
Abstract
BACKGROUND AND PURPOSE: The lateral tentorial sinus (LTS) has not been well described in the imaging literature. The aim of this study was to investigate the value of MR imaging in assessing the LTS, which may provide guidance for preoperative planning.
METHODS: Fifty-five adult patients underwent MR imaging of the brain. Four neuroradiologists evaluated the studies for delineation of the LTS and its branches. Presence of arachnoid granulation and dominance of the venous drainage also were reported.
RESULTS: An LTS was detected in 104 of 110 lobes. The LTS in each lobe was classified as type I (candelabra) in 30 (28.8%), type II (independent veins) in 22 (21.1%), and type III (venous lakes) in 37 (35.5%); in 15 (14.4%) of the lobes, the LTS was indeterminate. LTS branches were inconsistently detected, with the exception of the vein of Labbé (VL). Five of eight branches were seen in approximately half of the cases. The VL was identified in 94 (85.4%) lobes. Among these, 53 (56.4%) were draining into the LTS and 22 (23.4%) into the transverse sinus; in 19 (20.2%) cases, the terminal portion was not visualized. The right transverse sinus was dominant in 19 (34.5%) patients and the left in 18 (32.7%); codomination was present in 18 (32.7%) cases. At least one arachnoid granulation was seen in the transverse sinus in 27 (49.1%) patients.
CONCLUSION: In many instances, the LTS and VL drainage patterns were well delineated on routine MR images. For selected cases, this information may be crucial during lateral skull base surgery to avoid venous infarct.
Tentorial sinuses are constant venous channels that have been divided into medial and lateral groups (1–3). These sinuses are located on each half of the tentorium. The medial tentorial sinuses are responsible for the venous drainage of the superior cerebellar surface. The medial tentorial sinuses empty into the straight sinus and transverse sinus confluence. The lateral tentorial sinuses are formed by convergence of the veins draining the basal and lateral surface of the temporal and occipital lobes (Fig 1) (1, 3). These sinuses usually drain into the transverse-sigmoid junction and anterior two thirds of the transverse sinus on each side (Figs 1 and 2) (1, 3–5). The veins emptying into the lateral tentorial sinuses can be divided into the medial and lateral branches. The lateral branches include the anterior temporal vein, middle temporal vein, posterior temporal vein, and vein of Labbé (Figs 1 and 3). The medial branches include the anterior temporobasal vein, middle temporobasal vein, posterior temporobasal vein, and occipitobasal veins (Figs 1, 3, and 4) (1–3). These sinuses can be the main venous drainage pathways in situations such as vein of Galen aneurysm and holoprosencephaly when posterior dural sinuses are absent (6–8).

Direct superior of the LTS. 1, anterior temporal vein; 2, anterior temporobasal vein; 3, middle temporobasal vein; 4, posterior temporobasal vein; 5, occipitobasal vein; 6, posterior temporal vein; 7, vein of Labbé; 8, middle temporal vein.

LTS venous configuration.
A, Type I, venous candelabra.
B, Type II, multiple independent veins.
C, Type III, venous lakes within tentorium (14).

Type I LTS. Axial contrast-enhanced T1-weighted MR image obtained in a 37-year-old man shows several branches of the right LTS. 1, anterior temporobasal vein; 2, middle temporobasal vein; 3, posterior tomporobasal vein; 4, occiptiobasal vein; 5, posterior temporal vein; 6, vein of Labbé; 7, middle temporal vein. Left LTS is not well depicted on this image.
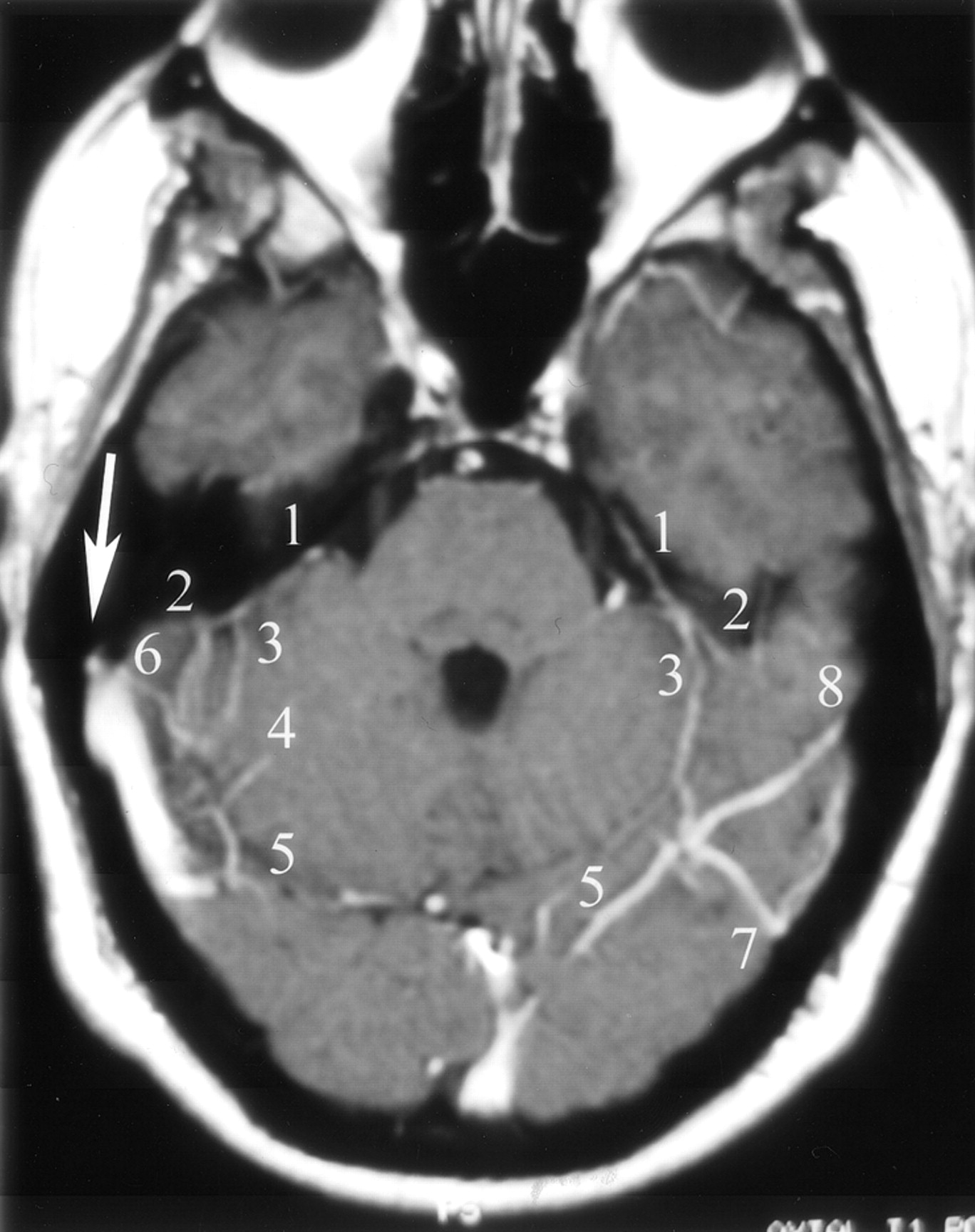
Types I and II LTS. Axial contrast-enhanced T1-weighted MR image obtained in a 55-year-old man with a type I LTS on the left and a type II LTS on the right. Right vein of Labbé terminates into the transverse sinus (arrow). 1, superior petrosal sinus; 2, anterior temporobasal vein; 3, middle temporobasal vein; 4, posterior temporobasal vein; 5, occipitobasal vein; 6, middle temporal vein; 7, posterior temporal vein; 8, vein of Labbé.
Despite its surgical importance, MR imaging of the lateral tentorial sinus (LTS) has not been extensively described in the literature. Although an LTS is commonly detectable on conventional angiograms and MR images, it is often ignored (9, 10) or simply described as a “cortical vein close to the vein of Labbé” (11). Disparity between anatomic studies and radiologic literature may be attributed to lack of notation by the radiologist, technical difficulty in imaging (12), and marked individual variation. Recent introduction of 3D CT angiography and 3D contrast-enhanced MR venography has improved our ability to image and evaluate intracranial dural sinuses and cerebral veins (4, 5, 13). However, in most cases, conventional MR imaging may provide adequate information without the need to use additional MR venography sequences that require additional time for acquisition and interpretation. In this study, our focus was to visualize the LTS and its branches, localizing the terminal portion of the venous lakes, by using conventional T1-weighted spin-echo contrast-enhanced MR imaging.
The temporal lobe is anchored to the tentorium and the transverse sinus via the LTS branches. Therefore, it is not surprising that the LTS branches often are manipulated by the surgeon while mobilizing the temporal lobe to access the deep seated structures during transtemporal, transtentorial, and combined transpetrosal approaches (1, 2, 14–16). Knowing the venous drainage of the posterior temporal lobe is one of the critical issues that directly relates to and influences the maneuvers used during a surgical approach, the potential risk of the venous infarct, and the outcome (11, 14).
Methods
Our cohort study sample consisted of 55 consecutive patients (26 male and 29 female patients; age range, 19–89 years; mean age, 45.5 years) who underwent clinical MR imaging of the brain that included conventional contrast-enhanced T1-weighted MR imaging during December of 2002. All MR imaging studies were performed on a 1.0-T imaging unit with a standard head coil. Axial T1-weighted spin-echo images (648–666/12–20/1 [TR/TE/NEX]; section thickness, 5 mm; intersection gap, 1 mm; field of view, 220–250 mm; matrix, 256 × 224) were obtained after IV infusion of 0.1 to 0.15 mmol/kg body weight gadopentetate dimeglumine contrast material injected manually at 1 to 2 mL/s within a period of 5 minutes after infusion. All axial images used for review were obtained in approximately 5 minutes 30 seconds.
Four neuroradiologists (Z.M., E.G.H., R.V., M.M.) reviewed the images. The following were determined by consensus and were recorded: 1) visualization of the LTS on each side; 2) visualization of the individual branches of the lateral tentorial sinuses; 3) classification of the LTS (type I candelabra pattern, type II multiple independent veins, and type III venous lake formation with or without independent draining veins) (Table 1 and Fig 2); 4) termination of the vein of Labbé (into LTS or transverse sinus); 5) presence of arachnoid granulation in transverse sinuses (determined by a sharp margined filling defect >3 mm); and 6) dominant transverse sinus (determined by size).
The study was limited to patients with dural sinuses that were normal appearing on the MR images. Patient findings consistent with lesions that affect the dural sinuses, previous surgery, trauma, sinus thrombosis, intracranial hypertension or hypotension, or technically inadequate studies were excluded from the analysis. Images showing such pathologic abnormalities are included herein for the purpose of discussion.
LTS branches were labeled according to the nomenclature described by Rhoton and his colleagues (1, 3) (Fig 1). We used the system described by Guppy et al (14) to classify the LTS (Table 1 and Fig 2).
Results
We were able to depict the right LTS in 50 of the 55 studies and the left LTS in 54 of 55 studies (Table 2). Of these, 16 on the right side were classified as type I (Figs 3 and 4), 12 as type II (Figs 4 and 5), and 17 as type III (Figs 5 and 6); five were indeterminate. Similar findings were disclosed on the left side: 14 type I, 10 type II, 20 type III, and 11 indeterminate.

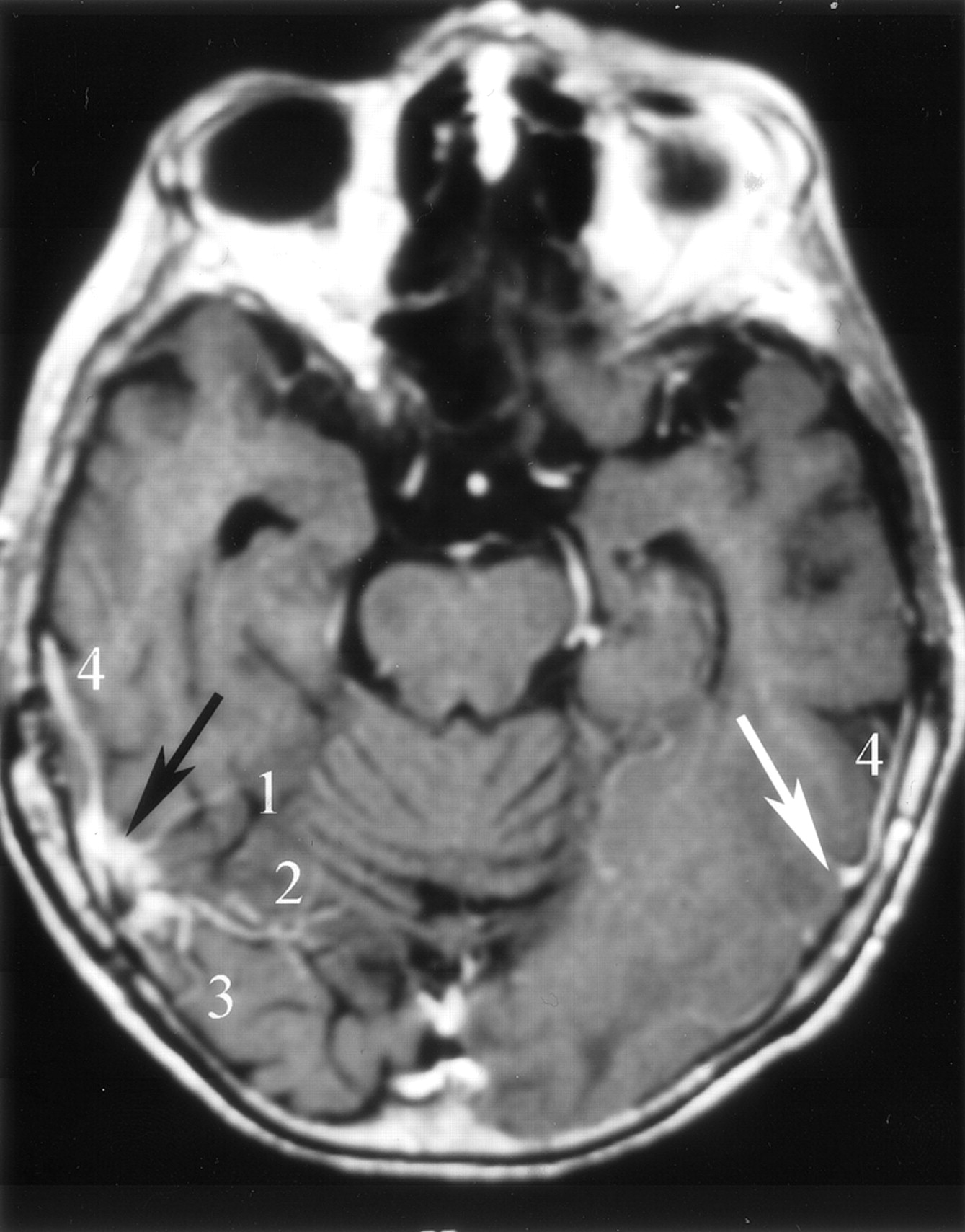
Types II and III LTS. Axial contrast-enhanced T1-weighted MR image obtained in a 34-year-old woman shows a type II LTS on the left and a type III LTS on the right side (black arrows). The veins of Labbé are draining separately into the transverse-sigmoid sinus junction (white arrows). 1, superior petrosal sinus; 2, middle temporobasal vein; 3, posterior temporobasal vein; 4, occipitobasal vein; 5, vein of Labbé.

Type III LTS. Axial contrast-enhanced T1-weigthed MR image obtained in a 57-year-old man depicts “venous lakes” of a type III LTS (black arrow) and the left vein of Labbé just before it drains into the transverse sinus (white arrow). 1, middle temporobasal vein; 2, posterior temporobasal vein; 3, posterior temporal vein; 4, vein of Labbé.
Occurrence by type of lateral tentorial sinuses on contrast-enhanced T1-weighted MR images of 55 patients
The occipitobasal and posterior temporobasal branches (Figs 2–4) were inconsistently seen and separated by our authors. We reached consensus in identifying the remaining six branches of the LTS, and therefore these were included in the final assessment. The anterior temporal branch and anterior temporobasal branch were compiled, because they often share a common trunk before emptying into the LTS (Fig 7). Anterior temporobasal branches and anterior temporal trunk, middle temporobasal branches, posterior temporal branches, and middle temporal branches were seen in 30, 25, 27, and 28 cases on the right, and 29, 26, 27, and 26 cases on the left, respectively (Table 3). Veins of Labbé were identified in 94 lobes (Table 3). Among these, 23 on the right side were draining into the LTS (Figs 3, 7, and 8) and 12 into the transverse sinus (Figs 4, 5, 9); 12 were indeterminate. On the left side, 30 were draining into the LTS and 10 into the transverse sinus; seven were indeterminate.

Anterior temporal vein and anterior temporobasal vein common trunk. Axial contrast-enhanced T1-weighted MR image obtained in a 45-year-old woman with a type I LTS on the right side. Anterior temporal and anterior temporobasal branches form a trunk (arrow) before draining into the LTS. 1, anterior temporobasal vein; 2, posterior temporal vein; 3, vein of Labbé; 4, anterior temporal vein.

Vein of Labbé termination into the LTS. Axial contrast-enhanced T1-weighted MR image obtained in a 39-year-old man shows the VL draining into a type I LTS (arrow). 1, anterior temporobasal vein; 2, middle temporobasal vein; 3, posterior temporobasal vein; 4, occipitobasal vein; 5, posterior temporal vein; 6, vein of Labbé.

Termination of the vein of Labbé into the transverse sinus. Axial contrast-enhanced T1-weighted MR image obtained in a 42-year-old woman shows the right vein of Labbé (arrow) as it drains into the transverse-sigmoid sinus junction. 1, vein of Labbé; 2, middle temporobasal vein.
Visualization of the lateral tentorial sinus branches on contrast-enhanced T1-weighted MR images of 55 patients (excluding posterior temporobasal and occipitobasal veins)
At least one arachnoid granulation was detected in the vicinity of the terminal portion of the vein of Labbé in 27 cases (Fig 10). In 19 cases, the right transverse sinus was dominant, and in 18 cases, the left transverse sinus was dominant; the remaining 18 were codominant (Fig 11). As an incidental finding, four sphenopetrosal sinuses were depicted, two of which were prominent (Fig 12).

Arachnoid granulation in type III LTS. Axial contrast-enhanced T1-weighted MR image obtained in a 61-year-old woman shows multiple venous tributaries of a type III LTS. Note the close relationship between the vein of Labbé and the arachnoid granulation (arrow). 1, vein of Labbé; 2, anterior temporobasal vein; 3, middle temporoabasal vein; 4, posterior temporobasal vein; 5, occipitobasal vein; 6, posterior temporal vein.

Tentorial meningioma displacing a type III LTS. Axial T1-weighted contrast-enhanced MR image obtained in a 64-year-old man shows a posterior fossa meningioma (asterisk) compressing the transverse sinus and distorting the nearby LTS (arrow). Note that the transverse sinuses are codominant and that the confluence of sinuses is widely patent. 1, superior petrosal sinus; 2, anterior temporobasal vein; 3, vein of Labbé; 4, occipitobasal vein.

Sphenopetrosal sinus in a patient with a petroclival meningioma.
A, Left common carotid artery injection, venous phase image obtained in a 61-year-old woman who presented with persistent headache reveals sphenotemporal sinus (arrowhead) draining into the transverse-sigmoid sinus junction (arrow).
B−D, Axial contrast-enhanced T1-weighted MR images again show a left petroclival meningioma (asterisks) and sphenopetrosal sinuses (arrows) emptying into transverse-sigmoid sinus junction, which is better seen on the right side (arrowhead). 1, superior petrosal sinus; 2, vein of Labbé; 3, occipitobasal vein; 4, posterior temporal vein; 5, middle temporal vein.
Discussion
Surgical Implication
Mapping the temporal venous anatomy is crucial for surgeons considering lateral skull base explorations (2). During such operations, surgeons often manipulate the LTS and its branches while lifting up the temporal lobe to achieve adequate exposure and working space (2, 12, 14–16). Surgeons make the best effort to preserve the bridging veins to avoid a venous infarct (10, 17, 18). We think that conventional contrast-enhanced MR imaging can be used as a tool to evaluate the temporal venous anatomy. Neuroradiologists should try to shed light on the following as they assess the imaging of such cases: 1) LTS type (types I and III require more careful handling of the tentorium to avoid damaging the LTS) (Figs 2–6) (14); 2) termination of the VL (early termination into the LTS calls for a combined petrosal approach) (Figs 3, 4, and 8) (15); 3) presence of a sphenoparietal sinus (often precludes standard petrosal approach) (Fig 12) (2); 4) venous drainage dominance (sacrifice of a dominant transverse and sigmoid sinus on the side of craniotomy can have catastrophic consequences) (19); 5) high jugular bulb and prominent sigmoid sinus or jugular bulb (limits the presigmoid working space and mastoidectomy for petrosal approach) (20).
LTS Type.
In many instances, the lateral skull base approach requires manipulation and incision through the tentorium. Such maneuvers should be avoided in cases with type I or III LTS, in which the temporal bridging veins converge in a single trunk or in venous lakes. Simple technical modifications, such as placing the spatula under the tentorium rather than the temporal lobe or using the “dura-reflecting technique,” may be help to preserve the temporal bridging veins (14, 21).
Termination of the Vein of Labbé.
The temporal lobe can be mobilized to the extent granted by the vein of Labbé. As a general rule, the more anterior these bridging veins terminate, the more difficult it is to deal with the temporal lobe and the tentorium because of limited working space (2). The vein of Labbé usually drains in to the LTS (Figs 3, 4, and 8) and less often into the transverse sinus (Figs 5 and 9) (22). The latter would make it easy for the surgeon to separate the vein of Labbé from the tentorium while mobilizing the temporal lobe. When a bridging vein terminates early into the tentorial sinus before entering the transverse sinus, surgical visualization is significantly restricted. This drainage pattern would limit the retraction of the posterior temporal lobe, and therefore exposure in a standard petrosal approach (15). In such cases, a wider working space can be achieved by extending the dural excision anteriorly and by adding an anterior petrosectomy (combined petrosal approach). On the other hand, intradural termination of the vein of Labbé into the anterior portion of the transverse sinus may also limit the mobility and surgical window (22). This rare anatomic variation often requires careful incision of the dura on both sides and separating the vein from the bone before mobilizing the temporal lobe. We were not able to show this anatomic variation with the prescribed imaging technique.
Presence of a Sphenoparietal Sinus.
The superficial sylvian vein usually drains directly or indirectly via sphenoparietal sinus into the cavernous sinus (4, 5, 13, 23). It rarely drains via the dural sinus along the floor of the middle cranial fossa sphenopetrosal sinus or sphenotemporal sinus into the superior petrosal or LTS (5, 13). The presence of such sinuses precludes a petrosal approach, because it limits mobilization of the temporal lobe by tethering it to the anterior edge of the tentorium (2). A combined presigmoid and lateral orbitozygomatic approach has been recommended in those cases (Fig 12) (2).
Venous Drainage Dominance.
One of the techniques that may widen the exposure during a lateral skull base approach is to divide the lateral sinus between the entrance of the vein of Labbé and the superior petrosal sinus. This maneuver requires patency of the confluence of sinuses, the opposite lateral sinus, and internal jugular vein (Fig 11) (19).
High Jugular Bulb and Prominent Sigmoid Sinus or Jugular Bulb.
A prominent sigmoid sinus or jugular bulb would limit the presigmoid working space. An anterior petrosectomy can be added to increase the working space in such instances (15). Similarly, a high jugular bulb may make mastoidectomy for petrosal approach difficult. In this situation, a sufficient working space could be achieved by exposing the jugular bulb and by gently mobilizing the sinus (20).
As clearly reflected in the above-mentioned surgical scenarios, knowledge of the temporal venous anatomy is crucial for the surgeon who is considering a lateral skull base approach (2, 11, 12, 14–16). Violating any venous structure in this region may result in a venous infarct that could have serious or even fatal consequences (10, 11, 17, 18).
Sample Cases
Case 1.
A 64-year-old man had a posterior fossa meningioma compressing the left transverse sinus and distorting the nearby LTS (Fig 11). The lesion was displacing a type III LTS. The transverse sinuses were codominant, and the confluence of sinuses was widely patent. This patient underwent a combined posterior fossa craniotomy. The left transverse sinus was ligated, and the tumor was completely excised with the overlying dura and part of the transverse sinus while sparing the LTS. The surgery and the postoperative course were uneventful.
Case 2.
A 61-year-old woman presented with persistent headache. MR imaging revealed a petroclival meningioma. An axial contrast-enhanced T1-weighted MR image showed the presence of sphenopetrosal sinuses emptying into the transverse sinus sigmoid sinus junction, which was confirmed by angiography (Fig 12). Instead of a standard petrosal approach, a combined approach was planned for this patient.
Interpretation of Results
Overall, our results, with a few exceptions, are comparable to previously published anatomic and angiographic studies. The most common LTS type we encountered was type III (35.5% [Figs 2, 6, and 11]). This varied from results of a cadaver study by Guppy et al (14) that reported type II (45%) to be the most common type. Our results regarding depiction of the VL and its termination are similar to the findings of a cadaver study presented by Koperna et al (22). The authors were able to see VL termination in 82% of the specimens, 73% of which drained into the LTS (Figs 3, 4, 6, and 8) and 27% of which drained into the transverse sinus (Figs 4, 5, and 9) (22). Arachnoid granulation in the transverse sinus has been shown to reliably indicate the termination of the VL (Fig 10) (24). At least one arachnoid granulation in the transverse sinus was depicted in 27 of our 55 patients. Recently, Liang et al (4) reported the presence of arachnoid granulation in transverse sinuses in 69 of 90 patients by using 3D contrast-enhanced gradient-echo MR venography. We showed even distribution among right, left, and codominant venous drainage. Durgun et al (25) conducted a retrospective assessment of 189 carotid angiographic studies, and reported that 41.3% of venous drainage occurred predominately on the right side, 18.5% on the left side, and 37.6% equally on both sides. Four (3.6%) sphenopetrosal sinuses were incidentally detected in three of our patients (Fig 12). This variation has been reported in 2% of 250 patients when using 3D CT angiography (13).
The reason for the discrepancies in classifying the LTS types and determining the venous dominance drainage between our results and those presented in the literature is unclear. One can argue that use of a dedicated MR venography technique would render a more reliable and detailed result. Further investigations with correlation to the criterion standard conventional angiography are needed to assess the validity of our results and perhaps to develop a standard preoperative venous mapping strategy. Of note is that our study was conducted in adult patients only, and that our results should therefore not be directly extrapolated for the pediatric population.
Conclusion
The LTS and some of its branches can be delineated on conventional contrast-enhanced MR images and should not be mistaken for arteriovenous malformations or venous angioma. In patients harboring a lesion, which may require lateral skull base surgery, knowledge of the LTS drainage may guide the surgeon in selecting the approach that is least likely to result in postoperative morbidity. This potentially useful information often goes unreported.
Acknowledgments
The authors thank Eugene Martinello, McMaster University Health Sciences Centre, Hamilton, Ontario, Canada, for preparing the illustrations.
Footnotes
Previously presented in part as a platform session at the 38th Meeting of the Canadian Congress of Neurological Sciences, Quebec City, Quebec, Canada, June 17–21, 2003.
References
- Received August 6, 2003.
- Accepted after revision December 22, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}