
Abstract
Summary: Leiomyoma is a rare tumor arising from the uveal tract. Fundoscopically, it appears as a yellowish-white, elevated mass and cannot be readily distinguished from melanoma or other uveal tumors. Cross-sectional imaging may have an important role, particularly when the opaque ocular media or a vitreous hemorrhage precludes a clear ophthalmoscopic view. In this respect, radiologists should be aware of suggestive findings of uveal leiomyoma to avoid an incorrect diagnosis and unnecessary radical surgery. We report MR imaging findings of three cases of uveal leiomyoma.
Leiomyoma of the uveal tract (UTL) is a rarely encountered disease entity in clinical practice. UTL is a yellowish-white, highly vascularized elevated mass on ophthalmoscopic examination. Because of similar appearances, malignant melanoma (especially amelanotic type), metastasis, or other unusual tumors cannot be differentiated from UTL only by ophthalmoscopic examination. In addition to this limitation, an obstacle to thorough ophthalmoscopic examination, such as opaque ocular media or vitreous hemorrhage, may lead a physician to perform the cross-sectional imaging. To the best of our knowledge, however, radiologic findings of UTL have not been reported previously in the radiologic literature. Therefore, until now, cross-sectional imaging has contributed little to making a proper differential diagnosis in practice. At our institution, we encountered three UTL cases with MR imaging over the past 4 years.
Case 1
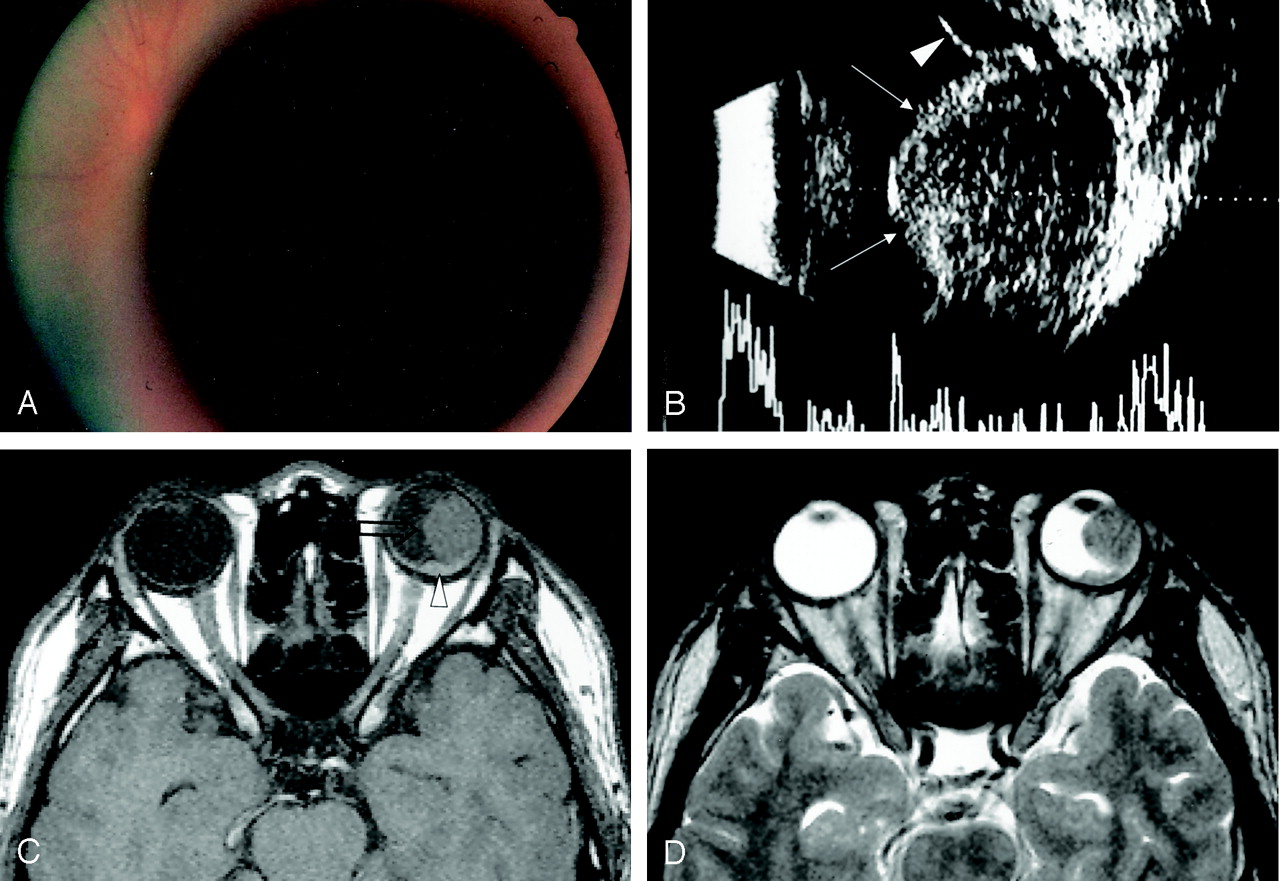
A 24-year-old man visited our institution for the evaluation of a sudden decrease in left visual acuity that developed 3 days earlier. Visual acuity was 20/20 on the right, and only hand-motion detectable at a distance of 30 cm on the left. Fundoscopy and ultrasonography showed a large circumscribed mass with subretinal effusion (Fig 1A and B). MR images revealed a well-circumscribed fungating mass involving the temporal ciliochoroidal region and some posterior choroid (Fig 1C–E). The epicenter of the tumor was the ciliochoroidal region or the peripheral choroid, and it was isointense to brain on T1- and T2-weighted spin-echo images. Gadolinium-enhanced T1-weighted images showed a strongly enhancing homogeneous mass. Our differential diagnosis was malignant melanoma and metastasis.

A 24-year-old man with sudden decrease of left visual acuity.
A, Fundus photograph shows a dark, large, circumscribed, view-obstructing mass.
B, Transocular sonography reveals a well-marginated endophytic mass with low internal reflectivity (arrows). Subretinal effusion is also observed (arrowhead).
C, The mass located at the ciliochoroidal region is large, protuberant, and isointense to brain on a precontrast T1-weighted axial image (open arrow). Small amount of subretinal hemorrhage is noted (arrowhead).
D, T2-weighted fast spin-echo axial image also shows an intraocular mass isointense to brain.
The left globe was enucleated. Gross pathologic examination revealed an oval-to-round bright whitish mass measuring 1.2 × 1.2 × 1.5 cm in maximal dimension. A low-power photograph of the globe was taken (Fig 1F). Microscopic examination revealed the tumor to be composed of spindle cells arranged in intersecting fascicles (Fig 1G). On immunohistochemical study, the tumor cells were immunopositive for the smooth muscle actin that is a marker of smooth muscle differentiation (Fig 1H). The final histopathologic diagnosis was leiomyoma of the ciliary body and choroid.

(continued) E, On gadolinium-enhanced T1-weighted axial image, a homogeneous, enhancing mass is seen at the ciliochoroidal region (open arrow), as is a small amount of nonenhancing subretinal hemorrhage around the posterior pole (arrowhead).
F, Low-magnification photograph of a cut specimen shows a well-circumscribed ciliochoroidal mass involving the whole stroma of the choroids (hematoxylin and eosin staining; magnification ×2). C indicates ciliary body; E, subretinal effusion; L, lens; N, optic nerve; and T, tumor.
G and H, Hematoxylin and eosin staining (G) shows spindle cells arranged in intersecting fascicles, and tumor cells that have cigar-shaped nuclei with blunted end (arrowheads). The chromatin pattern is vesicular and mitotic figures are not seen. The tumor cells are positively stained for smooth muscle-specific actin (H).
Case 2
A 20-year-old woman presented with an intraocular mass detected incidentally at a private ophthalmology hospital. Visual acuity was 20/100 on the right, and 20/100 on the left. Fundus examination of the right globe showed an orange-colored mass with localized retinal detachment. MR images showed a temporal, well-circumscribed ovoid mass, which involved the ciliochoroidal region of the globe. As in case 1, the mass was isointense to brain on T1- and T2-weighted images and showed strong homogeneous enhancement on gadolinium-enhanced T1-weighted images. The differential diagnosis included, in order, amelanotic malignant melanoma, metastasis, and other unusual tumors of the uvea.
Choroidal mass excision and cryotherapy were performed. The tumor size was about 1 cm. It appeared yellow and brownish and fragile. The tumor specimen was divided into two pieces, measuring 1.5 × 1.4 × 0.8 cm and 1.1 × 1.0 × 0.5 cm in maximal dimension. On the microscopic examination, the tumor was composed of spindle cells arranged in intersecting fascicles. Immunohistochemical studies demonstrated immunoreactivity of tumor cells for the desmin and smooth muscle actin. The final pathologic diagnosis was UTL.
Case 3
A 35-year-old woman presented with progressive decline of left visual acuity over a period of 4 months. Visual acuity was 20/40 on the right and only finger countable at a distance of 30 cm on the left. Fundus examination of the left eye showed a brownish choroidal mass with retinal detachment. Ultrasonography disclosed a hyperechoic choroidal mass with total retinal detachment. MR imaging showed a well-circumscribed elliptical mass involving the ciliochoroidal region and some posterior choroid. MR imaging signal intensity and the enhancement pattern of the mass were similar to the previous cases. The differential diagnosis included, in order, amelanotic melanoma, metastasis, and other benign tumors such as hemangioma.
Scleral dissection and incisional open biopsy of the intraocular mass were performed. On microscopic examination, the tumor was composed of spindle cells arranged in intersecting fascicles. The cells had fibrillary eosinophilic cytoplasm. Immunohistochemical studies demonstrated immunoreactivity of tumor cells for the vimentin and smooth muscle actin. The tumor cells were focal positive for desmin and negative for S-100 protein and melanoma-specific antigen (HMB-45). Pathologic diagnosis was UTL. Finally, tumor excision and cryotherapy were performed. The tumor was 1.0 × 0.8 × 0.5 cm in maximal dimension.
Discussion
The appropriate clinical diagnosis determined by using various diagnostic tools in ophthalmology does not always require further imaging studies, including CT or MR imaging, particularly for intraocular lesions. CT or MR imaging may help in the diagnosis or management of an intraocular disease when the opaque ocular media precludes a clear view or when vitreous hemorrhage and subretinal effusion obscure ophthalmoscopic viewing. Recognizing the intraocular lesion as melanoma is important with its invasiveness, because it determines whether a treatment plan such as local globe maintenance therapies (local excision, brachytheraphy, or percutaneous irradiation) or radical therapies (enucleation or exenteration) should be used for a uveal mass (1). But other uveal tumors cannot be readily differentiated from uveal melanoma, especially amelanotic tumors, even if they are rare or less common in incidence (2).
Clinically, UTLs are difficult to differentiate from amelanotic uveal malignant melanomas, which are revealed as protuberant masses on ophthalmoscopic examination (3). In a few case series, however, some clinical and pathologic characteristics have been reported that might serve to differentiate UTLs from melanomas (3, 4). UTLs tend to occur in younger patients and also have a predilection for female patients. They affect the ciliary body and peripheral choroids, rather than the posterior choroid, and involve the supraciliary or suprachoroidal space in terms of location of the globe wall stratification. By contrast, uveal melanomas are less likely to occur in the peripheral choroid or ciliary body and involve the uveal stroma in the globe wall (5). On transillumination, UTLs usually transmit light readily, whereas most melanomas cast a shadow (4). In our three cases, two patients were female and age ranged between 20 and 39 years. In all three cases, the UTL was located in the ciliochoroidal region, was protuberant in shape, and was isointense to brain on both T1- and T2-weighted sequences. UTLs were strongly enhanced with gadolinium injection. These MR imaging features and the location of the UTL may reduce the number of the differential diagnoses, in that 1) choroidal metastasis is usually seen with diffuse outline in shape in the choroid posterior to the equator of the globe (6); 2) choroidal hemangioma in a solitary circumscribed form is reddish orange on ophthalmoscopic examination, is mainly located in the posterior choroids (6), and is hyperintense on fast spin-echo T2-weighted images relative to vitreous matter (7); 3) uveal nevus is the most frequently seen in the posterior third of the choroid, is flat in shape, and is for the most part <5 mm in basal diameter (8); 4) melanocytoma is deeply pigmented on fundoscopic examination and usually occurs at the optic disk (9); and 5) choroidal osteoma appears as a platelike calcified thickening of the posterior choroid, typically in the juxtapapillary region (10). Nevertheless, other uveal tumors—including schwannoma, neurofibroma, medulloepithelioma, or even amelanotic melanoma—cannot be differentiated from UTL even by both clinical and imaging examinations.
Conclusion
UTL tends to occur in the ciliochoroidal region and to appear as a protuberant mass that is isointense to brain on T1- and T2-weighted MR images. UTL should, therefore, be included in the differential diagnosis when a protuberant mass that is isointense to brain is seen in the ciliochoroidal region.
References
- Received March 6, 2004.
- Accepted after revision April 9, 2004.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.