
Abstract
BACKGROUND AND PURPOSE: Optimal means for assessing cerebral vasospasm, mainly at the vertebrobasilar system, have not been established. The purpose of this study was to evaluate the role of multisection CT angiography (MCTA) in the detection and quantification of vertebrobasilar vasospasm (VBS) indicated on transcranial Doppler (TCD) imaging in patients with subarachnoid hemorrhage (SAH).
METHODS: Forty-three MCTA studies of the vertebrobasilar arteries were performed with a multisection spiral CT scanner in 36 patients with SAH. Parameters used were 1-mm collimation, 0.625Q pitch, 120 kV, and 250 mAs. Contrast material was injected (80–100 mL, 3 mL/s) after a 15–20-second delay. Postprocessing of the vertebrobasilar system was performed by using maximum intensity projection and volume-rendering reconstruction. Vessel diameter was measured at different intracranial locations along the vertebral and basilar arteries perpendicular to their long axis by using curved reformatted multiplanar reformation. TCD imaging of the posterior circulation was performed within 24 hours.
RESULTS: MCTA demonstrated narrowed arteries compatible with VBS in 13 patients, consistent with TCD findings. Despite TCD recordings of high flow velocity in three other patients, MCTA did not reveal vasospasm but did show wide arteries feeding arteriovenous malformations in two and normal-sized arteries in one. VBS in two patients was identified on MCTA but overlooked during TCD imaging. Twenty patients had normal findings on both TCD and MCTA studies.
CONCLUSION: Cerebral MCTA is recommended as a reliable, rapid, and minimally invasive diagnostic method, one complementary to TCD imaging for assessing VBS in patients with SAH.
Cerebral arterial spasm is the most frequent complication after subarachnoid hemorrhage (SAH) and one of the leading causes of morbidity and mortality in patients with SAH. Guidelines for optimal diagnostic algorithms have not yet been established, and various modalities have been examined for this purpose.
Transcranial Doppler (TCD) imaging is an accurate tool for evaluating flow velocities (FVs) in the major cranial vessels in patients with SAH. Numerous studies have confirmed the relationship between elevated FVs in the major cerebral arteries and arterial vasospasm (1–3). However, increased FVs do not necessarily reflect reduced vessel diameter, as both cerebral hyperemia and arterial vasospasm can lead to high FVs and cannot be distinguished by means of TCD alone (4, 5).
Consequently, morphologic evaluation of cerebral vessels with angiography remains the mainstay in diagnosing cerebral vasospasm. Currently techniques are based on digital subtraction angiography (DSA). Although DSA is an invasive procedure with known technical demands and complications (6–9), CT angiography (CTA) is considered a relatively safe, fast, and minimally invasive procedure (10–11). In recent years, CTA has emerged as a reliable tool for the morphologic evaluation of intracranial vessels. Also, various studies have demonstrated the accuracy of CTA in detecting vascular diseases (10–12), even in the presence of acute SAH. The introduction of multisection CT systems has enabled faster acquisition and better reconstruction. Multisection CTA (MCTA) performed with a multisection system has been shown to be superior to DSA in detecting small vascular diseases such as tiny aneurysms (13).
Still, little has been reported on the accuracy of MCTA in the diagnosis of vasospasm (14–20). Further, most studies have involved the anterior circulation; therefore, data on the clinical value of CTA in the diagnosis of vertebrobasilar vasospasm (VBS) are not available (21, 22). To our knowledge, no study has examined the diagnosis of VBS diagnosis by using MCTA.
In recent years, increasing attention has been given to VBS (23), particularly in posttraumatic SAH (21, 23–27). Our purpose was to prospectively investigate the role of MCTA in the evaluation and quantification of VBS in patients with SAH.
Methods
Patients
Thirty-six patients admitted to our neurosurgical department with acute SAH diagnosed on standard CT studies were included in this prospective study. Informed consent was obtained from all patients, including 22 men and 14 women ranging in age from 18 to 74 years (mean, 45.6 years ± 16.1). SAH was spontaneous in 27 patients, posttraumatic in eight, and postoperative in one.
MCTA Studies
A total of 43 MCTA studies were performed. In the 27 patients who had spontaneous SAH, MCTA studies were performed within 48 hours of their admission as part of our routine evaluation. In nine patients, CTA was indicated because of sustained, elevated FVs in the posterior circulation for at least 48 hours, as detected during TCD imaging; this was suggestive of vasospasm. Seven patients underwent additional MCTA study: In five patients, additional CTA was indicated because of TCD findings suggestive of vasospasm, and in two, second MCTA was performed as follow-up evaluation.
In all patients, high-resolution MCTA was performed with a multisection CT scanner (MX 8000 or MX 8000 IDT; Philips, Best, the Netherlands). Every patient was imaged from the upper cervical spine to the convexity of the brain. Imaging parameters were as follows: 120 kV, 250 mAs, 250-mm field of view; 512 × 512 matrix, 1–1.3-mm section width with 50% overlapping, and −0.675 pitch.
Nonionic contrast material was injected by using an intravenous catheter placed in a peripheral vein. A total of 80–100 mL was injected at a rate of 3 mL/s with a power injector after a delay of 15–20 seconds. The data were transferred to a workstation (MX View; Philips) for postprocessing. Reconstructions included the following: 1) maximum intensity projection (MIP), 2) four-dimensional CTA with volume rendering, 3) reformatted multiplanar reformation (MPR, Masrecut, Algoteck, Raanana, Israel) performed through each of the vertebral arteries (VAs) and basilar arteries (BAs), and 4) views perpendicular to the route of each vessel at selected locations along the arteries. The last enabled evaluation and accurate measurement of the diameter of the vessels at each level.
Diameters of the intracranial and extracranial segments of the VAs and BAs were measured by using window settings of 150 HU for center level and 500 HU for window width. For each artery, the narrowest segment was selected to assess the correlation with the highest FVs selected for TCD analysis. At each location, three independent measurements were averaged. Arterial spasm was categorized as mild, moderate, or severe when the vessel diameters were reduced by <30%, 30–50%, or >50%, respectively, as compared with the diameter of the nearest normal-appearing segment of the artery. Two experienced neuroradiologists (D.G., R.S.), who were blinded to the TCD results, performed all postprocessing reconstructions and measurements independently. Mean time of postprocessing work was 45 minutes per patient throughout the study.
TCD Studies
TCD studies were performed by using a system (Intraview; Rimed, Raanana, Israel) with a 2-MHz pulse-waved, range-gated transducer, according to the technique that Aaslid et al described (1). The VAs were insonated with the transducer on the posterior cervical triangle aimed at a depth of 45–55 mm for the extracranial segment, with a depth of at least 70 mm for insonation of the intracranial segments. The BA location was defined at an insonation depth above 80 mm, according to the technique that Fujioka and Douville described (26). FV in the BA was recorded in at least three locations. The highest was located at a depth above 90 mm. The TCD criterion for VBS was defined as a mean FV higher than 80 cm/s. TCD recordings were performed within the first 48 hours after admission and on a daily basis thereafter until the patient’s discharge or until TCD measurements stabilized at normal FVs.
Results
Overview
The vertebrobasilar and other major cerebral arteries were satisfactorily imaged during MCTA in all instances, regardless of the amount and attenuation of SAH. High-quality MIP and volume-rendered reconstructions were achieved in all cases. The bones at the base of the skull were difficult to remove in the production processing of MIP images by using the threshold technique. Yet, when we used the volume-rendering technique, these bones provided a suitably bright background for the arteries, supplying better morphological and anatomic information (Fig 1).

Bilateral vertebral spasm in a patient with posttraumatic SAH. Posteroanterior volume-rendered MCTA scan shows diffuse arterial spasm of the right intracranial segment and focal spasm in the left intracranial VA.
The curved MPR mode—the so-called Mastercut built on the volume-rendering reconstruction—enabled stretching and straightening of the arteries for clear visualization of changes in caliber along their route and evaluation of the length of the narrowed or widened segments (Fig 2). It also enabled the acquisition of sections perpendicular to the long axis of the vessel. These provided accurate measurements of the true diameter of the vessel at any desired location for both extracranial and intracranial segments of the arteries of the posterior cerebral circulation.

Same patient as in Figure 1. A, Mastercut view through the right VA with straightening of both extracranial and intracranial portions shows diffuse narrowing of the intracranial segment from the level of the foramen magnum. B, Mastercut through the left VA shows focal narrowing (arrow) at the intracranial segment C–E, Sections perpendicular to the arterial long axis below (C), at (D), and above (E) the focal spasm provide accurate measurements of vascular diameter at each location. Note the evenly narrowed diameter of the diffusely spastic right VA.
The average diameter of the extracranial segments of the VA was similar in all patients, whereas the average diameters of the intracranial segments of the VA and the BA were significantly smaller, indicating vasospasm in the vertebrobasilar system in 16 (44.4%) of 36 patients (Table). These patients had basilar spasm, which was mild in seven, moderate in one, and severe in eight. In all patients with basilar vasospasm, only a segment of the artery was affected, indicating focal spasm, with the diameter of the normal segment serving as a reference value. Vertebral spasm was found on MCTA in 15 patients; it was bilateral in 13 (36.1%) (Fig 1) and unilateral in two (5.6%). The spasm was graded mild in three, moderate in five, severe in seven and diffusely distributed along the intracranial segment.
Arterial diameter without and with elevated FV on TCD study
Seven of 16 patients with MCTA evidence of VBS underwent additional MCTA. In five patients, the first routine MCTA study was performed early after their admission and depicted no vasospasm; therefore, we were able to use these as control studies. The second study was indicated by TCD values suggestive of substantial VBS. In the remaining two patients, the first MCTA study revealed VBS, and additional MCTA was performed as a follow-up evaluation when TCD findings returned to normal. In all seven patients, the diameters of the BAs and VAs were significantly larger on the control studies than on the studies performed at the time of the peak of arterial spasm. Among four patients, arterial diameters were within the normal range of the control study in one patient (Fig 3), mildly reduced in two, and moderately decreased in one.

MCTA obtained in a 68-year-old patient with SAH.
A, Severe bilateral vertebral spasm.
B, Widening of the vessel toward its normal diameter 3 days later, after treatment.
Correlation with TCD
As a group, patients with significantly reduced BA diameters (2.3 mm ± 0.7) on MCTA fulfilled the TCD criteria for VBS, as compared with patients with larger diameters (3.8 mm ± 0.6, P < .0001) (Table; Fig 4). Individual analysis, however, revealed significant discrepancies between MCTA findings and TCD values. Among the 16 patients with CTA evidence of VBS, only 14 had elevated FVs in the BA. In the remaining two patients, basilar vasospasm was overlooked during TCD imaging, with measured BA FVs lower than 80 cm/s. In these two patients, the vasospasm was considered moderate on the basis of MCTA results.

Correlations.
A, BA diameter (BA D) and BA FV (BA FV).
B, Intracranial VA diameter (IVA D) and IV FV (IVA FV).
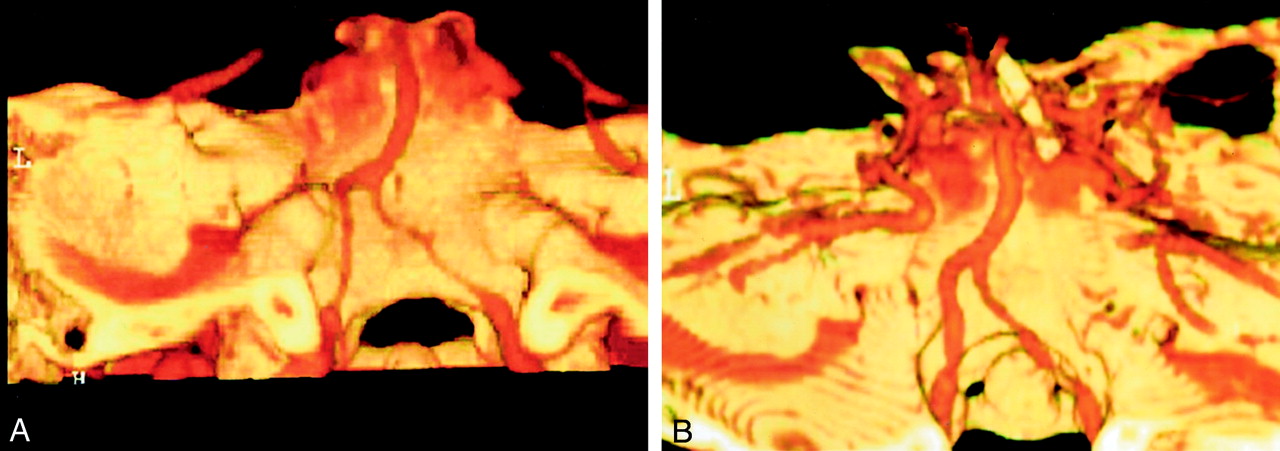
In contrast, three patients with BA FVs higher than 80 cm/s on TCD study had no CTA evidence of VBS. Two had arteriovenous malformations (AVMs), which were supplied by the posterior circulation and were revealed on CTA study and proven on DSA. These findings included a right thalamic AVM (Fig 5) and a left cerebellar AVM, explaining the increased FVs in the BA on TCD. The third patient in this group had posttraumatic SAH. MCTA results ruled out vasospasm in the posterior circulation or other gross vascular disease. The combination of the normal MCTA appearance of the vertebrobasilar arteries in this patient and the elevated blood FVs in the extracranial segments of the cerebral arteries on TCD reduced the difference in cerebral arteriovenous oxygen concentrations and increased intracranial pressure. Together, these findings indicated cerebral hyperemia.

Patient with an AVM. Volume rendering of a right thalamic AVM (A) on MCTA explains the high FV found on TCD imaging. VAs (B) and BAs (C) were wide in diameter, as measured on the sections.
Discussion
Accumulating evidence links arterial vasospasm in the vertebrobasilar system to a poorer outcome in patients with SAH, especially after head trauma. Because a substantial percentage of these patients are comatose and often sedated, obvious clinical signs of VBS are likely to be masked, enhancing the need for an accurate and reliable means of diagnosing vasospasm in the vertebrobasilar system. TCD imaging is currently used for this purpose, as it is a noninvasive and effective bedside screening tool that can be used on a routine basis with minimal cost. Previous studies have established the relationship between elevated blood FVs in the major cerebral arteries and arterial vasospasm (3–4). However, increased FVs reflect a physiologic phenomenon that may not necessarily be the result of narrowed vessel diameter. Therefore, TCD findings may be misleading because cerebral hyperemia may also produce the same high FVs. Previous studies have also shown that elevated FVs identified during TCD imaging indicate a poorer prognosis only when they are associated with reduced cerebral blood flow. Clinical and experimental studies have demonstrated that a reduction in vessel diameter by at least 50–60% is needed before significant flow reduction occurs (28–30). This finding may explain the relatively small number of patients with delayed brain ischemic lesions among those with TCD evidence of vasospasm, emphasizing the need for a quantitative evaluation of vessel narrowing.
Until recently, DSA has been the mainstay for the morphological evaluation of vasospasm following SAH. However, conventional angiography is less available than other studies and an invasive and manpower- and time-consuming procedure. Moreover, conventional angiography can be difficult to repeat, as is sometimes clinically indicated, especially in critically ill and ventilated patients. These patients often need standard head CT and MCTA can be added in less than 40 seconds in the same session. Unlike conventional angiography, MCTA is unable to show dynamic characteristics of blood flow, but it provides a rapid, minimally invasive morphologic study of brain vasculature with 3D details—at lower risk and cost. It is an accurate diagnostic tool for assessing the intracranial vasculature, even in the presence of acute SAH (10–12). MCTA can demonstrate cerebral arterial spasm (14–17) and was recently proved to be accurate and equal to DSA in detecting spastic as well as normal vessels (18–20). These studies dealt mainly with vessels of the anterior circulation, where clinical indications supported a diagnosis of vasospasm. The posterior circulation was neglected, despite its clinical and prognostic importance, particularly in trauma patients in whom the scarcity of typical symptoms and signs is an obstacle to correct diagnosis.
The use of multisection CT for CTA renders the procedure so rapid that patient movements hardly affect it. Furthermore, advanced postprocessing software improves morphological depiction of blood vessels. The anatomic relationship with surrounding structures is enhanced, and the images can be displayed with three-dimensional details in a rapid and easily reproducible fashion. Volume-rendering reconstruction mode eliminated the difficulties imposed by the proximity of the bones at the base of the skull to the vessels imaged, as this may hinder postprocessing reconstruction of blood vessels in the posterior fossa (31). Therefore, we consider volume rendering the preferred and primary reconstruction mode that also enables the performance of curved MPR. Direct demonstration of the vascular walls on the sections achieved only with MCTA assists in differentiating atherosclerotic narrowing from spasm. MCTA also enables accurate measurements of luminal diameter, thereby providing quantitative data on arterial spasm to help select patients with severe spasm for endovascular or other treatments.
Conclusion
Our results show MCTA to be an accurate and reliable method for quantifying and grading VBS in patients with SAH. It can be used to diagnose VBS correctly and differentiate it from cerebral hyperemia, as both of these conditions can produce high FVs on TCD study. As a highly available, feasible, and accurate technique, MCTA should be used as a routine primary procedure—one complementary to TCD study—for the diagnosis of VBS in patients with SAH. DSA should be used for solving discrepancies between TCD and CTA results and for treatment purposes.
Acknowledgments
The authors thank Ms. H. Wolf, Mr. S. Weizman, and Mr. P. Lavodviz for their outstanding technical assistance and Mrs. M. Perlmutter and Ms. A. Rosner for their help in the preparation of this paper.
References
- Received September 9, 2003.
- Accepted after revision February 29, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}