
Abstract
Summary: We report the MR imaging findings in a 44-year-old man with a low-grade synovial sarcoma. There was a right-sided epidural and paravertebral mass, widening of the ipsilateral neural foramen at the L4–L5 level, and focal erosion of the right superior articular process of the L5 vertebra. The mass was relatively homogeneous, hyperintense to muscle and isointense to fat on T2-weighted images, and isointense to muscle on T1-weighted images, and it demonstrated moderate homogeneous enhancement.
Synovial sarcoma is a rare malignant neoplasm of soft tissue that arises near, but not in, a large joint (especially the knee) and most often occurs in an adolescent or young adult. It is typically slow-growing and may escape notice until it causes pain. On rare occasions, it is also encountered in the head and neck region, the chest, the abdominal wall, and the lower back (1, 2). We describe the MR imaging features of a synovial sarcoma that was located in the lower lumbar paravertebral space. Although the imaging features of a peripheral synovial sarcoma have been extensively documented, to our knowledge, there are few reports of such findings in patients with a paravertebral synovial sarcoma (3, 4).
Case Report
A 40-year-old man presented with a 7-month history of right-sided sciatica. On examination, he could walk without any support; however, he had grade III weakness of dorsiflexion of the right great toe and ankle and decreased sensation in the right L4 and L5 nerve territory. Findings of routine radiographs of the lumbar spine were normal. MR images (Fig 1) demonstrated a large right paravertebral and epidural mass displacing the thecal sac to the left at the L4-L5 level. The mass was connected through a slightly widened right neural foramen. The paravertebral mass showed a focal infiltration into the psoas and paravertebral muscle and smooth pressure erosion on the superior articular process of the L5 vertebra. It was relatively homogeneous, hyperintense to muscle and isointense to fat on T2-weighted images, and isointense to muscle on T1-weighted images, and it demonstrated moderate homogeneous enhancement on gadolinium-enhanced T1-weighted images. Because we suspected a neurogenic tumor, the patient underwent hemilaminectomy with facetectomy from L4 to L5. At surgery, the mass was located in the spinal epidural space and extended through the right L4 neural foramen into the space between the psoas muscle and the paravertebral muscle. Adhesions between the mass and the adjacent muscles were seen. After the tumor was nearly totally removed because of adhesion between the mass and the adjacent structure, we performed a vertebral fusion, using iliac bone.

A 44-year-old man with right low back pain.
T1-weighted (A, -B) (TR/TE/acquisition, 716/13/2) and T2-weighted (C) (TR/TE/acquisition, 4000/114/2) axial MR images show a large mass (asterisks) in the right paravertebral space at the L4-L5 level. It is isointense to muscle with T1 weighting (A, -B) and isointense to subcutaneous fat and hyperintense to muscle with T2 weighting (C). The mass infiltrates the adjacent structures (arrowheads) with focal erosion of the superior articular process of L5 (arrow). Ipsilateral neural foraminal widening and displacement of the thecal sac due to the epidural component are also demonstrated. Contrast-enhanced T1-weighted (D) (TR/TE/acquisition, 716/13/2) axial MR images reveal moderate homogeneous enhancement of the mass.
Microscopically, the tumor contained a characteristic combination of epithelial and spindle cell elements (Fig 2). The former appeared as well-formed glandlike spaces lined by cuboidal cells that simulated the histology of synovium. The sarcomatous component contained spindle cells with a fibroblast-like appearance. There was no evidence of tumor calcifications. Immunohistochemistry showed a strong reactivity for cytokeratin in the epithelial area, but not in the sarcomatous area. The spindle cells were strongly positive for vimentin and CD99, but negative for smooth-muscle actin, desmin, S-100 protein, synaptophysin, neurofilament, and chromogranin. The diagnosis was a low-grade biphasic synovial sarcoma. CT of the chest and abdomen showed no distant metastasis. The residual mass was treated with radiation therapy because the patient refused chemotherapy. There was improvement of his symptoms during the ensuing 5 months before the writing of this report.
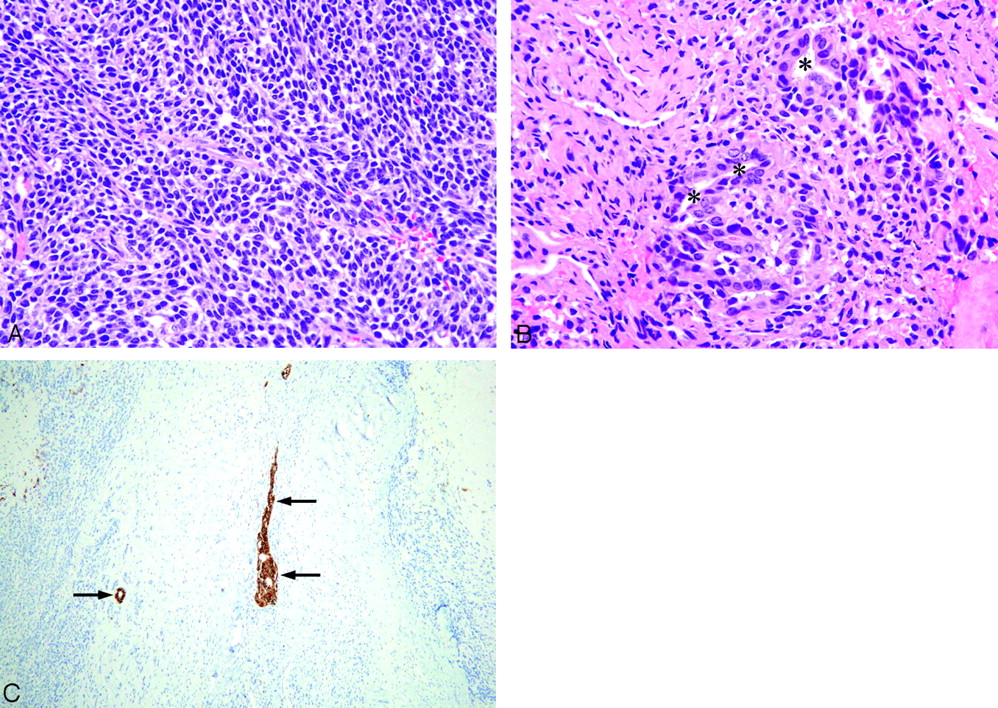
Histologic evaluation of low-grade biphasic synovial sarcoma involving the right paravertebral area with neural foraminal and spinal epidural extension.
A, The spindle cells of the tumor are uniform and relatively small, with ovoid pale-staining nuclei and inconspicuous nucleoli (hematoxylin and eosin, original magnification ×400).
B, The epithelial cells of the tumor have ovoid nuclei and abundant cytoplasm. They form glands with lumen (asterisks) (hematoxylin and eosin, original magnification ×400).
C, Immunohistochemistry for cytokeratin demonstrates the epithelial components of the tumor (arrows) (cytokeratin [AE1/AE3], ABC method, original magnification ×200).
Discussion
Synovial sarcomas comprise approximately 5%–10% of all soft-tissue sarcomas. They do not arise from the synovial membrane, but from undifferentiated mesenchymal tissues that then differentiate to a tissue similar to synovium (5). They can occur at any age, but most frequently affect young adults and adolescents (2) and are usually located in close proximity to a joint in the extremities, especially the knee. A minority of synovial sarcomas arise at unusual locations, such as the head and neck, chest wall, trunk, and retroperitoneal area (1, 2). A lumbar paraspinal location, as found in our patient, is rare (3, 4).
Synovial sarcoma occurs in 2 histologic subtypes: the biphasic type containing epithelial and spindle cell elements and the monophasic type containing only spindle cells (6). The chromosomal translocation t(X;18) has been considered as a specific cytogenetic chromosomal abnormality of synovial sarcoma. Molecular genetic studies have revealed that this translocation fuses 2 normal genes, SYT and SSX1 (or the related SSX2), to create an abnormal fusion protein. Recently, retrospective studies have shown that the presence of the SYT-SSX1 fusion transcript is correlated with a biphasic subtype of the synovial sarcoma, a higher proliferative rate, and a shortened metastasis-free survival (7).
In 50% of patients with synovial sarcoma, plain radiographic findings are normal; however, approximately 30% of patients have calcifications on plain radiography or CT. These are typically diffused punctate and often more concentrated at the periphery than at the center of the mass. Uncommonly, tumors can erode bone. In our patient, there was no calcification of the tumor on either radiologic or pathologic examinations.
MR imaging is the technique of choice in evaluating a synovial sarcoma because in comparison with other imaging techniques, it provides superior tissue characterization, can demonstrate involvement of neurovascular structures or bone marrow, can aid the preoperative planning, and can assist in grading the tumor and assessing clinical prognosis.
Most tumors display heterogeneous intermediate signal intensity on T1-weighted images. Small lesions are more likely to have predominantly homogeneous signal intensity similar to that of adjacent muscle; if the mass also has well-defined margins, a misdiagnosis of a benign lesion may be made. Morton et al (8) found that a synovial sarcoma was the type of malignant soft-tissue sarcoma most frequently misdiagnosed as benign. In both pre- and postcontrast images, the larger lesions are often heterogeneous, secondary to extensive areas of hemorrhage and necrosis.
On T2-weighted images, the tumors are usually hyperintense, with a signal intensity similar to, or lower than, that of fatty tissue. Considerable inhomogeneity, due to cystic, hemorrhagic, or necrotic change, is demonstrated in more than two thirds of lesions; fluid-fluid levels are demonstrated in the cystic components in 10%–25% of tumors (5). Approximately one third of lesions demonstrate a triple-signal-intensity pattern on T2-weighted images (5). The pattern is related to mixtures of hyperintense fluid with or without fluid levels, an intermediate signal intensity similar to that of fat, and a slightly hypointense signal intensity similar to that of fibrous tissue. Calcifications are not easily seen on MR imaging, and they are usually hypointense on images obtained with all sequences.
Tateishi et al (9) reported that statistically significant imaging findings supporting a diagnosis of a high-grade synovial sarcoma of the soft tissues include proximal distribution, large tumor size (>10 cm), the absence of calcification, the presence of a tumor cyst and hemorrhage, and the demonstration of a triple-signal-intensity pattern. They also observed that high-grade tumors are characterized by the demonstration of fluid-fluid levels in cysts, hemorrhage, and a triple-signal-intensity pattern.
In our patient, there was no evidence of a cyst with a fluid-fluid level, hemorrhage, or triple-signal-intensity pattern, and according to a previous report, these findings are consistent with a low-grade synovial sarcoma (9). Tumor calcification was not seen in our low-grade synovial sarcoma, and this finding is therefore at odds with a previous study that reported that the absence of calcification in a synovial sarcoma favors a diagnosis of a high-grade tumor and is associated with a poor prognosis.
The differential diagnosis of this case included a primary or metastatic tumor (extraskeletal Ewing sarcoma, lymphoma, or leukemic infiltration) and other benign neurogenic tumors (10, 11). Because the imaging findings in all paravertebral malignant tumors with epidural extension are similar, the final diagnosis depends on the histologic findings. However, benign tumors generally show a smooth tumor margin and lack of infiltrative growth. In the young adult, intervertebral disk herniation may be a further important factor in a differential diagnosis.
Complete surgical resection of the primary tumor is the mainstay of treatment. Adjuvant radiation therapy to treat microscopic residual disease after surgery provides excellent local control and obviates amputation for most patients with extremity tumors. The role of adjuvant chemotherapy remains controversial (12). Treatment of a paravertebral synovial sarcoma is similar but is complicated by the small operative field and the complex anatomy. The extension of the lesion to involve neurologic structures may preclude a complete resection and may limit the dose of radiation therapy, so chemotherapy should also be considered (4).
In conclusion, although rare, synovial sarcoma should be included in the differential diagnosis of epidural lesions with a paraspinal mass in patients with back pain and neurologic symptoms.
References
- Received December 3, 2004.
- Accepted after revision January 7, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Poorly Differentiated Synovial Sarcoma of the Lumbar Spine in a Fourteen-Year-Old Girl: A Case Report
- Poorly Differentiated Synovial Sarcoma of the Lumbar Spine in a Fourteen-Year-Old Girl: A Case Report
- A case of synovial sarcoma in the perivertebral space of the neck: clinical presentation, radiological findings and histopathological description