
Abstract
Summary: This report describes invasion of overlying calvaria and soft tissues by a high-grade glioma without macroscopic evidence of dural involvement. The initial radiologic examinations demonstrated a heterogeneous mass in the right frontoparietal region with both extra- and intra-axial components. Inward displacement of the adjacent dura initially prompted consideration for extra-axial lesions such as metastatic lesions, lymphoma, or an aggressive meningioma. The pathologic findings demonstrated a glial cell origin.
Invasion and destruction of calvaria by high-grade gliomas is exceedingly uncommon (1–3). Direct invasion of the temporal bone by a glioma has also been described (4).
More commonly, invasion of the calvaria is reported after previous surgery, either through a craniotomy or biopsy site (5–9). Direct extension of glioblastoma multiforme (GBM) into the orbit has been described, invading along white matter tracts (10). Postradiation gliosarcoma has also been described with associated bone destruction (11). To our knowledge, invasion and destruction of the calvaria from a GBM, without prior surgery or radiation, and without macroscopic destruction of the dura mater, has not been described previously. Calvarial destruction with associated intra-axial lesions on imaging may prompt the diagnosis of extra-axial tumors such as aggressive meningiomas, metastasis and lymphoma. We report an unusual case of frontoparietal GBM with destruction of the calvaria and scalp involvement in the absence of prior surgery or radiation.
Case Report
A 68-year-old African American man with a history of congestive heart failure, hypertension, diabetes mellitus, and chronic renal insufficiency presented to the neurosurgical service with increasing headaches and clumsiness of the left hand lasting a few days. On physical examination, he had left hemianospia with left-arm pronator drift. Palpation of the scalp revealed a soft tissue mass over the right parietal area. Further work-up included chest radiography, without evidence of malignancy and a prostate specific antigen level within normal limits.
Imaging
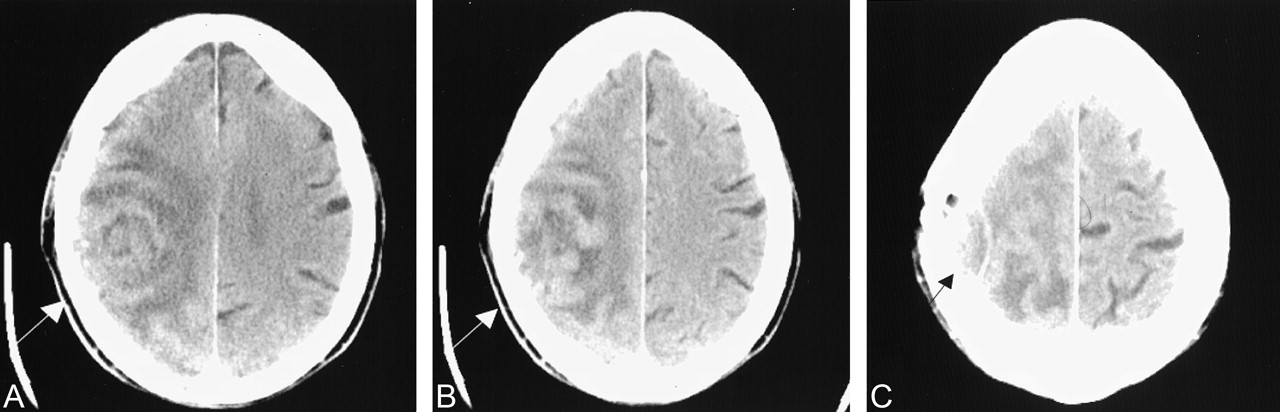
Because of renal insufficiency, a nonenhanced CT study was performed (Fig 1). The images showed an ill-defined, heterogeneous right frontoparietal mass causing moth-eaten, permeative destruction of the calvaria (Fig 2). Intra- and extra-axial localization was difficult secondary to lack of intravenous contrast enhancement. Overlying calvarial destruction and inward dural displacement prompted preliminary diagnostic considerations of aggressive meningioma, metastasis, or lymphoma.

CT scans.
A and B, Nonenhanced scans obtained at slightly different heights show a rounded heterogeneous mass in the right frontoparietal region (arrow).
C, Higher section shows inward dural displacement (arrow) and overlying calvarial destruction, suggesting extra-axial extension of the mass.

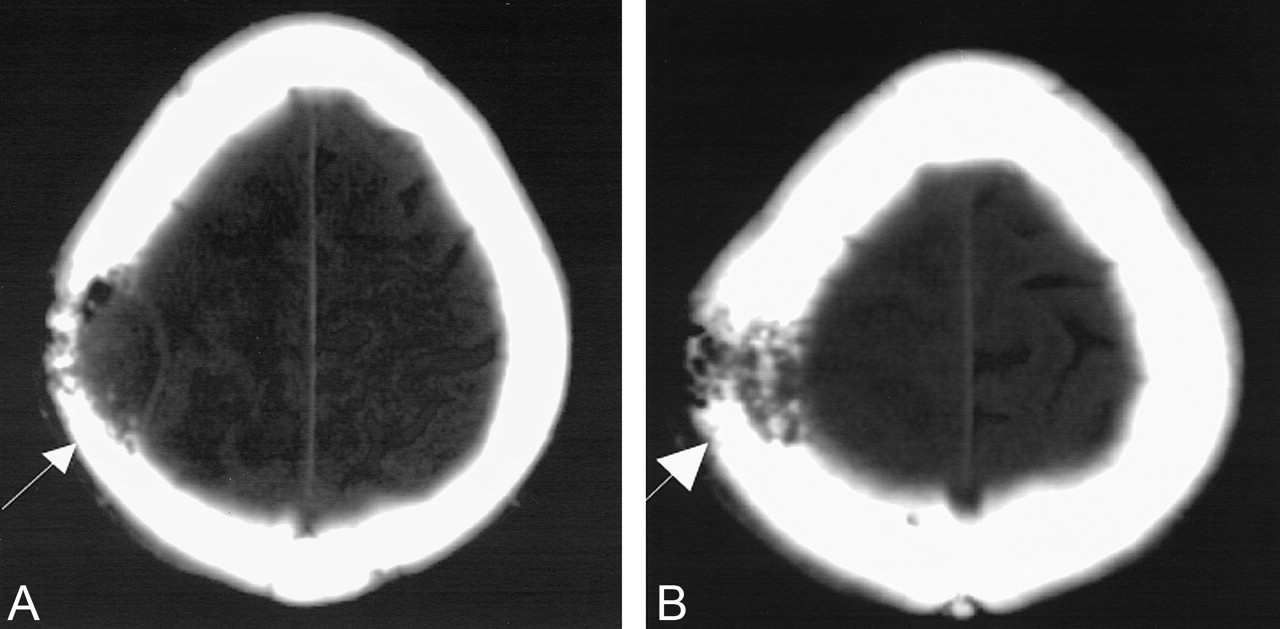
Bone window settings from the same nonenhanced CT study as in Figure 1 shows calvarial destruction (arrow).
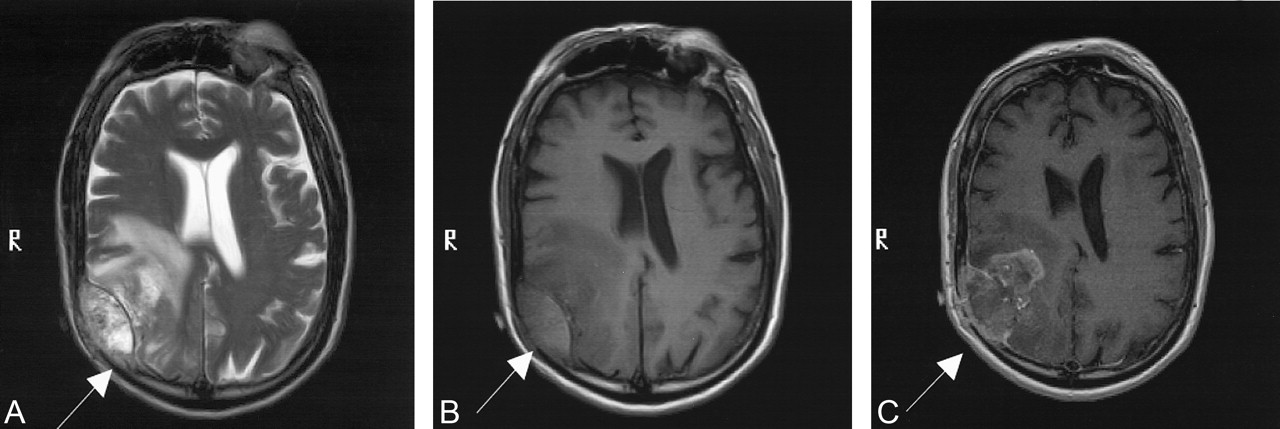
Results of preoperative MR imaging (with Stealth fiducials; Medtronics, Minneapolis, MN) confirmed the CT findings and showed both intra- and extra-axial necrotic, enhancing lesions in the right frontoparietal region (Fig 3). Tumoral involvement of the frontoparietal white matter and overlying calvaria and soft tissues was noted, without definite discontinuity of the dura on imaging (Fig 4). The extra-axial component showed heterogeneous, predominantly bright T1 and T2 signal intensity. Given these findings, sarcoma and GBM were added as diagnostic considerations.

MR images demonstrate intra- and extra-axial locations of the mass eroding through the calvaria (arrow). Note inward displacement of the hypointense dura.
A, T2-weighted image.
B, T1-weighted image.
C, Gadolinium-enhanced T1-weighted image.

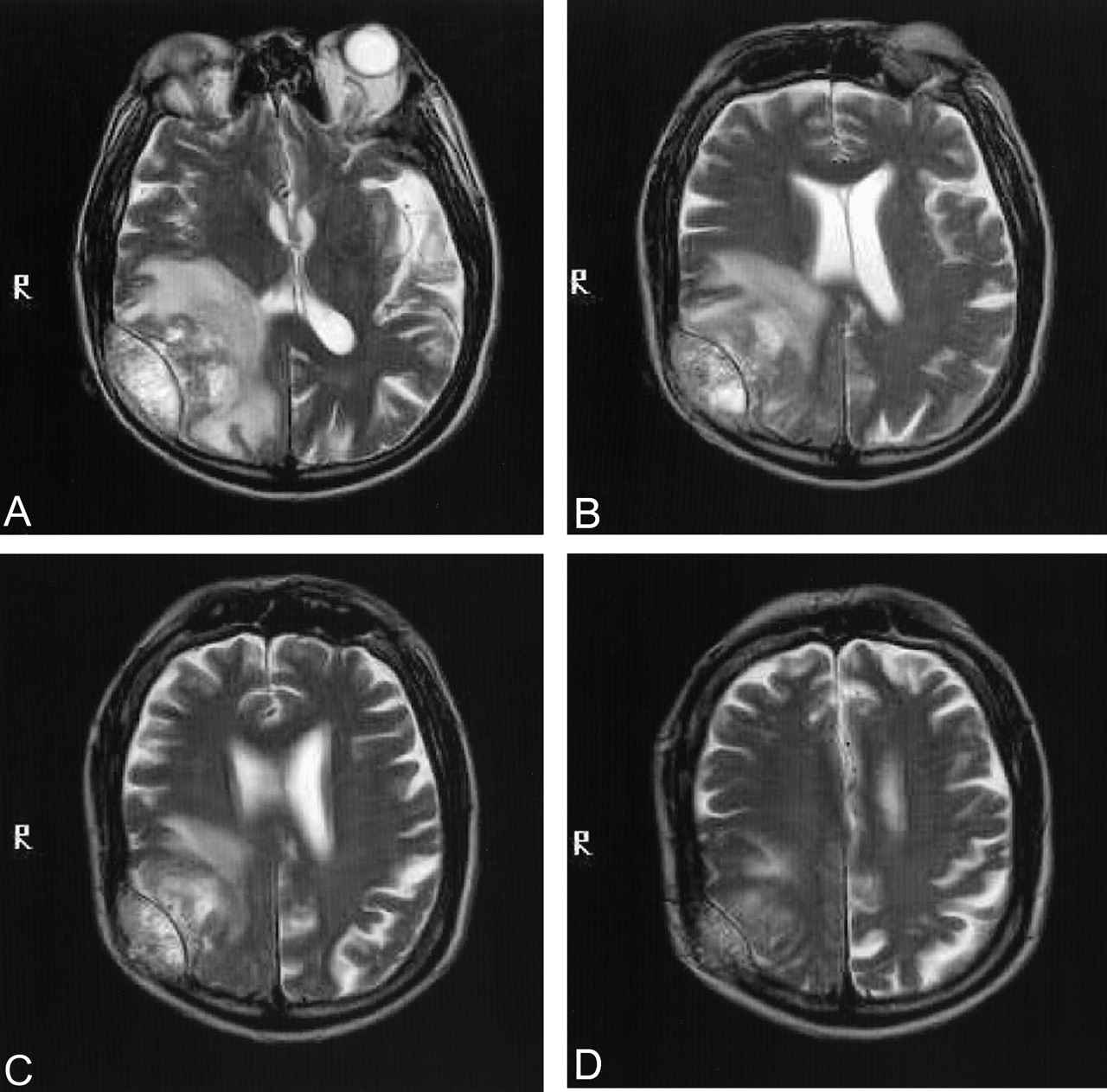
Sequential T2-weighted images demonstrate no definite gross violation of the dura.
Intraoperative Findings
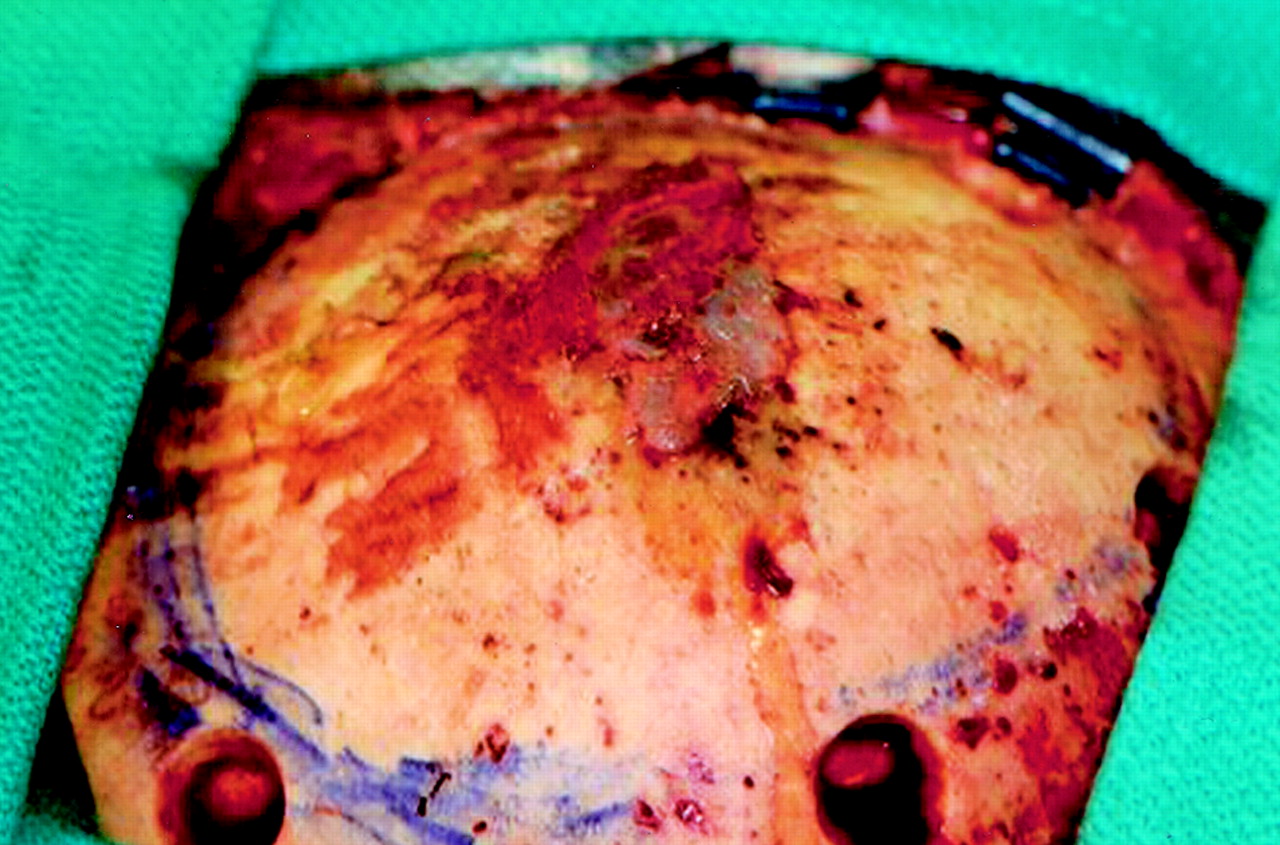
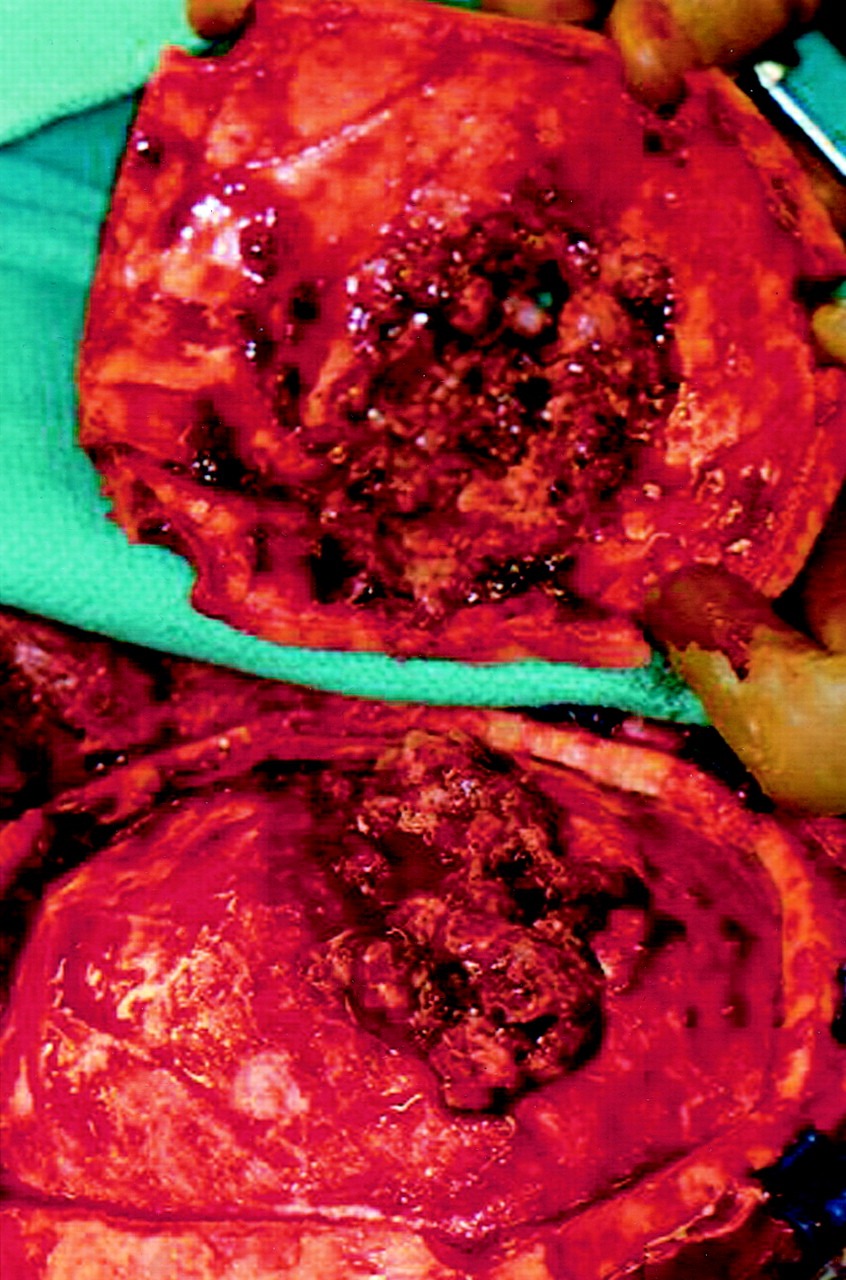
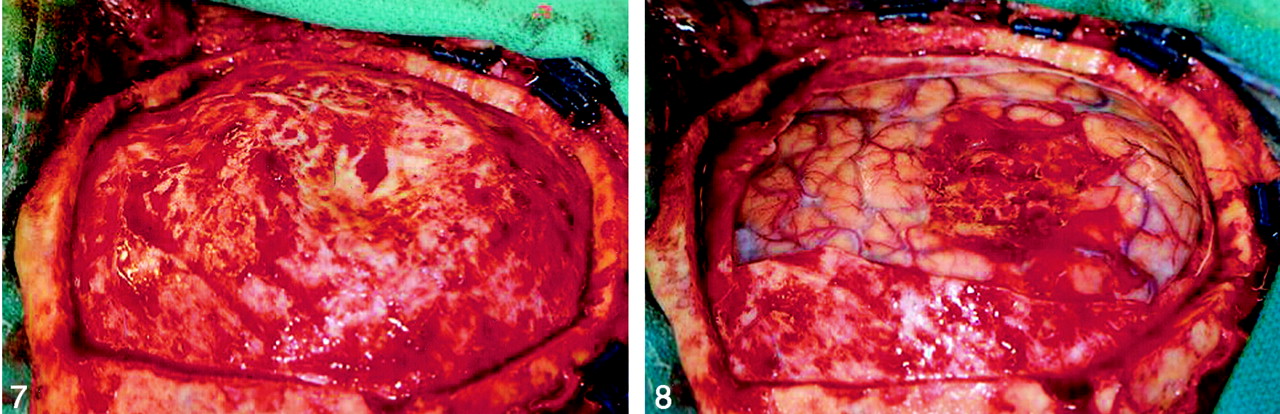
The patient was offered image-guided craniotomy for diagnosis and resection of this lesion. He received standard preoperative medication, including phenytoin, dexamethasone, antibiotics, and mannitol on the morning of surgery. A linear parasagittal incision over the tumor was planned by using intraoperative localization. After the scalp was opened, the tumor was immediately visible. The tumor mass had infiltrated the galea of the overlying scalp, which was then resected. Craniotomy was performed by using wide margins around the destroyed calvaria with the use of multiple burr holes. (Figs 5 and 6) After the bone flap was removed, a large tumor mass was found in the epidural space (Fig 7). The dura under this mass was completely intact macroscopically. The epidural mass was easily peeled off the dura mater. The dura was then excised widely around the tumor mass, and attention was focused on the subdural and intraparenchymal part of this lesion. (Figs 7 and 8) The bulk of the tumor was gray, soft, and friable without clearly identifiable margins between tumor and surrounding normal brain tissue. By using intraoperative navigation, near-total resection was achieved. The dura was repaired with bovine pericardium dural substitute. The bone flap was then inspected and the tumor resected. With a high-speed drill, all abnormal bone was drilled off, and titanium mesh was used to repair the defect. The bone flap was irradiated with 120 Gy, then replaced and secured with a titanium plating system. The scalp was closed. Postoperatively, the patient’s hemiparesis improved, with unchanged visual fields on confrontation.

Tumor eroding through the bone before the bone flap was created.
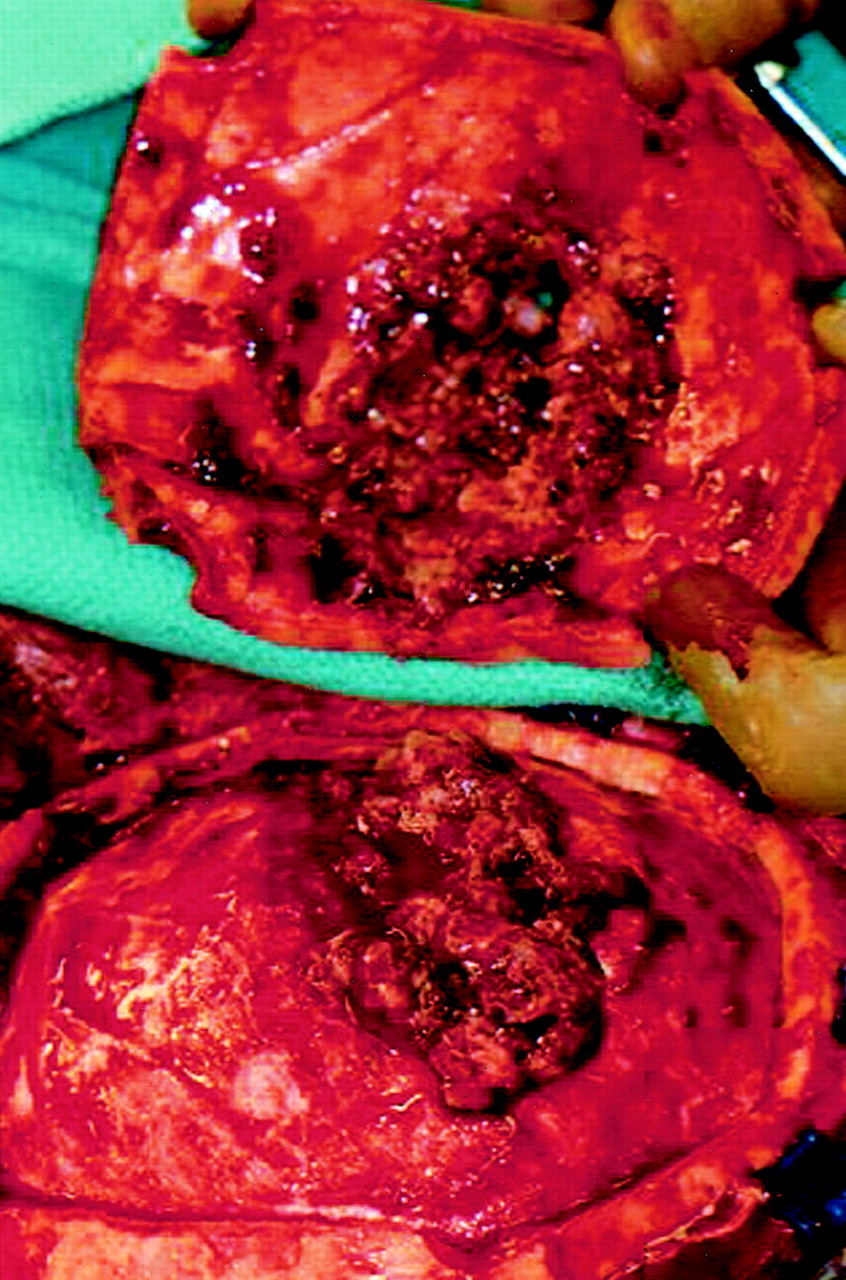
Epidural tumor leaving the dura macroscopically intact without substantial dural adherence.
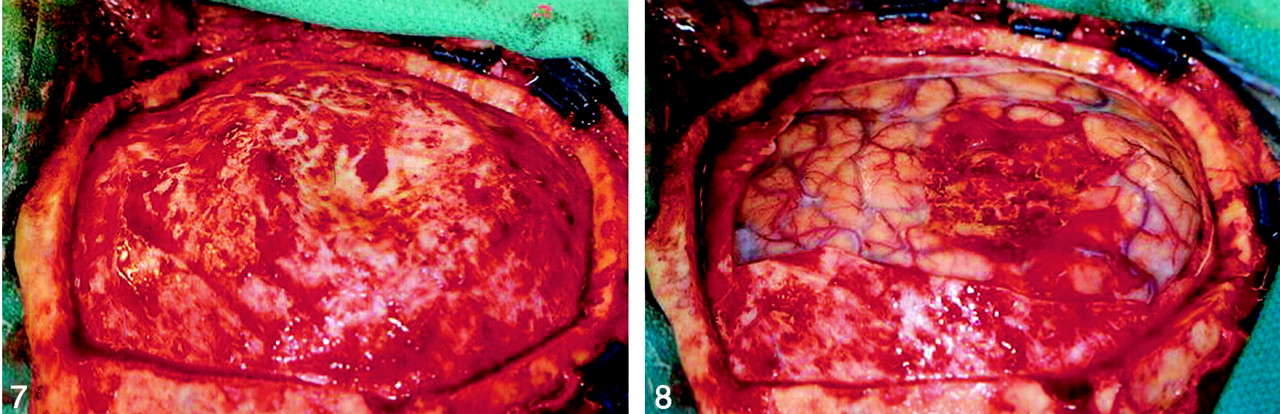
Macroscopically intact dura after the epidural portion of tumor was removed.
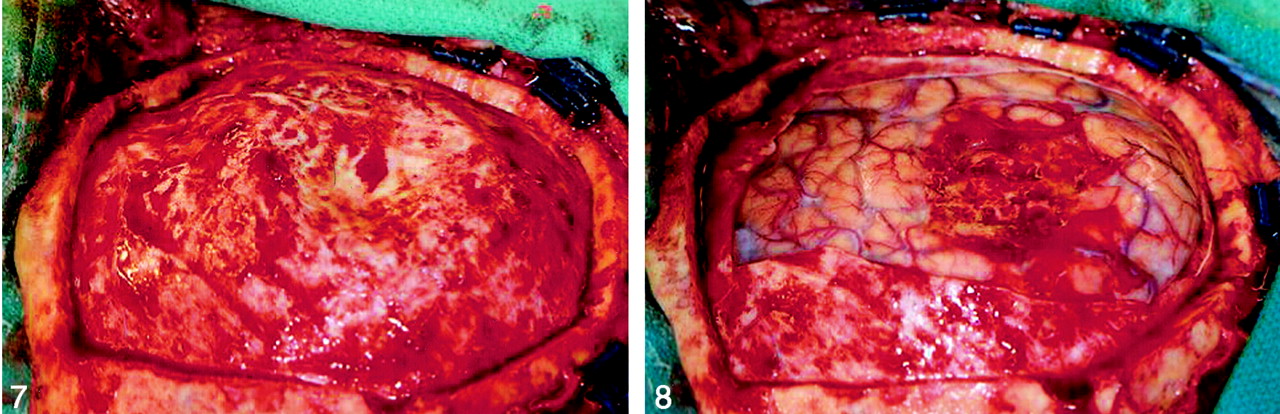
Intracerebral component is visible and surrounded by normal cortex.
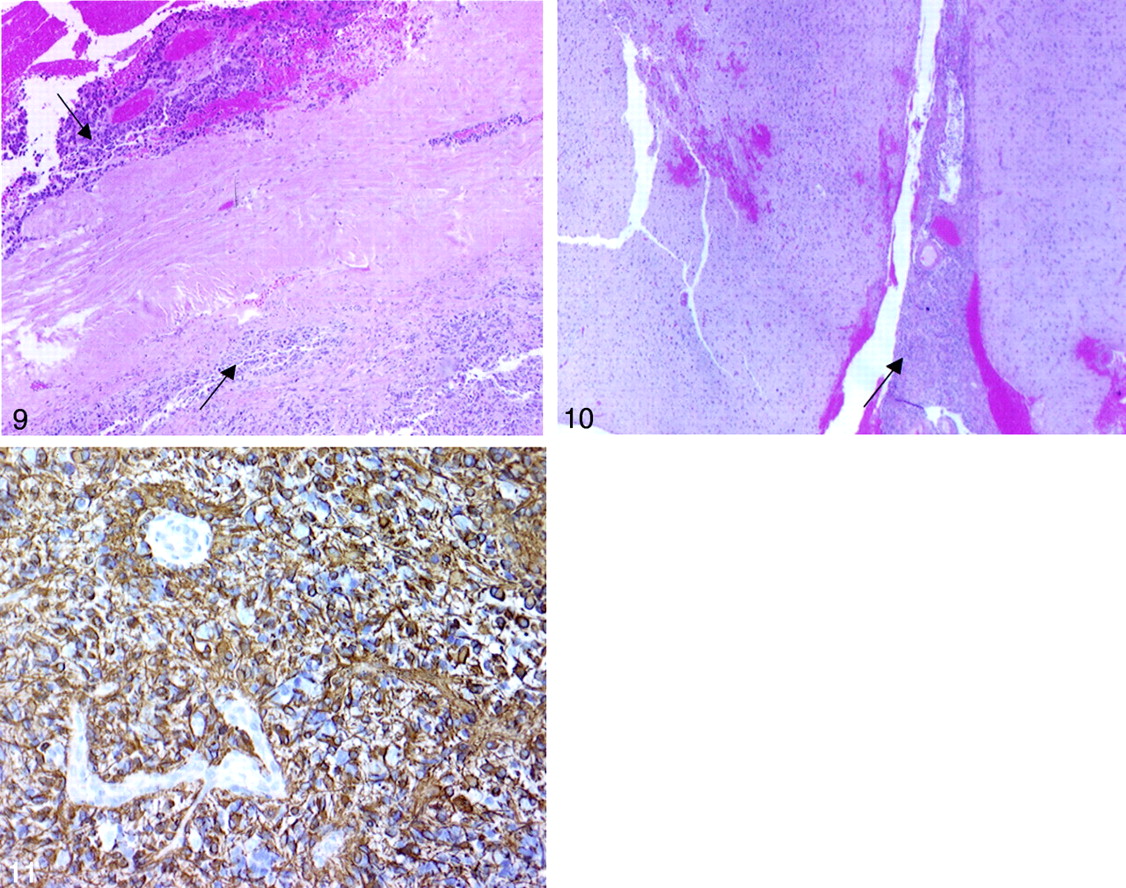
The histopathologic specimens demonstrated microscopically disrupted dura (Fig 9) with destruction of the calvaria (Fig 10). Initial assessment of the specimens included lymphoma and small cell cancer in the differential diagnosis. To clarify the origin of this tumor, immunoperoxidase stains were performed on all tumor specimens. This tumor was positive for antibodies against CD56, GFAP, and S100 (Fig 11). The tumor did not stain with HMB45, chromogranin A, or pancytokeratin. Therefore, the diagnosis of GBM, without sarcomatous changes, was made on all resection areas.

Right parietal dura with tumor (arrows) on both sides of the dura (original magnification ×40).

Right parietal intracerebral tumor (arrow). Image shows the GBM arising in the brain and growing outward as a mass outside the brain that penetrated the dura and the skull (original magnification ×20).
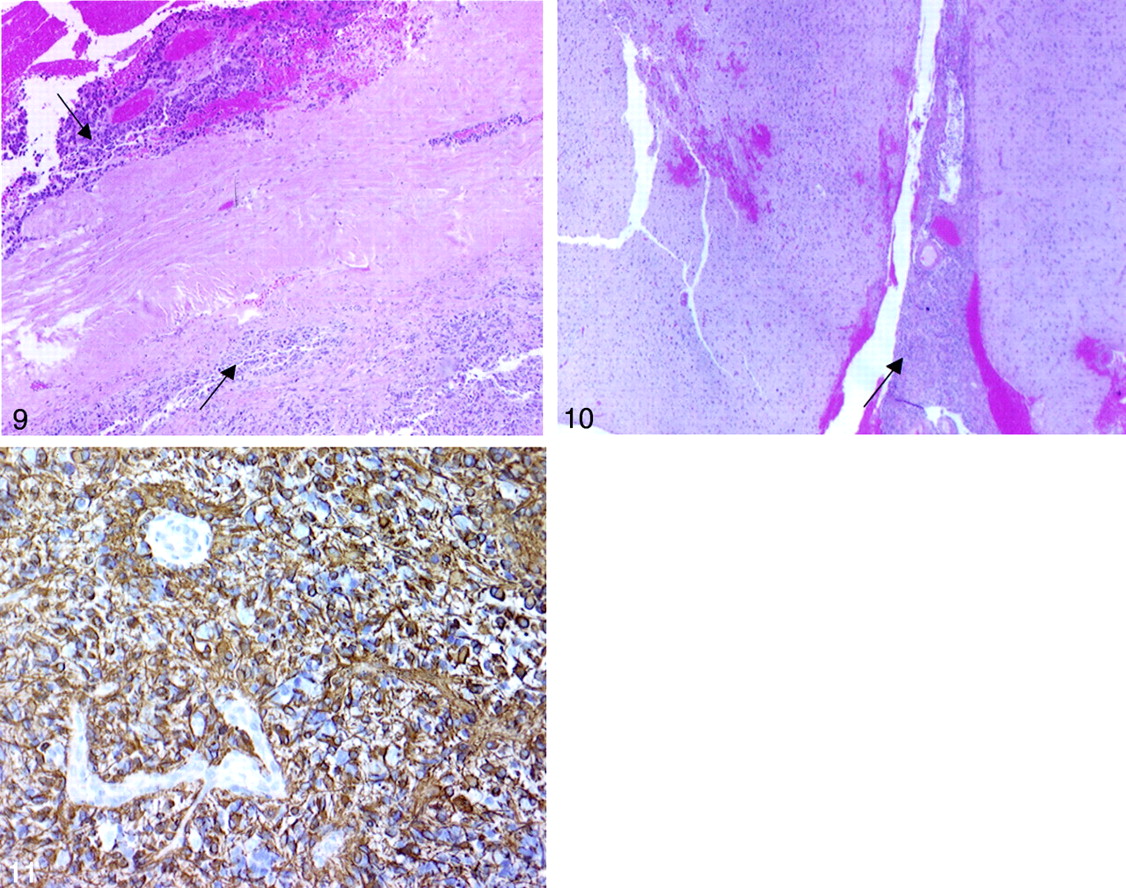
Right parietal tumor shows positivity for immunoperoxidase staining against GFAP (original magnification ×40).
Long-Term Follow-up
The patient experienced improved but persistent neurologic deficits postoperatively. Both chemotherapy and radiation therapy were contemplated. Chemotherapy was declined because of the patient’s worsening renal function and other concomitant ailments, and radiation therapy was initiated on postoperative day 30. Six weeks of external-beam radiation therapy was applied to the gross tumor volume.
The patient had persistent symptoms and was readmitted for evaluation of continued neurologic complaints on postoperative day 95. MR imaging performed on admission demonstrated two new lesions: one in the right temporal region and the other involving the ipsilateral high parietal region. Adjacent calvarial destruction was noted at both sites. Additional surgery, radiation therapy, and chemotherapy were declined. The patient entered home hospice care and died on post-operative day 143.
Discussion
Primary high-grade gliomas as a cause of skull erosion and destruction are exceedingly uncommon (1). Superficial slow-growing astrocytomas or oligodendrogliomas can cause inner table remodeling and or erosion related to chronic mass effect (2). It is rare for high-grade gliomas to invade and destroy the bone.
Most of the literature on GBM causing calvarial destruction comes from isolated case reports. Harwood-Nash and Fitz (3) described skull erosions on skull radiographs secondary to parietal GBM. Nager (4) reported two cases of GBM involving the temporal bone. Woodruff et al (1) described a case of frontotemporal GBM invading the temporal bone. In their case, CT results were misleading because of the presence of calvarial destruction. However, MR imaging showed the intraparenchymal extent of the mass, establishing the intracerebral site of tumor origin. This case is similar to ours, wherein CT showed impressive calvarial destruction, and the exact intra-axial or extra-axial location was not confirmed. Inward dural displacement suggested an extra-axial location favoring meningioma, metastasis, or lymphoma. MR imaging was useful in delineating the exact extent and helped in adding GBM as a possible cause.
Calvarial destruction with preexisting glial tumor has been described in the presence of prior surgery and irradiation, often along iatrogenic violations of natural barriers to tumoral growth (5–11). This case is unusual for two reasons. First, the GBM involved both the brain parenchyma and skull without antecedent radiation or surgery. Second, the lesion traversed the dura without radiologic or gross interruption of the dura. Microscopic invasion is then implicated, allowing glial cells to invade and destroy the overlying bone and galeal tissues. It is far more common for meningiomas, metastases, or sarcomas to cause direct involvement of the skull with accompanying destruction of the dura, given that the dura is believed to normally provide a barrier against invasion (12). Figure 9 demonstrates microscopic evidence of dural invasion.
Conclusion
Calvarial destruction in association with extra- and intra-axial neoplasm should include GBM in the differential diagnosis, although this is rare. While imaging findings may include GBM in such cases, the final diagnosis is established by means of pathologic examination.
References
- Received December 15, 2003.
- Accepted after revision January 23, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}