
Abstract
BACKGROUND AND PURPOSE: Imaging characteristics of temporal bone meningioma have not been previously reported in the literature. CT and MR imaging findings in 13 cases of temporal bone meningioma are reviewed to define specific imaging features.
METHODS: A retrospective review of our institutional case archive revealed 13 cases of histologically confirmed temporal bone meningioma. CT and MR imaging studies were reviewed to characterize mass location, vector of spread, bone changes, enhancement characteristics, and intracranial patterns of involvement. Clinical presenting signs and symptoms were correlated with imaging findings.
RESULTS: Thirteen temporal bone meningiomas were reviewed in 8 women and 5 men, aged 18–65 years. Meningiomas were stratified into 3 groups on the basis of location and tumor vector of spread. There were 6 tegmen tympani, 5 jugular foramen (JF), and 2 internal auditory canal (IAC) meningiomas. Tegmen tympani and JF meningiomas were characterized by spread to the middle ear cavity. IAC meningiomas, by contrast, spread to the cochlea and vestibule. Hearing loss was the most common clinical presenting feature in all cases of temporal bone meningioma (10/13). The presence of tumor adjacent to the ossicles strongly correlated with conductive hearing loss (7/9).
CONCLUSION: Meningioma involving the temporal bone is rare. Three subgroups of meningioma exist in this location: tegmen tympani, JF, and IAC meningioma. Tegmen tympani and JF meningiomas spread to the middle ear cavity. IAC meningiomas spread to intralabyrinthine structures. Conductive hearing loss is commonly seen in these patients and can be surgically correctable.
Meningioma of the temporal bone is a common tumor in a rare location; however, the imaging features and patterns of involvement have not been well characterized. Prognosis and treatment of temporal bone meningioma differs significantly from that of other more common entities in this location. Patients with temporal bone meningioma commonly have conductive hearing loss related to ossicular chain encasement by tumor, implying a component of surgically correctable hearing loss with appropriate management. Preoperative diagnosis, therefore, has important therapeutic implications.
Meningioma gains access to the temporal bone from 3 principal sites of origin: tegmen tympani and jugular foramen (JF) meningiomas, which spread secondarily into the middle ear cavity, and internal auditory canal (IAC) meningiomas, which invade the cochlea and vestibule. Distinctive CT and MR imaging features help to differentiate temporal bone meningioma from other more common tumors in this location. Analysis of bone changes on CT and enhancement pattern on MR imaging, combined with the characteristic vector of tumor spread in each location, will help alert the radiologist to this unusual diagnosis.
Materials and Methods
A retrospective case archive review, approved by our institutional review board, revealed 13 cases of histologically confirmed temporal bone meningioma in adult patients during a 10-year period from 1995 to 2005. Enhanced MR images and unenhanced temporal bone CT scans were reviewed to identify imaging characteristics of temporal bone meningioma.
CT examinations were reviewed to characterize mass location and patterns of bone involvement. The presence of hyperostosis and permeative, sclerotic, and/or destructive changes were noted in the skull base. Attenuation characteristics of the tumor and vector of spread either into the middle ear cavity and/or bony labyrinth were characterized in all cases. For middle ear cavity masses, ossicles were inspected for either erosive changes, defined as mild or incomplete bone loss, or destructive changes, considered to represent complete or near-complete absence of bone. The facial nerve canal was evaluated for areas of encroachment and dehiscence. MR images were reviewed for the following features: mass location, vector of spread, signal intensity, enhancement characteristics, and the pattern of intracranial involvement. Patient medical records were reviewed for demographic data and presenting features. Clinical symptoms and signs were then correlated with imaging findings when possible. The diagnosis of meningioma was confirmed by review of histopathologic records. The presence of ossicular erosion was recorded, if noted in the pathology report.
Results
A total of 13 cases of temporal bone meningioma in 8 women and 5 men, aged 18–65 years (mean, 52.7 years), were confirmed histopathologically. There were 6 tegmen tympani, 5 JF, and 2 IAC meningiomas.
Clinical Features of Temporal Bone Meningioma
Hearing loss was the most common clinical presenting feature in all cases of temporal bone meningioma, found in 10/13 cases (unknown, 3/13). Hearing loss was mixed in 5/13, conductive only in 2/13, sensorineural only in 3/13, and undocumented in 3/13. Nine patients had a soft-tissue mass either partly or completely surrounding the ossicles. The presence of tumor adjacent to the ossicles strongly correlated with a component of conductive hearing loss (7/9) on presentation.
Facial nerve symptoms were present in 2 patients, both of whom had CT evidence of facial canal encroachment by hyperostotic bone changes. Five additional patients had similar CT findings of facial canal narrowing without reported facial nerve symptoms.
Findings at otoscopy, available in 8/13 cases, were notable for the presence of a vascular-appearing retrotympanic mass in 7/13 cases, clinically mimicking paraganglioma. A gray mass was observed in the remaining case (1/8). A complete description of clinical features is listed in the Table.
Clinical and imaging features of temporal bone meningioma
All cases of meningioma were confirmed by histopathology. The intralabyrinthine component of enhancement in both IAC masses was also confirmed to represent meningioma on histopathology. A single tumor (tegmen tympani meningioma) had mild erosion of the stapes arch histologically, which was not apparent on imaging.
Radiologic Features of Temporal Bone Meningioma
Using imaging characteristics, we stratified meningiomas into 3 groups on the basis of primary location and tumor vector of spread. JF and tegmen tympani meningiomas were characterized by spread to the middle ear cavity. IAC meningiomas, by contrast, spread to the intralabyrinthine structures. One particularly large invasive middle ear cavity mass, primarily originating in the JF, also involved the tegmen tympani. MR imaging and CT characteristics are described in this article, according to location of origin.
Tegmen Tympani Meningioma
All cases of meningioma primary to the tegmen tympani arose from the floor of the middle cranial fossa and spread inferomedially into the middle ear cavity (Fig 1). Characteristic CT features included thickening of the tegmen tympani, observed in 5/6 cases (Fig 2A, -B). The internal trabecular architecture of the involved bone was preserved in all cases. This feature was termed “trabecular” hyperostosis, to contrast it to bone thickening observed in cortical hyperostosis or fibro-osseous lesions. The inner margin of the involved calvaria along the lateral aspect of the middle cranial fossa was irregular in 5/6 cases. A middle ear cavity soft-tissue mass, present in all cases, resulted in ossicular encasement or abutment in 5/6. No ossicular erosion or destruction was observed in any case. Calcification within the soft-tissue mass was seen in 2/6. Facial nerve canal encroachment was present in 4/6 cases (1 involving both the tegmen tympani and JF).

Coronal graphic depicts characteristic findings in tegmen tympani meningioma. Tumor arises in the middle cranial fossa and spreads inferomedially through the tegmen tympani to the middle ear cavity. En plaque intracranial enhancement is typical (straight white arrows). Ossicles are encased by tumor (curved white arrow), without destruction (reprinted with permission from Amirsys14).
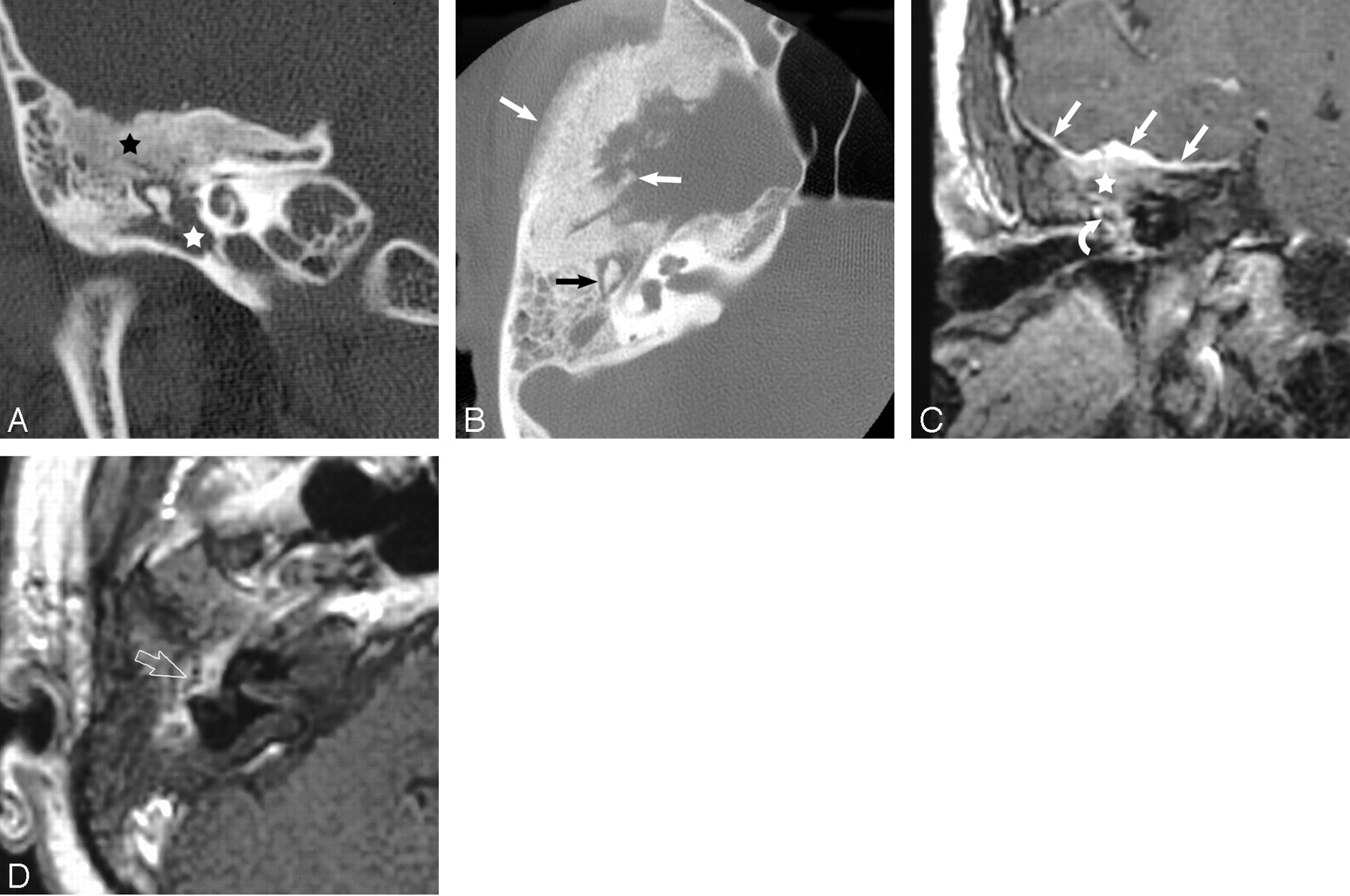
A, Coronal unenhanced CT scan reveals typical thickening and trabecular hyperostosis of the tegmen tympani (black star). Note the soft-tissue mass in the middle ear cavity (white star), which encases the ossicles but lacks erosive or destructive change.
B, Axial unenhanced CT scan shows ossicular encasement without erosive or destructive changes (black arrow). The involved calvaria (white arrows) is characterized by preserved internal architecture (trabecular hyperostosis) and irregularity of the inner table.
C, Coronal contrast-enhanced MR image shows typical en plaque enhancement along the floor of the middle cranial fossa (straight white arrows) in a tegmen tympani meningioma. Note thickened enhancing tegmen (white star) and enhancing tissue surrounding the ossicular chain (curved white arrow).
D, Axial contrast-enhanced MR image of the tegmen tympani meningioma shows tumor enhancement in the middle ear cavity. Note the intact appearance of the ossicular chain (open white arrow), seen through the enhancement.
MR imaging findings characteristic of tegmen tympani meningioma were en plaque linear dural enhancement along the floor of the middle cranial fossa and homogenous soft-tissue enhancement in all cases (Fig 2C, -D). The involved bone also enhanced, with preserved appearance of the internal architecture. A larger dural-based enhancing mass in the intracranial compartment was present in 3 cases. Vasogenic edema in the adjacent temporal lobe, without direct brain invasion, was observed in 1 case.
JF Meningioma
JF meningiomas were primarily centered in the JF, with superolateral vector of spread into the middle ear cavity (Fig 3). Characteristic CT features in JF meningioma included a centrifugal pattern of spread to the regional skull base in all cases. Involved bone showed a mixed permeative/sclerotic appearance in all cases. As with tegmen tympani meningiomas, the internal trabecular architecture was preserved in all cases. In contrast to tegmen tympani meningiomas however, bone thickening was not observed in any case. A soft-tissue mass involving the middle ear cavity was seen in all cases. Abutment or encasement of ossicles without destruction or erosion was observed in 4/5 (Fig 4A, -B).

Coronal graphic depicts findings in JF meningioma: location primary to the JF (white star) with superolateral vector of spread of the soft-tissue mass into the middle ear cavity (black arrow) (reprinted with permission from Amirsys14).

A, Coronal unenhanced CT scan shows a mixed permeative/sclerotic appearance of the involved skull base (white star) that is typical for JF meningioma. Bony changes mildly narrow the mastoid segment of the facial nerve canal (open white arrow).
B, Axial unenhanced CT scan again demonstrates the characteristic mixed permeative/sclerotic appearance and centrifugal involvement of the skull base (black star). Note intact-appearing cortical margins (black arrows). Although not a common finding, calcification of the soft-tissue mass (white arrow) is a fairly specific finding of meningioma when present.
C, Coronal enhanced MR image demonstrates an enhancing mass primarily located in the jugular foramen (white arrow), with centrifugal involvement of the surrounding skull base and superolateral soft-tissue spread to the middle ear cavity (black star). Note intense intraosseous enhancement relative to the extracranial component and largely preserved intrinsic bony architecture (black arrows).
D, Axial enhanced MR image demonstrates an intensely enhancing mass surrounding the intact-appearing ossicular chain (open white arrow). Note the intracranial enhancing dural tail (straight white arrow). Secondary extension to the internal auditory canal (curved white arrow) is also present in this case.
MR imaging features of JF meningioma included centrifugal skull base infiltration in all cases. The involved skull base invariably enhanced, with characteristic preservation of the internal architecture. The intratympanic soft-tissue mass and intraosseous component were observed to enhance more intensely than tumor below the skull base. (Fig 4C, -D). An associated intracranial enhancing dural “tail” was seen in all cases. Flow voids were not apparent in any case.
IAC Meningioma
Both IAC meningiomas involved the IAC and spread laterally to involve the cochlea and vestibular apparatus (Fig 5). One case was characterized by a large cerebellopontine angle enhancing mass with extension into the IAC and labyrinthine structures. The other demonstrated a tiny enhancing mass isolated to the IAC fundal apex, which extended laterally into the cochlea and vestibule. MR imaging of IAC meningioma revealed intense intralabyrinthine enhancement in both cases (Fig 6A, -B). An enhancing intracranial dural tail was present in the larger tumor. CT, available in 1 case, demonstrated a partly calcified intracochlear mass, with surrounding lucency of the involved otic capsule (Fig 7).

Coronal graphic depicts findings in IAC meningioma: tumor in the cochlea and vestibular apparatus (black arrows). Note the intracranial component in the IAC and cerebellopontine angle (black star) (reprinted with permission from Amirsys14).

A, Coronal enhanced MR image of an IAC meningioma demonstrates intense enhancement of the intralabyrinthine structures (curved white arrow). The mass extends from the IAC and cerebellopontine angle (open white arrow).
B, Axial enhanced MR image of an IAC meningioma demonstrates intense enhancement of the cochlea (curved white arrow) and vestibular apparatus (open white arrow). The large IAC and cerebellopontine angle enhancing mass (straight white arrow) are clues to the diagnosis.

Axial unenhanced CT scan demonstrates pericochlear bone lucency (straight black arrows). Calcification of the mass (curved white matter) suggests the diagnosis of meningioma, as seen in other locations.
Discussion
Temporal bone meningiomas are common tumors in an uncommon location. Although they have long been recognized from a clinicopathologic perspective, description in the imaging literature has been limited.1–4 Meningiomas typically gain access to the temporal bone via 3 potential sites of origin: the tegmen tympani, JF, and IAC. Arachnoid cap cells, the cells of origin in meningioma, are found in abundance in arachnoid granulations, JF, geniculate ganglion, and the pachymeninges.5–8
Temporal bone meningioma can be considered part of the ectopic meningioma group. Ectopic or extracranial meningiomas are classified into 4 subgroups: direct extension from primary intracranial meningioma, extracranial growth from cranial nerve sheath arachnoid cells, extracranial extension from embryonic arachnoid rests without connection to the skull base or cranial nerves, and distant metastasis from intracranial tumors.8
The likely mechanism in tegmen tympani meningioma is origin from the middle cranial fossa dura with inferomedial vector of spread through the tegmen tympani. Tumor likely spreads transosseously, though lack of frank bone destruction is an interesting feature that seems characteristic for meningioma. Bone infiltration in meningioma most commonly occurs by secondary spread, though primary intradiploic tumors are reported. Secondary infiltration of bone may reflect tumor involvement or reactive changes; however, these are not reliably differentiated on imaging. Irregular bone deposition occurs earliest along the inner table, though later outer table involvement, with spiculated margins, may occur.9 Origin from the dura along the distal cranial nerve sheaths may account for the occurrence of JF and IAC meningiomas.
Middle ear meningiomas (tegmen tympani and JF) commonly encase the ossicular chain, resulting in conductive hearing loss. Conductive loss is usually surgically correctable with appropriate management. Additional sensorineural hearing loss may also be present in these typically middle-aged patients; however, because there is no visible cause of sensorineural hearing loss on imaging, this might be unrelated to the tumor itself.
Patients treated with tumor resection and ossicular prosthesis implantation can expect serviceable hearing after surgery.10–13 Unlike paragangliomas, which more commonly affect the middle ear cavity, middle ear meningiomas appear to have no tumor invasion of the ossicles. Consequently, a more conservative surgical procedure, with the goal of ossicular preservation, can be considered, thereby allowing a substantially better hearing outcome for these patients.
Situations may arise in which indeterminate-sized (early or small) middle ear cavity masses are discovered. This scenario suggests that an approach of watchful waiting is most prudent. If no diagnostic imaging features are evident, follow-up imaging during a 6–12 month interval to ensure no aggressive growth pattern is recommended.
Middle Ear Meningioma: Tegmen Tympani
Middle ear meningioma can be confused with other lesions, depending on their site of origin. Tegmen tympani meningioma bone changes on CT can be confused with fibrous dysplasia of this area. Preservation of internal trabecular architecture distinguishes it from the ground-glass attenuation seen in typical fibrous dysplasia however. Enhanced T1-weighted MR images clearly show the characteristic thickened enhancing dura along the intracranial surface of the tegmen tympani, which would mitigate against fibrous dysplasia. The other dominant consideration for tegmen tympani meningioma on CT is cholesteatoma; however, on CT, meningiomas lack the bone and ossicular destructive changes. Enhanced MR imaging will distinguish meningioma from cholesteatoma because the latter will not enhance.
Other diagnostic considerations for tegmen tympani meningioma include granulation tissue, facial nerve hemangioma, and facial schwannoma. These all lack the characteristic tegmen tympani thickening on CT and dural enhancement along the floor of the middle cranial fossa seen with meningioma on enhanced MR imaging. Enlargement of the facial canal typical of schwannoma is not seen with meningioma. Facial nerve hemangioma causes amorphous honeycomb bone changes on CT in larger lesions, which differ from the trabecular hyperostosis of tegmen tympani meningioma. Ossifying variants of hemangioma may have spicules of lamellar bone, which could more easily mimic meningioma on CT; however, most facial nerve hemangiomas are primarily centered in the geniculate fossa. This location should help distinguish them from meningioma.14
Vasogenic edema in the temporal lobe, observed in 1 tegmen tympani meningioma, presumably reflected reactive edema. This finding is seen with up to 50% of intracranial meningiomas, and although it can suggest a more difficult resection for surgeons, it does not imply brain invasion or malignancy.8,15 Resolved edema on follow-up imaging in this patient after resection of the enhancing component confirmed this impression.
Middle Ear Meningioma: JF
JF meningioma that accesses the middle ear mimics glomus jugulare paraganglioma. However, the permeative sclerotic bone changes on CT and the absence of flow voids on MR imaging, seen in JF meningioma, are distinctly different from the permeative destructive changes on CT and flow voids on MR imaging of glomus jugulare paraganglioma.
IAC Meningioma
IAC meningioma that involves the inner ear may initially suggest the diagnosis of schwannoma on MR imaging. MR imaging findings of a dural tail favor the diagnosis of meningioma over acoustic schwannoma. Uniform enhancement of all intralabyrinthine structures supports the diagnosis of meningioma, because uniform enhancement of both the cochlea and vestibular apparatus is atypical for schwannoma.
Reactive intralabyrinthine enhancement should also be considered in cases in which the IAC is obstructed by tumor. Such IAC “block” is thought to cause venous congestion and/or inflammation, though the enhancement seen with tumors is typically much more intense than that seen as a result of vascular engorgement or inflammation. Relative T2 hypointensity is a helpful imaging finding, suggesting cellularity, and supports a diagnosis of tumor rather than reactive enhancement. Because hearing loss is not usually correctable following surgical resection of intralabyrinthine tumor however, treatment should be based on clinical indications with this fact in mind.
Conclusion
Temporal bone meningioma can be separated into 3 subgroups on the basis of site of origin, vector of spread, and specific CT/MR imaging findings. Common to all temporal bone meningiomas is the presence of an intracranial enhancing dural-based component and preserved internal architecture of involved bone. Tegmen tympani and JF meningiomas are characterized by an enhancing soft-tissue mass in the middle ear cavity without erosive or destructive changes of involved bone or ossicles. JF meningiomas have a permeative/sclerotic appearance of the involved skull base. By contrast, IAC meningiomas are characterized by intralabyrinthine tumor spread, with intense enhancement of the cochlea and vestibule.
References
- Received December 6, 2005.
- Accepted after revision February 4, 2006.
- Copyright © American Society of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}