
Abstract
Summary: Heterotopic brain presenting as a giant, growing, single locular cyst at the parapharyngeal space has not been reported before, to our knowledge. We present such a case, with MR imaging findings, in a 13-month-old girl. A well-demarcated giant cystic mass was noted in the left parapharyngeal space from the skull base to the submandibular region. Airway compression and deformity of the left mandible with subluxation of the temporomandibular joint were noted. The cyst contained a clear fluid that was isointense to CSF with all pulse sequences. Wall enhancement was noted on contrast-enhanced T1-weighted images. No connection to intracranial structures was noted. Histologic findings were compatible with neuroglial heterotopia.
Neuroglial heterotopia, heterotopic brain, or differentiated neural tissue outside the cranial vault is uncommon, and these anomalies most commonly occur in the nasal cavity (1, 2). Neuroglial heterotopia in the parapharyngeal space has rarely been reported (3–5). Previous reports of these cases have shown only CT images of neuroglial heterotopia presenting as a low-attenuation mass with some area of focal cystic formation (3–5). We herein present the MR imaging findings of a parapharyngeal neuroglial heterotopia presenting as a giant, growing, single locular cyst in a 13-month-old girl.
Case Report
A 13-month-old girl was noted by her mother to have a growing left lower facial mass and asymmetrical jaw. The mass widened and softened and compressed the lower gingiva. Snoring when she was sleeping was noted. No neck stiffness and no upper respiratory tract infection had been noted in the few days before presentation. Her mother mentioned that the little girl had a cystic lesion in the head and neck area at birth. The infant was born at another hospital.
On this admission, MR imaging of head and neck revealed a thin-walled cystic lesion, measuring 32 × 57 × 47 mm, in the left parapharyngeal space at the oropharyngeal and nasopharyngeal levels, and extending inferiorly to the left submandibular space (Fig 1A–D). No solid part or internal septation was seen within this cyst, and mild enhancement was noted along the wall after gadolinium administration. The mass caused the mild deformity and deviation of the left mandible and masticator muscles anteriorly and associated subluxation of the left temporomandibular joint. The airway at the pharyngomucosal space was compressed and stenosed, but the fat planes between the constrictor muscles and cystic wall appeared intact. At the submandibular level, the cystic mass displaced the left submandibular gland medially and stretched the left digastric muscles posteriorly and laterally. No communication between the cyst and the intracranial structures was noted.

Thirteen-month-old female infant with neuroglial heterotopia in the parapharyngeal space.
A and B, Axial T1-weighted MR images before (A; TR, 450 ms; TE, 11 ms) and after (B; TR, 566 ms; TE, 11 ms) gadolinium administration at the oropharynx level. A huge, thin-walled cystic lesion is noted in the left parapharyngeal space, obliterating the normal parapharyngeal fat associated with compression and narrowing the oropharynx air column. The cyst displaces the carotid space posteriorly, the masticator space anteriorly and laterally, and the parotid space laterally. There is a thin fat plane (white arrows) seen between the parotid gland and the lesion, excluding the possibility of a lesion from the deep lobe of parotid gland. Note the parapharyngeal triangular fat clearly identified on the contralateral side (black arrow). Mild enhancement is seen along the wall of the cyst after gadolinium administration (arrowhead).
C and D, Axial T2-weighted MR images at a lower level (C; TR, 3000 ms; TE, 56.7 ms) and coronal T2-weighted (D; TR, 4800 ms; TE, 47.7 ms) images. The cyst appears to have no septum and no mural nodule or focal wall thickening. The cystic contents are isointense to CSF for all pulse sequences. The left mandibular arch is eroded, thinner and deformed when compared with the contralateral side (arrow). No communication between the cyst and intracranial structures is noted. The skull base over the left middle cranial fossa is intact.
The initial diagnosis was cystic hygroma. The patient then received total excision of the cystic mass, facial deformity reconstruction, and prevention of airway obstruction by a left submandibular approach. During surgery, a large cystic mass filled with clean fluid over the left parapharyngeal space was noted. The mass adhered strongly to the surrounding tissues.
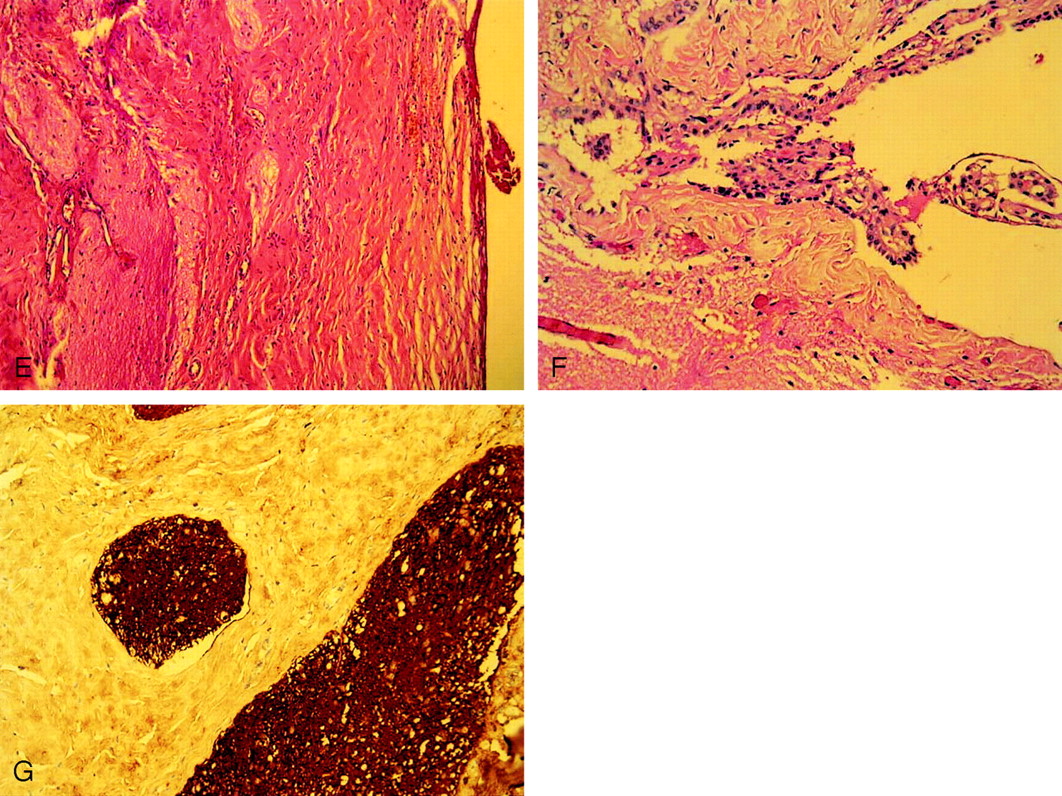
Grossly, the specimen appeared brownish and soft to elastic. When cut, a collapsed cystic lesion with a smooth inner wall in the soft tissue was noted. On microscopy, serial sections showed neuroglial heterotopia in soft tissue composed of neuroglial tissues embedded in the fibrous wall of the cyst (Fig 1E). Some ependymal cells and choroid plexus-like elements on the dense fibrous cystic wall were also noted. The neuroglial tissue was positive for glial fibrillary acid protein (GFAP), and the choroic plexus-like cells were positive for cytokeratin in a few cells on immunohistochemical study (Fig 1F and G). No meningeal lining was identified. Two weeks after resection, clinical follow-up revealed no evidence of complications.
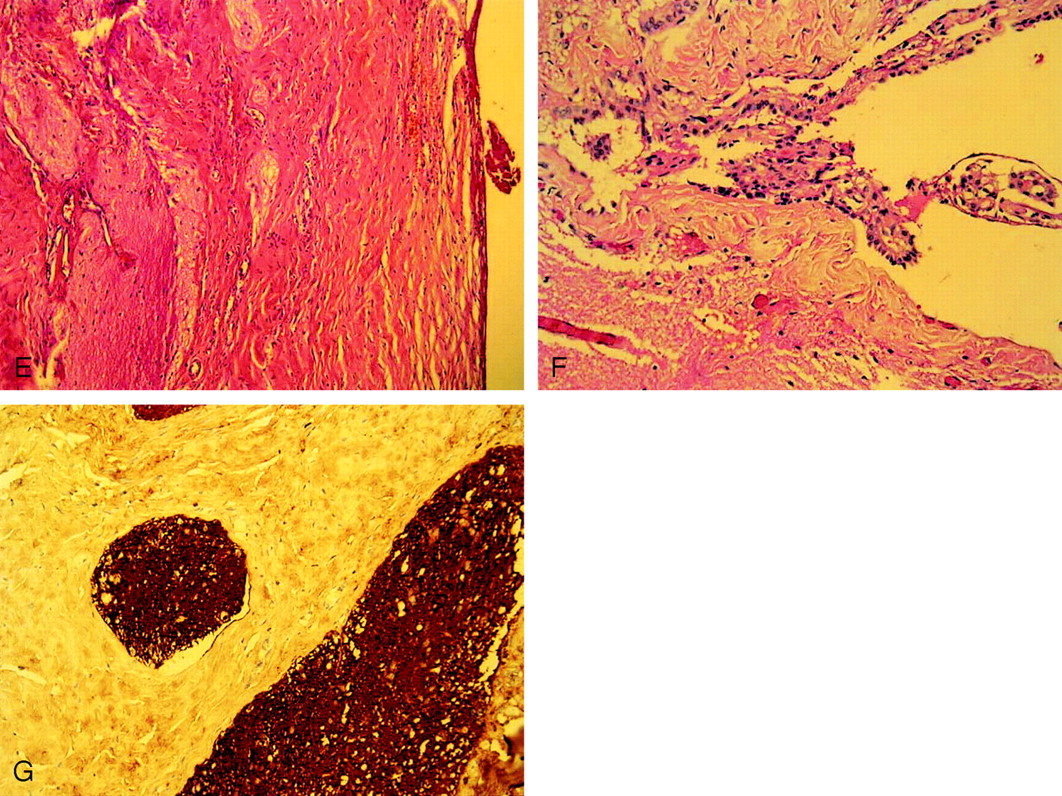
E, Islets of mature neuroglial tissue are noted in the fibrous tissue of cyst wall (H&E, original magnification ×100).
F, Choroid plexus-like tissue is noted in the inner wall of cyst (H&E, original magnification x200).
G, The mature neuroglial tissues are strongly staining for GFAP by immunohistochemical stain (original magnification ×200).
Discussion
Neuroglial heterotopia has been defined as a mass composed of mature brain tissue isolated from the cranial cavity or spinal canal (6). This anomaly can occur in the nasal cavity (1), scalp (7), orbit (8), pterygopalatine fossa (9), pharynx (10, 11), palate (12), lips (13), tongue (14), middle ear region (6) and even lung (15). More than 140 cases of nasal heterotopic brain (misnamed nasal glioma) (1, 2) have been described, but fewer than 20 cases of its counterpart at the parapharyngeal space have been reported (2–5).
Parapharyngeal neuroglial heterotopia is usually found in neonates with clinical manifestations of airway obstruction, feeding difficulty, and a neck mass (3–5). This anomaly seems to have a left side and female predominance in previously reported cases (3–5), as in our case. Other associated developmental anomalies have been reported, such as cleft palate, Pierre-Robin syndrome, and congenital heart disease (3–6). Unlike meningoencephaloceles, brain heterotopias lack connection with the subarachnoid space (6).
Neuroglial heterotopia usually consists of neuroglial elements, but it may contain elements of choroid plexuses. In general, growth of heterotopic brain parallels growth of normal tissue, and in some cases the lesion is cystic, owing to the presence of a functional choroid plexus (2), but growth can overtake that of normal tissue, as in our case. Patients with cystic lesions may have acute respiratory distress when the airway is compressed, or facial deformity due to the pressure erosion, but it is less common with solid lesions (2, 11, 15–18).
CT and MR imaging are complementary studies that are necessary in preoperative planning to determine the extent and location of a mass. On CT scans, a heterogeneous hypoattenuated mass with or without a cyst is a common feature (1, 16). On MR images, neuroglial heterotopia or heterotopic neuronal tissue usually has signal intensity characteristics similar to brain on T1-weighted, proton density-weighted, and T2-weighted images. It may be hyperintense on T2-weighted images because of dysplastic neural tissue (10, 12). Heterotopic brain containing functioning choroid plexus elements may present as a cystic mass because of production of CSF. It may enhance depending on the vascularity or presence of choroid plexus (2, 15, 18). An important role of MR imaging is to exclude communication with the adjacent brain tissues in order to distinguish neuroglial heterotopia from encephalocele; differentition can easily be achieved with sagittal or coronal imaging.
Pharyngeal neuroglial heterotopia usually appears as a large-mass lesion with heterogeneous attenuation and no intracranial connection (3–5). In comparison to their nasal counterpart, focal cyst formation and calcification are not uncommon and two reported cases have appeared as a multicystic mass (4). These lesions can be located superiorly in the skull and inferior to the clavicle level, with a varied degree of mass effect to adjacent structures. In addition, erosion of the floor of the middle cranial fossa is a suggestive characteristic (5). In our case, heterotopic brain presenting as a growing, giant single locular cyst without obvious solid parts or septation at the parapharyngeal space has not been reported before. The signal intensity of thin wall, as compared with that of brain tumors, appeared hypointense on both T1- and T2-weighted images and obvious enhancement on gadolinium-enhanced T1-weighted images. It can be explained by dense fibrosis of the wall, which also contained functioning choroid plexus and vascularity, as documented on our histologic findings. We proposed that the large amount of CSF production by functioning choroid plexus expands the small amount of heterotopic neuroglial tissue and reacts to cystic pressure with fibrosis and vascularity. Dense fibrosis of the wall with vascularity, which was confirmed on the basis of pathologic examination, was formed after tissue reaction to cystic pressure. Bone erosion of the left skull base and deformity of the left mandible and temporomandibular joint due to mass effect were also well delineated.
On pathologic examination, pharyngeal heterotopic neuroglial tissue may contain neurons and astrocytes, as well as more complex CNS elements such as ependymal-lined structures, a functioning choroid plexus, and pigmented cells of retinal differentiation (5, 6), as documented in the histologic findings of our case. The neural elements are typically embedded in fibrous tissue and may exhibit calcification. Rare instances of neoplasm, including oligodendroglioma and neuroectodermal tumor, within excised lesions have been reported (19, 20).
The parapharyngeal space is a fat-containing space surrounded by pharyngeal mucosa, masticator, parotid, carotid, and retropharyngeal spaces. Only vessels, lymph node, nerves, and some ectopic minar salivary glands are seen in the area. To approach a parapharyngeal space lesion, the first step is to differentiate it from more common, deep-lobe parotid lesions to determine the appropriate surgical approach (21). MR imaging can distinguish this by revealing the fat plane between the normal parotid gland and a mass arising within the parapharyngeal space, as shown in our case.
The differential diagnosis of a parapharyngeal tumor is limited and includes schwannoma and minor salivary gland tumors (21). These tumors can undergo cystic degeneration but complete cystic change presenting as an even, thin wall is very rare; these lesions usually occur in adults. Large cystic masses in the parapharyngeal region are rare in the neonate. Most common differential diagnoses include cystic hygromas, encephaloceles, meningoceles, teratomas, branchial cleft cysts, and giant diving ranulas. In contrast to an encephalocele or meningocele, parapharyngeal neuroglial heterotopia has no intracranial communication. Teratoma appears to have a variety of contents in addition to the cystic, including fat and calcification (22). Branchial cleft cysts in the parapharyngeal space are also unilocular but tend to have a much thicker cyst wall and thicker contents with cholesterol crystals and are usually confined at the nasopharynx or oropharynx (23, 24). The characteristics of cystic hygromas include multiple cysts with relatively well-demarcated margins and extremely high signal intensity on T2-weighted images with fluid-fluid levels of higher signal intensity in the upper layer and displacement rather than infiltration of muscle (25). In younger adults, a giant ranula may attain very large dimensions by gross involvement of the submandibular and parapharyngeal spaces. These lesions are unilocular, smooth, well-defined, fluid-filled, nonenhancing masses (26). They are, however, usually centered in the submandibular space and involve the sublingual space with smooth a tapered tail. The submandibular gland is always displaced laterally (26).
The treatment of heterotopic brain tissue is complete surgical excision; recurrence as a result of incomplete excision has been described (5). Although focal areas of immature cells have been reported (19, 20), these masses lack invasive patterns and are not true neoplasms.
Before surgery, it is difficult to differentiate the neuroglial heterotopia from lymphangioma in cases such as ours. The only clue is a giant single locular (as in our case) rather than multiseptated cyst, which can be commonly seen in lymphangioma; however, heterotopic neuroglial tissue presenting as a giant single locular cyst has not been reported before. Another way to differentiate these two entities is the laboratory study of the fluid. Therefore, we can differentiate neuroglial heterotopia from meningoencephalocele easily whenever the neuroglial tissue has been excised, and the clue is that no intracranial connection is seen, as in our case.
Surgical intervention is necessary in patients with heterotopic parapharyngeal neuroglial tissue that causes airway distress, dysphagia, or failure to thrive (3–5). The timing of surgery is controversial. Proponents of delayed resection believe that resection might be safer in the older child, in whom vital neurovascular structures are more easily salvageable and blood volume is greater (3–5).
Conclusion
Radiographic assessment of parapharyngeal heterotopic neuroglial tissue is best performed by using MR imaging in multiplanar views, complemented by CT. When a large parapharyngeal cystic mass and skull base erosion in a female neonate has been encountered, especially over the left side, neuroglial heterotopia should be included in the differential diagnosis. MR images are useful not only in identifying the heterotopic neural tissue extension, but also in excluding associated cranial defects and direct communication with the brain; thereby, they can be helpful for choosing the less hazardous surgical plane.
References
- Received March 18, 2004.
- Accepted after revision March 25, 2004.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}