
Abstract
Summary: Basal cell adenoma is a rare benign salivary gland epithelial tumor, usually involving the parotid gland. We report CT and MR findings of three cases with basal cell adenoma occurring in the parotid gland. The three cases presented here demonstrate a well-circumscribed tumor, which showed a cystic and solid, or the pure solid mass. They were well enhanced after contrast matter injection. The solid portion of the mass was isoattenuated at CT, with intermediate signal intensity on T1- and T2-weighted MR images. Its cystic portion was hyperintense on both T1- and T2-weighted MR images. It had a hypointense rim on T2-weighted image.
Basal cell adenoma is an uncommon benign epithelial tumor of the salivary gland, accounting for 1–2% of all salivary gland epithelial tumors. More than 80% of basal cell adenomas arise in the major salivary gland, mostly the parotid gland. It is known to consist of a monomorphic population of basaloid epithelial cells, organized with a prominent basal cell layer and distinct basement membrane-like material; however, it lacks the myxochondroid stromal component, which distinguishes it from the pleomorphic adenoma (1–3). The imaging features of basal cell adenoma in the parotid gland have not previously been described with detail in the English language literature.
We report three cases of the basal cell adenoma and describe the CT and MR imaging appearance of this unusual tumor, which is based on three cases occurring in the parotid gland.
Case Reports
Case 1
A 59-year-old woman was admitted because of a palpable mass in the left parotid region. Physical examination revealed a mass measuring about 3 × 3 cm, which was hard, movable, and not tender.
A contrast-enhanced CT scan showed a well-defined and homogeneously well-enhanced mass occurring in the left parotid gland (Fig 1A). A fine needle aspiration biopsy obtained atypical epithelial cluster from parotid gland mass. On the 5th hospital day, the patient underwent left superficial parotidectomy, including the removal of the mass, with preservation of the facial nerve and its branches. The mass was located at the superficial lobe of the left parotid gland. Grossly, it revealed a 2.3 × 2.0 × 1.5-cm, irregular surfaced, firm, well-encapsulated mass, with well-circumscribed, pale brownish, homogeneous cut surface. It was adhered to the surrounding normal parenchyma of the parotid gland and soft tissue. Microscopic examination proved the mass to be a basal cell adenoma (Fig 1B).
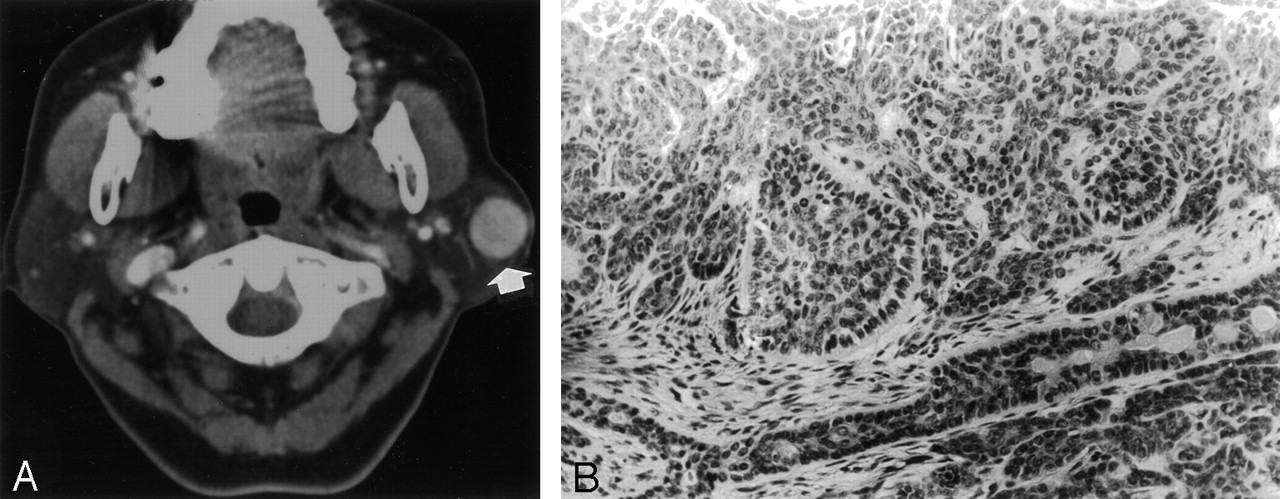
Case 1, a 59-year-old woman with a palpable mass in the left parotid region.
A, Contrast-enhanced axial CT scan shows a round, well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement.
B, Photomicrograph of the left parotid mass (hematoxylin-eosin stain; ×200) reveals trabecular cords in the tumor. Many small lumens that are lined by ductal or basaloid cells are evident within trabecular cords of basaloid cells. Peripheral nuclear palisades with thick basal lamina surround the nests.
Case 2
A 45-year-old woman was admitted because of a mass in the left parotid region of 1-year duration. On admission, the physical examination revealed a 3 × 4 cm soft, freely movable, nontender mass at the left parotid area.
CT showed a 2 × 2.2 × 3-cm cystic mass in the deep lobe of the left parotid gland. The mass was composed of mural nodules at its anterior and posterior portions, which was well enhanced. The wall of the cystic mass also showed slight enhancement. There was soft tissue attenuation in the left parapharyngeal space, which may have been an extension of the solid portion or leakage of inner content from the cystic portion (Fig 2A and B).

Case 2, a 45-year-old woman with a mass in the left parotid region.
A, Precontrast CT scan shows an isoattenuated mass with central low attenuation in the deep lobe of left parotid gland.
B, Postcontrast CT scan shows mass that is composed of well-enhanced peripheral mural solid nodule and central cystic component.
C, Axial T1-weighted (TR/TE, 500/27) MR image shows a well-defined cystic and solid mass in left parotid gland (arrow) with peripheral hypointense rim. The mass is composed of peripheral mural solid component of intermediate signal intensity to the muscle and central cystic component of high signal intensity.
D, Axial T2-weighted (TR/TE, 2500/80) MR image at the same level shows that the solid portion of the mass is still intermediate signal intensity to the muscle and its cystic portion shows high signal intensity.
E, Gross finding of the left parotid mass reveals a mass with large area of cystic change. There is peripheral, round, solid portion protruding into the lumen (arrow). A cystic portion is filled with brownish fluid. The cystic wall reveals yellow brown pigmentation along the wall, which is consistent with hemosiderin, microscopically.
F, Photomicrograph of the solid portion of left parotid mass shows epithelial nests and tubular structure composed of uniform cells with peripheral palisade (immunostaining for S-100 protein; ×100).
G, There were basaloid cells of the nest with thick hyaline basal laminas around the tumor nests on Periodic acid Schiff staining (magnification ×200). The histology is compatible with basal cell adenoma with cystic change.
MR imaging showed a 2 × 2 × 1.5-cm, well-marginated mass lesion at the medial portion of deep lobe of left parotid gland. The mass was a cystic and solid tumor with a thin fibrous capsule, composed of central cystic and peripheral soft-tissue components. The solid component was slightly hypointense/hyperintense compared with the muscle on T1- and T2-weighted images. The cystic contents of the mass were hyperintense on both T1- and T2-weighted images and proved to be hemorrhage (Fig 2C and D).
The patient underwent left total parotidectomy on the 2nd hospital day. The mass was located in the deep lobe of parotid gland and was firmly adhered to the posterior belly of left digastric muscle. Grossly, it was round, well demarcated, and relatively hard. On gross resection, a cystic mass contained a round solid lesion protruding into the lumen, filled with blood-tinged, brownish fluid (Fig 2E). Microscopically, the solid lesion showed epithelial nests and tubular structure composed of uniform cells with peripheral palisade. No mitosis was found. The histology was compatible with basal cell adenoma with cystic change (Figs 2F and G).
Case 3
A 49-year-old woman was admitted with the complaint of a 5-year history of a mass in the left infra-auricular area. Physical examination revealed a 3 × 2-cm firm, fixed, and nontender mass.
CT scans showed about 3 × 2 × 2.5-cm well-demarcated mass in the deep lobe of left parotid gland that protruded to the superficial lobe. The retromandibular vein was displaced anteriorly, and the carotid sheath was medially deviated by the mass. The left internal jugular vein was also slightly compressed by the mass. The mass was isoattenuated compared with the muscle on pre-enhanced scans and well enhanced on postenhanced images. No internal necrotic or cystic component was seen. There was no definite lymphadenopathy along the internal jugular or spinal accessory chain (Figs 3A and B).

Case 2, a 45-year-old woman with a mass in the left infraauricular area.
A, Precontrast CT scan shows a well-demarcated isoattenuated mass to the muscle in the deep lobe of left parotid gland.
B, Postcontrast CT scan shows that the mass is inhomogeneously well enhanced, not containing definite cystic or necrotic components.
C, Photomicrograph of the left parotid mass reveals that the tumor is composed of small uniform basaloid cells arranged in solid or trabecular pattern. The stroma is scanty. There is characteristic palisading in the peripheral portion of the tumor cell nests and sharp demarcation between neoplastic cells and stroma. The histologic features are consistent with basal cell adenoma rather than pleomorphic adenoma (hematoxylin-eosin stain; ×200).
D, Immunohistochemical staining for cytokeratin shows positive staining in the central portion of tumor cell nests than peripheral portion (cytokeratin; ×200).
E, Immunohistochemical staining for smooth muscle actin shows peripheral staining of the tumor, which is indicative of myoepithelial differentiation (smooth muscle actin; ×200).
Left total parotidectomy was performed on the 2nd hospital day. The mass was well encapsulated and attached to parotid tissue. The mass measured 3.5 × 3.0 × 2.0 cm in diameter. It showed a smooth and lobulated surface and homogeneously pale, yellowish appearance with minute foci of cystic areas. Gross resection showed a well-encapsulated tumor of the parotid gland. The tumor was composed of small uniform basaloid cells arranged in solid or trabecular pattern. The stroma was scanty. There was characteristic palisading in the peripheral portion of the tumor nests and sharp demarcation between the neoplastic cells and stroma. The histologic features were consistent with basal cell adenoma, rather than pleomorphic, adenoma (Fig 3C and E).
Discussion
Salivary gland neoplasms represent less than 3% of all tumors in the general population. Approximately 88% of salivary gland neoplasms are of epithelial origin, and benign adenomas account for 65.5% of salivary tumors. Basal cell adenoma accounts for 1–2% of all salivary gland epithelial tumors, and more than 80% of them arise in the major salivary glands, mostly the parotid gland, as in the cases presented here.
Basal cell adenomas arise almost exclusively in adults, with the average patient age being 57.7 years, more than a decade older than the average age of patients with pleomorphic adenoma. There is a 2:1 female predominance for most of basal cell adenoma.
Basal cell adenoma was classified as part of the category of monomorphic adenomas, which was first described and adequately documented as a distinct clinical and pathologic entity by Kleinsasser and Klein in 1967 (4). The adenoma was divided into pleomorphic adenoma and monomorphic adenoma. Basal cell adenoma was defined as a subtype of monomorphic adenoma. In 1991, the World Health Organization (WHO) separately classified basal cell adenoma and its malignant counterpart, basal cell adenocarcinoma, as well as canalicular adenoma. The concept of monomorphic adenoma as the opposite of pleomorphic adenoma was repudiated. Instead, every adenoma was equated with pleomorphic adenoma (3, 5–7). Basal cell adenoma, as defined by WHO, is a distinctive benign neoplasm composed of basaloid cells organized with a prominent basal cell layer and distinct basement membrane-like structure and no myxochondroid stromal component as seen in pleomorphic adenomas. Three cellular patterns occur: solid, trabecular-tubular, and membranous. The common clinical feature of basal cell adenoma is a slow-growing, asymptomatic, freely movable parotid mass, which is often observed in women >50 years of age.
Grossly, basal cell adenomas are round or oval in shape. They tend to be smaller than pleomorphic adenomas; most measure 3 cm or less in diameter. On cut section, they are typically uniform and solid, without necrosis. They can, however, occasionally be cystic. They have characteristic, numerous endothelial-lined vascular channels, in which small capillaries and venules are prominent within the microcystic areas of the adenoma. These vascular structures can cause intratumoral hemorrhage (1, 8). The membranous type is noteworthy in that it can be multifocal, with a multinodular growth pattern. In many cases, cystic formations containing mucinous fluid are present in the center of a tumor. This can explain why basal cell adenomas are well enhanced and why hemorrhagic components are found within the cystic portion.
On microscopic examination, basal cell adenomas are benign tumors composed of relatively basaloid cells, a conspicuous basal cell layer, and distinctive basement membrane-like material. Basal cell adenomas lack the characteristic myxochondroid matrix of pleomorphic adenoma. Most tumors are well circumscribed and encapsulated by fibrous connective tissue, although any of the subtypes may have a multinodular microscopic pattern. This can explain the relatively homogeneous signal intensity of the solid portion of the tumor with the well-circumscribed, low-signal-intensity rim of the tumor capsule on T2-weighted images, as was seen in our cases.
Basal cell adenomas are amenable to conservative resection such as local excision or superficial parotidectomy, whereas the membranous subtype requires parotidectomy. The recurrence rate for the solid and trabecular-tubular variants is almost nonexistent. This contrasts with the high recurrence rate (24%) of the membranous type, which is perhaps a result of the multicentricity of this lesion. Although exceedingly rare, malignant transformation is more common in the membranous type than in the other types (1, 3, 9, 10).
The differential diagnosis for common salivary gland tumors includes pleomorphic adenoma, Warthin tumor, and other low-grade malignant tumors. The monomorphic appearance and the absence of chondroid tissue and myxoid stroma differentiate basal cell adenoma from pleomorphic adenoma. Pleomorphic adenoma often shows heterogeneously intermediate signal intensity on T1-weighted images and high signal intensity on T2-weighted images; however, other salivary gland tumors, including Warthin tumor and other low-grade malignant tumors, show intermediate signal intensity on T1- and T2-weighted images, with more frequent cystic change. The basal cell adenoma is sometimes mistaken for adenoid cystic carcinoma. There are two features that help to distinguish these lesions. One is the circumscription of the basal cell adenoma, which contrasts with the invasive pattern of adenoid cystic carcinoma. The other is the lack of vascularity in the microcystic areas of adenoid cystic carcinoma, which contrasts with the numerous endothelial-lined channels in basal cell adenoma. Although basal cell adenocarcinoma is an epithelial neoplasm that has the cytological characteristics of basal cell adenoma (10), it is characterized by invasive and destructive morphologic growth, in contrast to the noninvasive appearance of basal cell adenoma. Even in the multinodular forms of membranous basal cell adenoma, the individual tumor nodules are well circumscribed and noninfiltrative. In cases of basal cell adenocarcinoma, invasion of the salivary gland parenchyma and adjacent tissue is the rule.
Although basal cell adenoma in the parotid gland is a rare benign epithelial neoplasm with no specific imaging features, it should be differentiated as a salivary gland tumor, especially if it shows a well-enhanced, solid tumor or mixed solid and cystic hemorrhagic tumor with low signal intensity rim on the T2-weighted image.
References
- Received June 26, 2003.
- Accepted after revision July 3, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}