was also performed on one adult and two fetal vertebral sections.
Results
Imaging Studies
During the 2-year study period, epidural lipomatosis with geometric dural sac deformation was noted in 13 (0.8%) of 1642 CT examinations (Figs 1 and 2) and in 13 (1.2%) of 1097 MR examinations (Figs 3 and 4). This deformation was categorized as illustrated in Table 1.
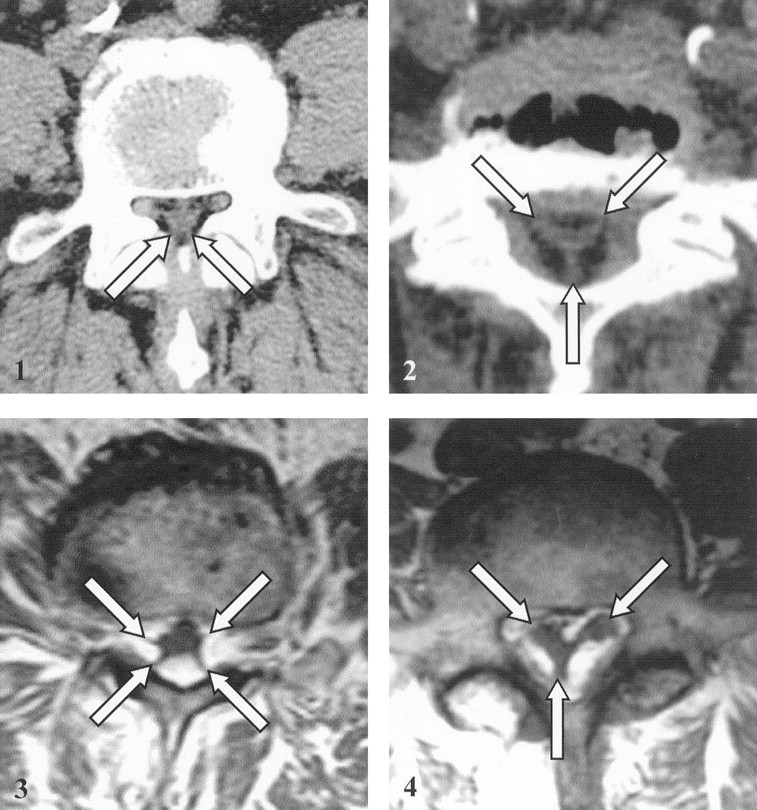
Axial CT scan at the L5 level in a 60-year-old patient with epidural lipomatosis shows low-attenuation fat surrounding the dural sac in the spinal canal; the sac shows polygonal deformation with spiculated contours (arrows).

Axial CT scan at the L5-Sl level in a 66-year-old patient with epidural lipomatosis shows low-attenuation fat surrounding the dural sac in the spinal canal; the sac shows Y-shaped or inverted triangular deformation (arrows). Disk bulge (anteriorly) and ligamenta flava (posterolaterally) lie peripheral to the fat.

MR imaging appearance of epidural lipomatosis in a 70-year-old patient. Axial T1-weighted MR image at the L4 level shows high-signal-intensity fat surrounding the dural sac in the spinal canal; the sac shows polygonal (stellar) deformation with spiculated contours (arrows).

MR imaging appearance of epidural lipomatosis in another 66-year-old patient. Axial T1-weighted MR image at the L5-S1 level shows high-signal-intensity fat surrounding the dural sac in the spinal canal; the sac shows Y-shaped or triangular deformation (arrows).
Variations of dural sac shape as seen on axial CT or MR images of the lumbar spine in 26 patients with epidural lipomatosis
Anatomic Study
Meningovertebral Ligaments
These ligaments were observed in each of the 70 adult lumbar vertebral segments, with topographic variations from one subject and level to another.
In the anterior epidural space, these ligaments appeared as thin connective bands that anchor the outer surface of the dura mater to the periosteum of the posterior wall of the vertebral body, to the posterior longitudinal ligament, or to the internal aspect of the pedicles. These fibrous bands usually showed a grossly sagittal or sagittal-oblique orientation and, depending on their insertions, were located in the median, paramedian, or lateral areas of the anterior epidural space, on one or both sides (Fig 5).

Macroscopic study in an adult spine.
A-C, Transverse sections of the lumbar spinal canal show median (arrow in A), bilateral paramedian (arrows in B), and lateral (arrows in C) locations of the meningovertebral ligaments in the anterior epidural space. The thecal sac (S) is collapsed by drawing the dura mater posteriorly with a thread.
In the posterior epidural space, similar meningovertebral ligaments also extended from the outer surface of the dura mater to the vertebral laminae and to the ligamenta flava. According to their insertions, they were located in the median, paramedian, or lateral areas of the posterior epidural space (Fig 6).

Macroscopic study in an adult spine. Transverse sections of the lumbar spinal canal show different locations of the meningovertebral ligaments in the posterior epidural space.
A, Paramedian (arrow) and median (arrowhead) locations of meningovertebral ligaments. The thecal sac (S) is collapsed by drawing the dura mater forward with a thread.
B and C, Paramedian (arrow) and lateral (arrowheads) locations of meningovertebral ligaments. The thecal sac (S) is collapsed centrally.
In the lateral epidural space, similar thin fibrous structures were observed, anchoring the lateral outer surface of the dural sac to the contours of the intervertebral foramina (Fig 7).

Macroscopic study in an adult spine shows lateral location (arrow) of meningovertebral ligaments in the lateral epidural space (the dura mater is drawn laterally).
The frequencies of the meningovertebral ligaments are illustrated in Fig 8, according to their location in the 70 adult vertebral levels. By convention, the meningovertebral ligaments were listed at 12 different locations corresponding to the 12 rays of a clock quadrant. Median anterior and posterior ligaments were located in the sagittal midplane, whereas those of the lateral epidural space were situated in the frontal plane. Finally, the paramedian and lateral ligaments of the anterior and posterior epidural space were placed between these two perpendiculars. None of the positions was absolutely consistent. First, in the median location, meningovertebral ligaments were most frequent in the anterior epidural space with 47% of the observations, to 17% in the posterior space. The paramedian location was the most represented, in both anterior and posterior epidural spaces, concerning, respectively, about 90% and 40% of the vertebrae. Last, the lateral position was observed in nearly half of the anterior epidural space and in one-fourth of the posterior one. In the lateral epidural space, meningovertebral ligaments were present in one of four vertebrae (Fig 8).
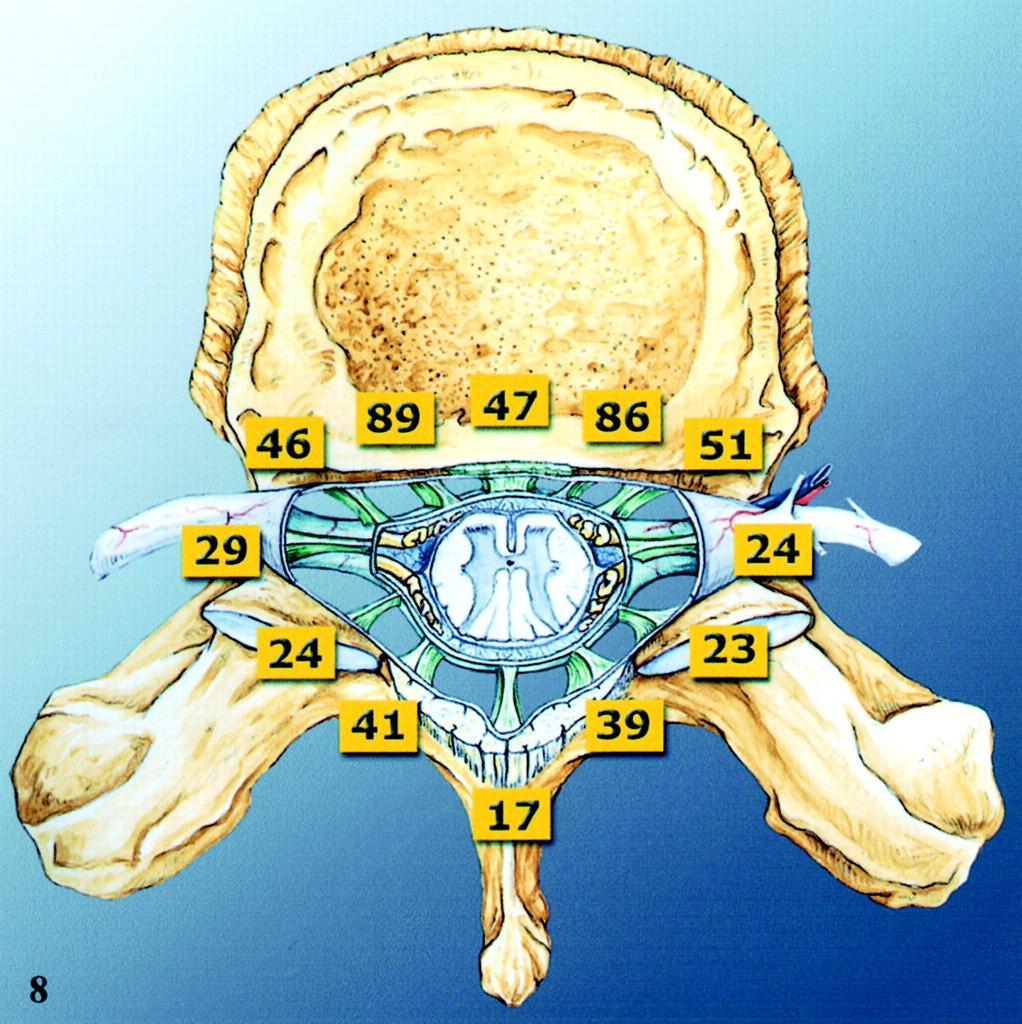
Distribution of the meningovertebral ligaments in the transverse plane in the 70 adult dissected lumbar vertebrae, with corresponding frequencies (numbers are percentages).
When compared in adjacent spinal levels, meningovertebral ligaments sometimes were observed at the same location. This extension from one segment to the other suggests that meningovertebral ligaments represented an irregular and discontinuous, grossly longitudinal septum leading to partial partitioning of the epidural space.
Shape of the Dural Sac
When analyzed before epidural fat dissection, the shape of the dural sac showed changes in the successive transverse sections of the lumbar spine. It was most often polygonal (hexagonal or pentagonal) in the upper lumbar spine, whereas it progressively showed an inverted triangular or Y shape in the lower spine (Table 2).
Variations of dural sac shape as seen on macroscopic photographs of 70 dissected adult lumbar spine segments
Microscopic Study
Histologic examination of the fetal and adult spinal levels showed that the meningovertebral ligaments are mainly composed of dense connective tissue, mixed with elastic fibers, and surrounded by fat lobules (Figs 9 and 10). Specific immunohistochemistry demonstrated that their major component consisted of collagen type I fibrils (Fig 9B and C). These ligaments were in continuity with the most external fibroelastic layers of the dura mater, at one of their extremities, and with the osteofibrous walls of the spinal canal, on their other end (Fig 9). Laterally, they were connected with the medial aspect of the epineurium of the spinal nerves.

Microscopic study in a 27-week fetal spine shows relation of meningovertebral ligaments to dura mater and to spinal canal walls.
A, Photomicrograph (Goldner trichrome stain; original magnification, ×12) of a fetal spinal canal at the L1 level. Meningovertebral ligaments extend from the outer surface of the dura mater to the osteofibrous walls of the spinal canal in the lateral areas, representing perivascular bands (arrowheads), and in the median area of the posterior epidural space (arrow). The large box outlines the region of the epidural space that is magnified in B. The small box outlines the region that is magnified in C.
B, Magnified view (immunohistochemical stain for type I collagen) of the large box in A. The meningovertebral ligament anchors the dura mater (curved arrow) to the spinal canal (arrow) and surrounds small vascular structures (arrowhead).
C, Magnified view (immunohistochemical stain for type I collagen) of the small box in A. The meningovertebral ligament (arrowhead), mainly composed of type I collagen, is connected to the outer surface of the dura mater (arrow).

Microscopic study of meningovertebral ligament content in fetal spine. Photomicrograph (Goldner trichrome stain; original magnification, ×20) at the L1 level of a 27-week fetal spinal canal. The meningovertebral ligament (arrowhead) contains small vessels (arrow) (same observation as in adult spine in Fig 11).
In the spine of the 11-week-old fetus, meningovertebral ligaments were already present, though much thinner than those in the adult. They were surrounded by large amounts of mesenchymal cells, which filled the epidural space. These cells were absent and replaced by epidural fat in older fetuses. Small vascular structures were also observed in some meningovertebral ligaments (Fig 10).
In the adult spine, the ligaments remained connected to the dural sac and to the osteofibrous walls of the vertebral canal (Fig 11). They appeared somewhat thicker than in the fetal spines, and also contained occasionally small vascular structures (Fig 11).
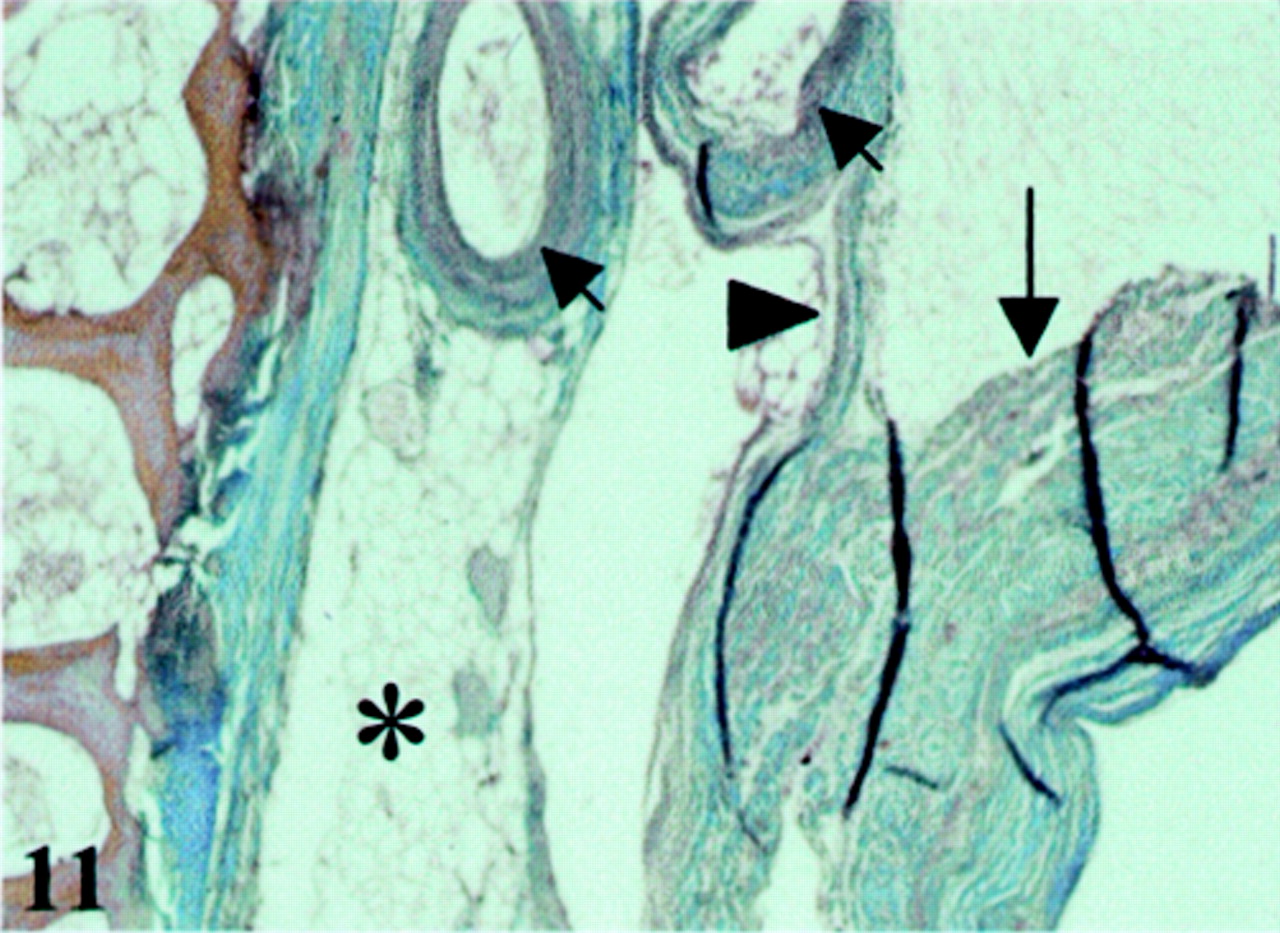
Microscopic study at the L3 level of an adult spinal canal. Photomicrograph (Goldner trichrome stain; original magnification, ×20) shows that the meningovertebral ligament (arrowhead) is connected to the dura mater (long arrow) and contains epidural vessels (short arrows); loose fat is present in the lateral area of the posterior epidural space (asterisk).
Discussion
This study was designed to find the explanation for the deformation of the dural sac seen on axial CT and MR images in patients with epidural lipomatosis. During a 2-year study, this anomaly was observed in approximately 1% of patients undergoing lumbar spine CT or MR examinations. Our results can be summarized as follows. First, our anatomic and histologic studies of fetal and adult spines confirm that meningovertebral ligaments are present in the anterior epidural space (Fig 5), as previously described (10, 11, 13). Second, our data show that similar ligaments also exist in the posterior lumbar epidural space (Fig 6). The frequency of this observation conflicts with anatomic descriptions (6–8) and with a recent histologic study of the posterior epidural fat in which the authors concluded that there was an absence of posterior anchoring of the dura mater (9). This discrepancy can be explained by a major difference in dissection techniques. Indeed, the opening of the lumbar canal by section of the pedicles and the posterior epidural fat removal before histologic study could damage the posterior meningovertebral ligaments (9). In our study, the segments of the spine were processed for histologic examination without previous dissection or manipulation.
The anatomic and topographic features of meningovertebral ligaments observed in this study parallel the deformations of the dural sac seen on serial axial CT and MR images obtained in patients with lumbar epidural lipomatosis (Figs 1–4). The thecal sac was collapsed because of posterior (Fig 5) or anterior (Fig 6) drawing of the dura mater. This explains the differences between the images and the anatomic sections. We believe that the “spiculations” of polygonal sections or star branches correspond to the dural insertion site of the ligaments, and that the intervening depressions correspond to the mass effect of the excessive epidural fat in these patients. The variations in geometric shapes most likely result from the inconsistent and random distribution of these ligaments.
We observed variations of the shape of the dural sac along the lumbar spine. In both the imaging and anatomic studies, sac shape was generally polygonal in the upper levels and tended progressively to be inverted triangular with a dorsomedian apex in the lower ones (Tables 1 and 2). The same trend had already been noted at epidurography (14–16) or in anatomic preparations after injecting polyester resin into the epidural space (17). The presence of median, paramedian, and lateral meningovertebral ligaments most likely explains the hexagonal, pentagonal, or square shape of the dural sac found in the upper and middle lumbar spine. The inverted triangular or Y shape observed in the lower lumbar segments probably results from several factors: the nerve roots originating from the sac on its anterolateral aspects and the filum terminale on its posterior aspect could contribute to this shape. Moreover, a median meningovertebral ligament can be responsible for the posterior “spiculation” of the dural sac. This posterior spiculation likely corresponds to the posteromedian fold of the dura mater visible at lumbar epidurography or epiduroscopy, which was called “plica mediana dorsalis” and interpreted as the consequence of the presence of a posterior connective tissue band extending from the dura mater to the ligamenta flava or to the laminae (15, 16, 18–22). From our anatomic observations, this posterior connective tissue can be considered a median meningovertebral ligament.
Although they do not connect articular structures, the anatomic term “ligament” seems to be most appropriate to characterize these thin but resistant fibroelastic bands extending from the outer surface of the dura mater to the osteofibrous walls of the spinal canal. This terminology appears adequate because of their dense connective nature and because of their presumed function of attachment of the dural sac to the neighboring structures. They should be considered loose ligaments, similar to pericardial, abdominal, or pelvic visceral ligaments or to the retinacular ligaments of the fingers, which all share the same characteristic feature of connecting soft tissues at the periphery of various organs to adjacent skeletal surfaces.
Chronologically, thin meningovertebral ligaments were already present at the 11th week of gestation and were then surrounded by large amounts of mesenchymal cells. During fetal growth, these surrounding cells are progressively replaced by epidural fat. Since the vertebral canal is enlarging, the small connective bands extending between the dural sac and the vertebral canal are progressively stretched out along axial spinal blood vessels (Figs 9 and 10). The morphogenetic phenomenon leading to development of the meningovertebral ligaments seems to be randomly distributed in the epidural space, and their definitive location in the adult vertebral canal varies according to both the subject and the vertebral level (Fig 8).
The occasional observation of the same location of meningovertebral ligaments in adjacent spinal segments suggests the possibility of a localized continuity between these ligaments, resulting in a partial and randomly distributed partitioning of the epidural spaces, and especially of the posterior epidural space. This compartmentalization might explain occasional problems in epidural anesthesia, such as inhomogeneous spread of the injected anesthetic drugs (14, 17, 19), failure of catheter introduction, or deviation of the ascending guide that stumbles over resistant connective bands, leading to final lateral positioning of the catheter (20, 23). Excessive manipulations of this latter may then give rise to accidental dural leakage or epidural hemorrhage (21) by injury of the epidural vessels running in close anatomic relationship with the ligaments (Figs 10 and 11).
The observation of meningovertebral ligaments in fetal spines and their histologic similarity with adult meningovertebral ligaments definitively strengthen their native origin.
Conclusion
The results of this study show that meningovertebral ligaments are present in all subjects, in both the anterior and posterior epidural spaces. These ligaments, invisible on imaging studies of subjects with normal spines, become evident to the radiologist’s eye in patients with epidural lipomatosis, when epidural fat overgrowth incidentally reveals their presence by indentations of the dural sac, alternating with intervening depressions due to mass effect of the excessive fat.
Footnotes
Presented in part at the 28th meeting of the French Society of Neuroradiology, Brussels, Belgium, 2000, and at the 12th European Anatomical Congress, Lyon, France, 2001.
References
- Received January 16, 2003.
- Accepted after revision February 18, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Differentiation between Tuberculous and Pyogenic Spondylodiscitis: The Role of the Anterior Meningovertebral Ligament in Patients with Anterior Epidural Abscess
- Immediate Pain Response to Interlaminar Lumbar Epidural Steroid Administration: Response Characteristics and Effects of Anesthetic Concentration
- Acute spinal cord compression