
Abstract
BACKGROUND AND PURPOSE: The role of diffusion tensor imaging (DTI) in neurosurgical planning and follow-up is currently being defined and needs clinical validation. To that end, we sought correlations between preoperative and postoperative DTI and clinical motor deficits in patients with space-occupying lesions involving the corticospinal tract (CST).
METHODS: DTI findings in four patients with masses near the CST and not involving motor cortex were retrospectively reviewed and compared with contralateral motor strength. CST involvement was determined from anisotropy and eigenvector directional color maps. The CST was considered involved if it was substantially deviated or had decreased anisotropy. Interpretations of the DTIs were blinded to assessments of motor strength, and vice versa.
RESULTS: Of the four patients with potential CST involvement before surgery, DTI confirmed CST involvement in three, all of whom had preoperative motor deficits. The patient without CST involvement on DTI had no motor deficit. After surgery, DTI showed CST preservation and normalization of the position and/or anisotropy in two of the three patients with preoperative deficits, and both of those patients had improvement in motor strength. The other patient with preoperative deficits had evidence of wallerian degeneration on DTI and had only equivocal clinical improvement.
CONCLUSION: Preoperative CST involvement, as determined on DTI, was predictive of the presence or absence of motor deficits, and postoperative CST normalization on DTI was predictive of clinical improvement. Further study is warranted to define the role of DTI in planning tumor resections and predicting postoperative motor function.
Diffusion tensor imaging (DTI) is a potentially valuable tool for preoperative planning (1–11) and postoperative follow-up (12) of surgically treated brain tumors and vascular malformations. The goal of surgical treatment is to maximize the extent of tumor resection while minimizing postoperative neurologic deficits resulting from damage to intact, functioning brain. This outcome can be facilitated by preoperative mapping of the tumor and its relationship to functional structures, including cerebral cortex and white matter (WM) tracts. Although cortical mapping can be accomplished preoperatively with functional MR imaging, only DTI is able to map the relationship of tumor with functional, connective pathways in the WM. Because axonal fibers and their myelin sheaths limit the diffusion of water molecules in a directionally dependent (ie, anisotropic) fashion, the directional analysis of diffusion by DTI enables WM tracts to be mapped noninvasively and provides a means to characterize tumor-related alterations of tissue microstructure (2, 3, 13).
The role of DTI in preoperative planning and postoperative follow-up is currently being defined. Most of the published experience in this area has been limited to isolated case reports and demonstrations in small numbers of patients (1, 4, 6–9, 12, 14). Typically, some form of tensor directional mapping is used to depict the deviation of a fiber tract by tumor. Some investigators have integrated cortical mapping by using functional MR imaging with fiber tract mapping by using DTI, in some cases by using the results of the former to guide the latter (8, 10, 14). DTI-based fiber tract maps can provide confirmation that a tract in question remains intact and can inform the surgeon as to the location of the tract with respect to the tumor, possibly facilitating preservation of the tract at surgery (12).
Although results to date appear promising, further validation of preoperative DTI as a clinically relevant technique is still needed. Correlations with intraoperative findings (11) and clinical outcomes are relatively lacking. As a first step toward clinical validation, we retrospectively analyzed the preoperative and postoperative DTI appearances of the corticospinal tract (CST) in a series of patients with space-occupying lesions and compared them with the patients’ clinical motor function before and after surgical resection.
Methods
Patient Selection
Between August 2001 and October 2003, 55 patients with intracranial masses were preoperatively evaluated with DTI at our institution. Among them, nine patients were found to have potential CST involvement (mass near the cerebral peduncle, posterior limb of internal capsule [PLIC], or corona radiata) on conventional MR imaging. Five patients with concomitant involvement of the motor cortex, due to mass effect, edema or direct tumor involvement, were excluded, leaving four patients (patients 1–4) with lesions potentially involving only the CST (Table). These patients ranged in age from 20 to 46 years. Their lesions included two pilocytic astrocytomas, one ganglioglioma, and one cavernous angioma. The lesions were located in the region of the thalamus and/or basal nuclei in all patients.
Clinical motor findings and DTI-determined CST involvement
DTI and MR Imaging Studies
Preoperative and postoperative imaging was performed at 1.5 T by using a standard quadrature birdcage head coil (GE Medical Systems, Milwaukee, WI). The imaging protocol included conventional clinical sequences and DTI and was approved by the institutional review board at our institution. Time from preoperative imaging to surgery ranged from 2 to 15 days (mean, 8 days), and time from surgery to postoperative imaging ranged from 152 to 258 days (mean, 197 days).
DTI was performed by using a pulsed gradient spin-echo sequence with a single-shot echo-planar acquisition. Imaging parameters were TR/TE/NEX=4500/71.8/4, field of view=240 mm, section thickness=3 mm, matrix=128 × 128 zero-filled to 256 × 256, voxel size (before interpolation)=1.87 × 1.87 × 3.0 mm interpolated to a 0.94-mm isotropic voxel dimension. Diffusion encoding was performed in 23 uniformly distributed directions (15) with b=0 and 1000 s/mm2. DTI scanning time was approximately 7 minutes. Image distortion from eddy currents and misregistration from head motion were corrected by using image coregistration software with an affine warp model in Automated Image Registration (16). Image signal-to-noise ratio was improved by using a 3 × 3 in-plane spatial median filter. The diffusion tensors were decoded and diagonalized for each voxel location (15, 17). The spatial diffusion tensor information was represented by two parametric images: the fractional anisotropy (FA) (18) and the major eigenvector direction represented by using a red-green-blue color map weighted by FA (19). The latter map was critical to identification of the CST, the superior-inferior orientation of which resulted in a characteristic blue given the chosen color scheme.
Clinical Evaluation
All patients underwent detailed neurologic examinations before and after surgery. Time between physical examination and DTI ranged from 0 to 22 days (mean, 4 days). A senior attending neurosurgeon assessed their motor strength by using the Medical Research Council scale of 0–5 (20), where 5 indicating that muscle contraction overcame full resistance; 4, muscle contraction was reduced but able to overcome some resistance; 3, muscle contraction was able to overcome only gravity; 2, muscle contraction occurred only when the force of gravity was eliminated; 1, muscle produced only trace movement or fasciculations; and 0, no muscle contraction was observed.
Motor findings were obtained from inpatient charts or outpatient clinic notes. The same physician, who was blinded to the DTI findings, assessed preoperative and postoperative motor findings in all patients. Scores that were reported between scale levels (eg, 4+ or 5−) were assigned to the lower value (ie, 4+ and 5−=4). The range of motor function was reported for both upper and lower extremities for each patient before and after surgery.
Image Analysis
A neuroradiologist (A.S.F.) with a certificate of added qualification who was blinded to the results of physical examination and surgical pathology determined CST involvement from anisotropy and directional color maps. The affected CST was compared with that of the unaffected, contralateral hemisphere. Involvement of the CST was considered present if any portion of the tract was substantially deviated (abnormal position with preserved anisotropy) and/or edematous, infiltrated, and/or gliotic (decreased anisotropy) (2, 3). No attempt was made to discriminate bland edema, tumor infiltration, and gliosis, as this remains an unsolved problem (2, 3).
Results
DTI-Determined CST Involvement
In the four patients with possible CST involvement and normal motor cortex before surgery, DTI confirmed CST involvement in three patients (Table). Of these three, patients 1 and 2 had substantial deviation of the PLIC, along with reduced anisotropy (Figs 1A–C and 2A–C), whereas the third (patient 3) had only a deviated PLIC (Fig 3A–C). The fourth, patient 4, had a preserved PLIC despite the presence of a striatal cavernoma primarily involving the anterior limb of the internal capsule and barely displacing the PLIC (Fig 4A–C

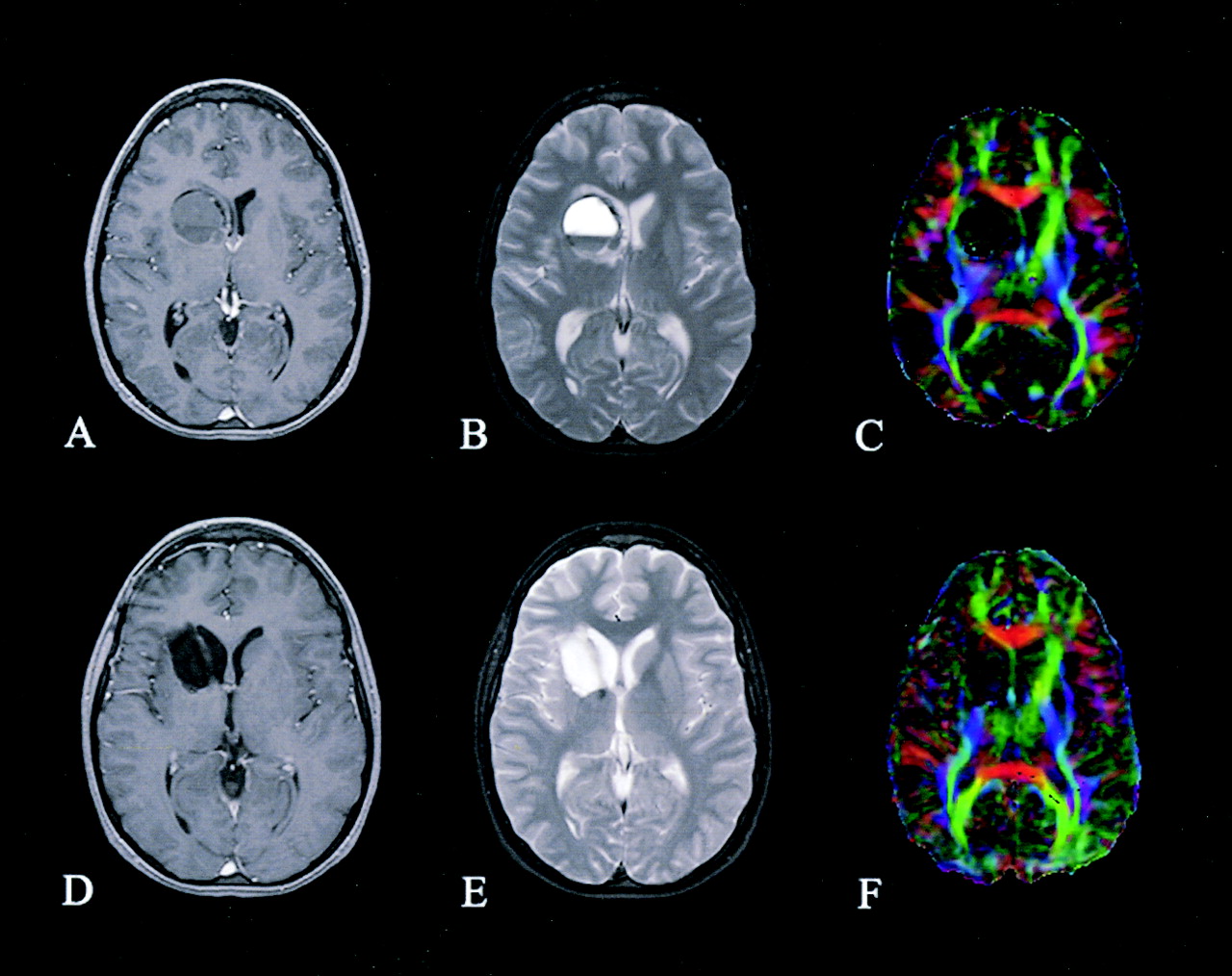
Patient 1. Preoperative (A–C) and postoperative (D–F) axial images of a right thalamic pilocytic astrocytoma: contrast-enhanced T1-weighted images (A and D), T2-weighted images (B and E), and directional color maps (C and F). Before surgery, DTI reveals decreased FA (diminished blue in C) and posteromedial displacement of the right PLIC (arrow in C). After surgery, DTI shows persistently decreased FA and displacement of the right PLIC (arrowhead in F).

Patient 2. Preoperative (A–C) and postoperative (D–F) axial images of a left frontal pilocytic astrocytoma: contrast-enhanced T1-weighted images (A and D), T2-weighted images (B and E), and directional color maps (C and F). Before surgery, DTI reveals decreased FA (diminished blue in C) and posteromedial displacement of the left PLIC (arrow in C). After surgery, DTI shows both restored FA (normal blue in F) and normal positioning of the left PLIC.

Patient 3. Preoperative (A–C) and postoperative (D–F) axial images of a left thalamic ganglioglioma: contrast-enhanced T1-weighted images (A and D), T2-weighted images (B and E), and directional color maps (C and F). Before surgery, DTI reveals lateral displacement of the left PLIC (arrow in C); after surgery, DTI shows that the position has returned to normal.

Patient 4. Preoperative (A–C) and postoperative (D–F) axial images of the right striatal hemorrhagic cavernous angioma: contrast-enhanced T1-weighted images (A and D), T2-weighted images (B and E), and directional color maps (C and F). Before surgery, DTI reveals only slight displacement of the right PLIC. After surgery, DTI shows a preserved right PLIC.
After surgery, DTI revealed CST preservation and normalization of position and/or anisotropy in two (patients 2 and 3) of the three patients with preoperative CST involvement (Figs 2D–F and 3D–F). Patient 1 continued to have substantial PLIC deviation with reduced anisotropy (Fig 1D–F). Although conventional T2-weighted imaging of the brainstem demonstrated only subtle blunting of the right ventral pons (Fig 5A and C) in patient 1, DTI revealed marked diminution of the right CST within the pons, consistent with wallerian degeneration (Fig 5B and D). In patient 4, who did not have preoperative CST involvement, the PLIC remained preserved and unchanged after surgery (Fig 4D–F).

Patient 1. Axial images of the brainstem. Before (A) and after (C) surgery, conventional T2-weighted images show subtle blunting of the right ventral surface of the pons (arrow). Preoperative (B) and postoperative (D) DTI reveals marked diminution of the CST in the right ventral pons, consistent with wallerian degeneration (arrowhead).
Correlation with Clinical Data
All three patients with DTI-confirmed preoperative CST involvement and normal motor cortex had preoperative motor deficits: a 2–4/5 left upper-extremity deficit, a 4/5 right-sided deficit, and a 3–4/5 right-sided deficit (in patients 1, 2, and 3, respectively). The patient (patient 4) without CST involvement on DTI had no motor deficit. In patients 2 and 3, in whom CST normalized, their hemiparesis completely resolved after surgery. Patient 1, who had persistent postoperative CST involvement with wallerian degeneration, had equivocal improvement in motor strength: Hemiparesis, which was rated 2–4/5 before surgery, was rated 2–5/5 after surgery. (Ranges reflect distal-to-proximal muscle groups.)
Discussion
The role of DTI in neurosurgical planning and postoperative follow-up is currently being defined. The depiction of WM tracts on DTI with directional color mapping is informative, esthetic, and highly useful to the neurosurgeon in certain preoperative planning situations, at least anecdotally. Nevertheless, the clinical utility of DTI in neurosurgical patients remains to be proved. The present study represented an attempt to validate preoperative and postoperative DTI findings by comparing them against findings on physical examination.
This is a challenging problem for at least two reasons. First, tumor-involved WM tracts may exhibit several different patterns of structural alteration on DTI, and these patterns are not yet completely understood (2, 3, 9). Second, no objective clinical measures exclusively correspond to any specific WM tract; rather, multiple functional structures, both cortical and subcortical, contribute to clinically relevant measures. We addressed the first problem by adopting a relatively simple, nonspecific criterion for tract involvement (i.e. the presence of either substantial deviation or reduced anisotropy without regard to cause, be it edema, gliosis, or tumor infiltration). We addressed the second problem by limiting the study to a tract (the CST) that is both readily identified on DTI color maps and associated with a readily measured function (motor strength). The potential for confounding involvement of the motor cortex was eliminated by carefully assessing this region on conventional MR imaging. Only four patients from an initial pool of 55 potential subjects satisfied these inclusion criteria; therefore, the results must be considered preliminary and in need of further validation.
Another limitation of the study was the use of DTI performed in the late rather than the immediate postoperative period. Given the high vulnerability of echo-planar imaging to susceptibility-related artifacts and the frequent presence of both air and blood products in the resection bed soon after surgery, we had limited success with early postoperative DTI and elected to use later scanning instead. Future studies may benefit from DTI acquisitions, such as the fast-spin-echo-based PROPELLER sequence, that do not rely on echo-planar imaging (21).
Anecdotally, neurosurgeons considered preoperative DTI highly useful in planning resection and in discussing the surgical risks with patients and their families. The most useful feature of DTI was the ability to preoperatively confirm the integrity of and to localize a markedly deviated tract. The frequency with which this information will affect a surgeon’s decision to operate or alter his or her surgical approach remains an open question that, as the present results suggest, is worthy of further study.
Conclusion
The appearance of the CST on DTI demonstrated excellent correlation with findings on clinical motor examination. In all patients, preoperative CST involvement determined on DTI was predictive of the presence or absence of motor deficits, and postoperative CST normalization on DTI was predictive of clinical improvement. These promising findings should be confirmed in a larger trial with rigorous outcomes analysis to more definitively validate the utility of DTI in planning tumor resection and predicting postoperative deficits.
Footnotes
Supported in part by National Institutes of Health grant R01-MH62015.
Presented in part at 42nd annual meeting of the American Society of Neuroradiology, Seattle, Washington, June 5–11, 2004.
References
- Received April 22, 2004.
- Accepted after revision July 30, 2004.
- American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Multimodal Imaging in Malignant Brain Tumors: Enhancing the Preoperative Risk Evaluation for Motor Deficits with a Combined Hybrid MRI-PET and Navigated Transcranial Magnetic Stimulation Approach
- Clinical significance of preoperative fibre-tracking to preserve the affected pyramidal tracts during resection of brain tumours in patients with preoperative motor weakness