
We read with interest the article by Robson et al on CT and MR findings in nontuberculous mycobacterial infections of the head and neck in immunocompetent children (1).
The authors suggest that adenitis caused by nontuberculous mycobacteria (NTM) has a typical imaging appearance and may be characterized by an asymmetric cervical lymphadenopathy with minimal inflammatory stranding of the subcutaneous fat and lack of surrounding inflammation and that these criteria may help to distinguish adenitis caused by NTM from staphylococcal and streptococcal adenitis (1, 2).
Having had experience with a case of NTM infection of the head in an immunocompetent adult, we felt obliged to report our own observation to show that strong inflammatory stranding of the subcutaneous fat with surrounding inflammation may also occur in NTM lymphadenitis and does not per se help to differentiate NTM adenitis from bacterial lymphadenitis (Fig 1).
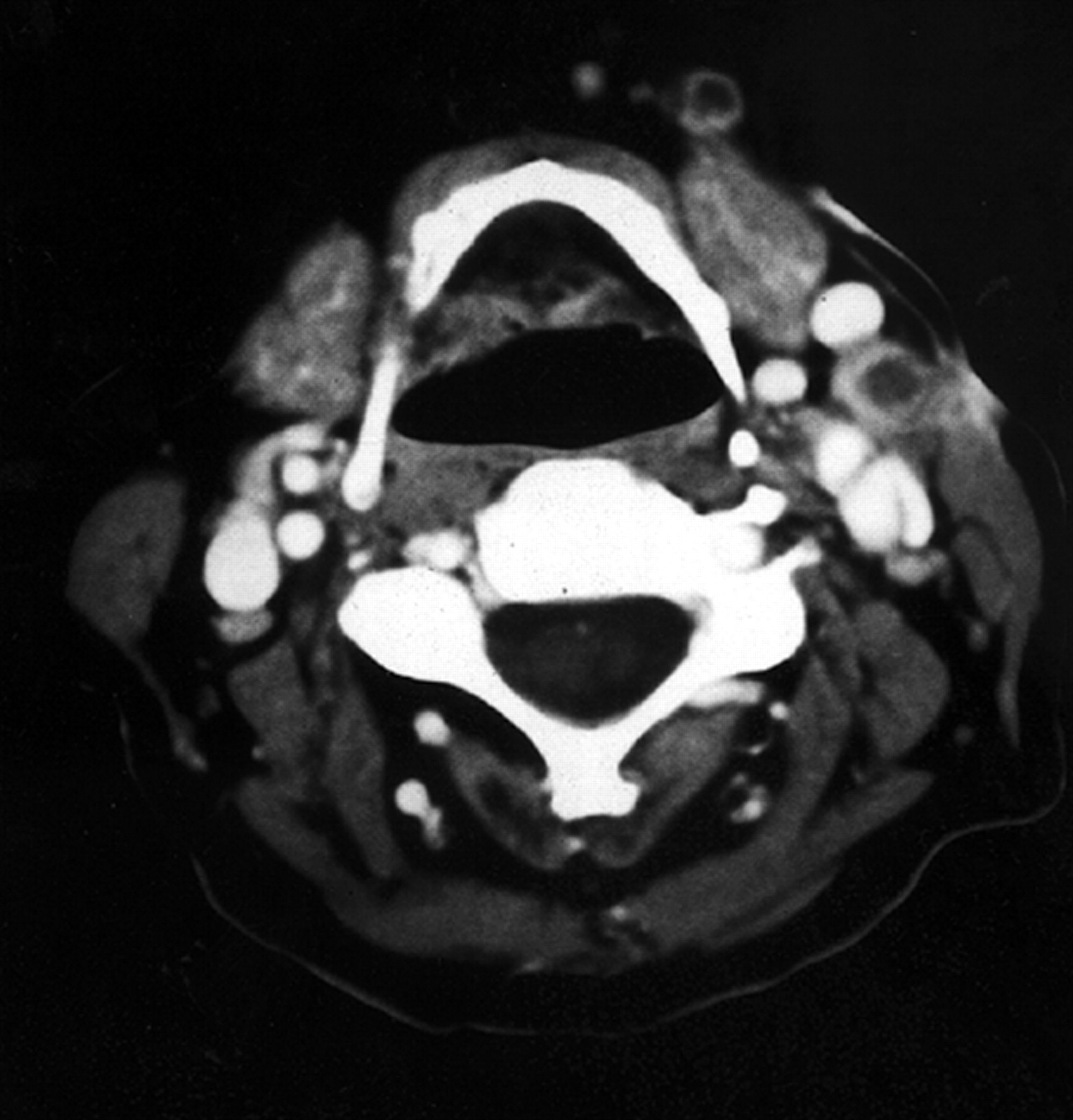
A 61-year-old immunocompetent woman presented with a painful tenderness of the submandibular region. On clinical examination, she had generalized lymphadenopathy with a cervical abscess at the left. A CT scan of the neck showed multiple cervical lymph nodes with ring enhancement, central necrosis, and an abscess with diffuse strong edematous infiltration of adjacent skin structures; no calcification within the involved lymph nodes was seen.
Surgical resection was only partially possible because of adherences of inflamed lymph nodes to the arteria carotis. Histopathologic analysis of the biopsy specimen obtained from the partial resection of a cervical lymph node revealed a necrotizing granulomatous lymphadenitis. Appropriate cultures (BACTEC method; Becton Dickinson Diagnostic Systems) of the biopsy yielded mycobacterium avium/mycobacterium intracellulare complex, thus confirming the rare case of a cervical NTM lymphadenitis in an immunocompetent adult patient (3). Triple oral antibiotic treatment with clarithromycin, rifabutin, and ethambutol was started, but cervical lymphadenitis was complicated by longstanding formation of fistulas, and the clinical symptoms regressed only after 12 months of antimycobacterial chemotherapy. No new lesions occurred within the next 2 years.
To conclude, the present case demonstrates that the extension of the inflammatory stranding and surrounding inflammation in CT imaging does not (at least in adults) reliably differentiate NTM adenitis from bacterial lymphadenitis. Therefore, we emphasize the possibility of confirming the exact radiologic diagnosis by precise bacteriologic evaluation of the case.

CT scan of the neck shows multiple cervical lymph nodes with ring enhancement, central necrosis, and an abscess with diffuse strong edematous infiltration of adjacent subcutaneous fat involving the skin
Reply:
We read with interest the letter by Drs. Hanck, Katz, and Fleisch. We agree that stranding of the subcutaneous fat can occur in NTM infection (Fig 1). In our series of 12 immunocompetent children with NTM infection, one child had moderate stranding of the subcutaneous fat (1). It is interesting that this patient had the shortest duration of history. The CT appearance of a heterogeneous nodal mass with minimal or absent stranding of the subcutaneous tissues and extrusion of necrotic material toward or into the skin should suggest a diagnosis of NTM infection. However, the presence of stranding of the subcutaneous fat does not exclude NTM infection (2, 3). Stranding of the fat may to lead to a delay in diagnosis with an initial search for streptococcal, staphylococcal, or bartonella (cat scratch disease) infection. Over time, evolution of the imaging findings to a more characteristic appearance may be observed.
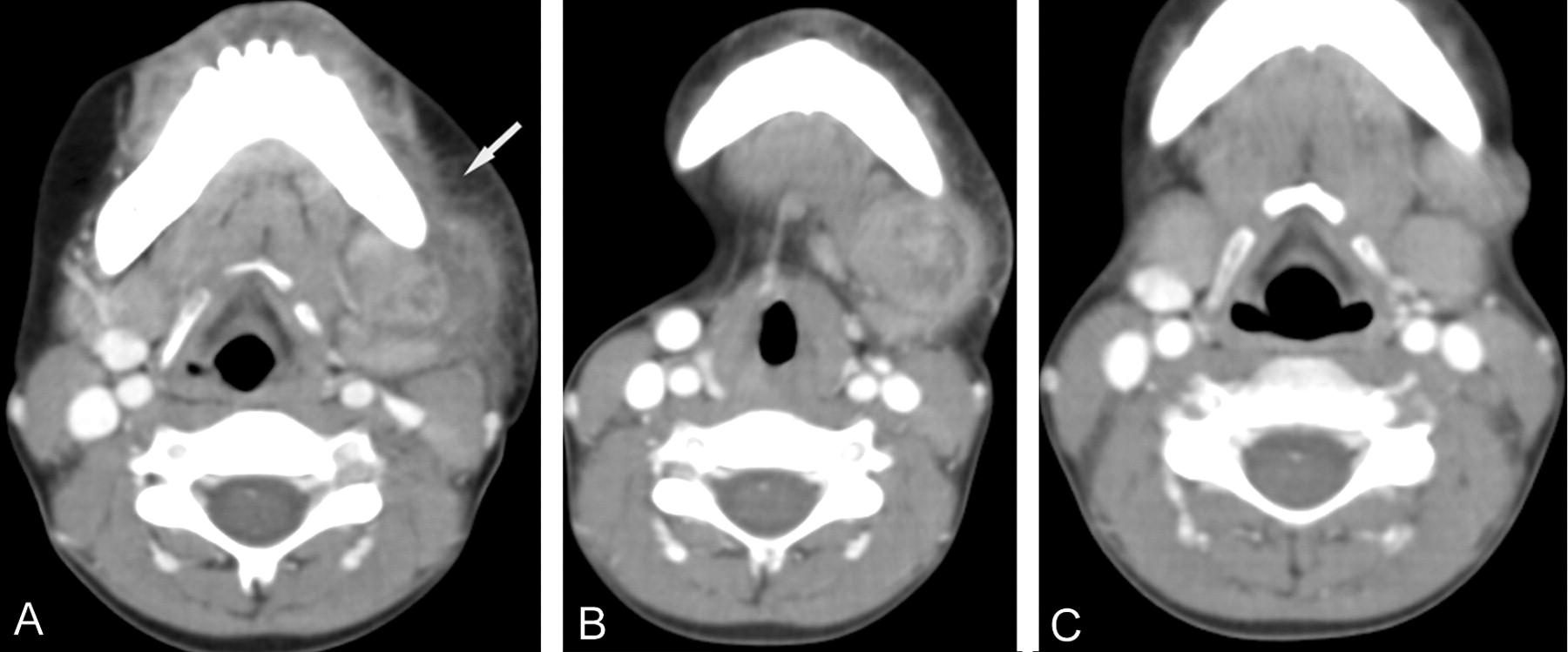
A case of an immunocompetent 5-year-old girl with a 5-week history of a neck mass.
A, Contrast-enhanced CT scan demonstrates heterogeneously enhancing left submandibular lymphadenopathy with adjacent phlegmonous changes and stranding of the subcutaneous fat (arrow).
B, Three weeks later, there is less stranding of the subcutaneous fat. Following curettage, a diagnosis of NTM infection was obtained.
C, Two months following curettage, and treatment with oral clarithromycin and ethambutol, the lesion has extended to the skin and decreased in size.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}