
Abstract
SUMMARY: The characteristics of multiple sclerosis (MS) lesions on diffusion-weighted sequences and apparent diffusion coefficient (ADC) mapping at the very early phase of symptoms have not been clearly described. We report the case of a young woman who presented with a sudden pseudostroke form of MS resulting in hemiplegia and sudden aphasia. MR imaging showed a lesion of the left internal capsule with reduced ADC, which suggests an ischemic stroke. This case shows that very acute MS lesions may have reduced ADC on MR imaging, reflecting cytotoxic and not vasogenic edema.
Acute, pseudostroke manifestations of multiple sclerosis (MS) are rare: only a few cases of sudden aphasia, sudden deafness, or hemiplegia have been described.1–3 These manifestations can be confused with the acute phase of stroke, and diffusion-weighted MR imaging (DWI) should facilitate the differential diagnosis. The current data in the literature concerning DWI of acute lesions of MS, however, are contradictory. Some authors consider that recent lesions present high-intensity signals on b-1000 sequences and an unreduced apparent diffusion coefficient (ADC) for less than 3 months.4,5 It has been shown that higher ADCs in acute lesions than in chronic lesions were the result of demyelination or vasogenic extracellular edema.6–12 The behavior of very newly diagnosed MS on DWI sequences has been poorly described during the first 24 hours, and especially only 2 hours after the onset of the symptoms.13
We report a case of a sudden-onset MS with right hemiparesis and aphasia. MR imaging, performed within the second hour after the onset of symptoms, showed a left capsular lesion appearing as an acute ischemic lesion with high signal intensity on DWI and a reduced ADC.
Case Report
A 36-year-old right-handed Portuguese woman, taking no treatment, was admitted for a sudden onset of right hemiplegia and aphasia. Her history included 3 episodes of spontaneously resolving (4–5 days) right hemibody motor deficit during a 13-year period (1989, 1994, and 1998). A brain CT scan performed in 1994 was normal. She remained asymptomatic after these episodes without treatment. Brain MR imaging performed in 1997 showed 4 high-intensity lesions of the white matter on T2-weighted sequences, including one right periventricular lesion without high signal intensity of the left internal capsule (Fig 1).

Brain MR imaging, T2-weighted sequence: high-intensity white matter images, 2 of which are periventricular.
In November 2002, she suddenly developed right hemiplegia of the face, arm, and leg and aphasia for which she was referred for thrombolysis with a suspected diagnosis of stroke. MR imaging performed 2 hours after onset of the deficit showed a lesion of the left internal capsule (Fig 2). This lesion had high signal intensity on fluid-attenuated inversion recovery (FLAIR) images, high signal intensity on DWI, and a reduced ADC: 45.2 × 10−5 mm2/s for the region of interest versus 73 × 10−5 mm2/s for apparently normal white matter. Six other, older high-intensity images on T2-weighted sequences were observed in the white matter of both hemispheres that did not alter diffusion.
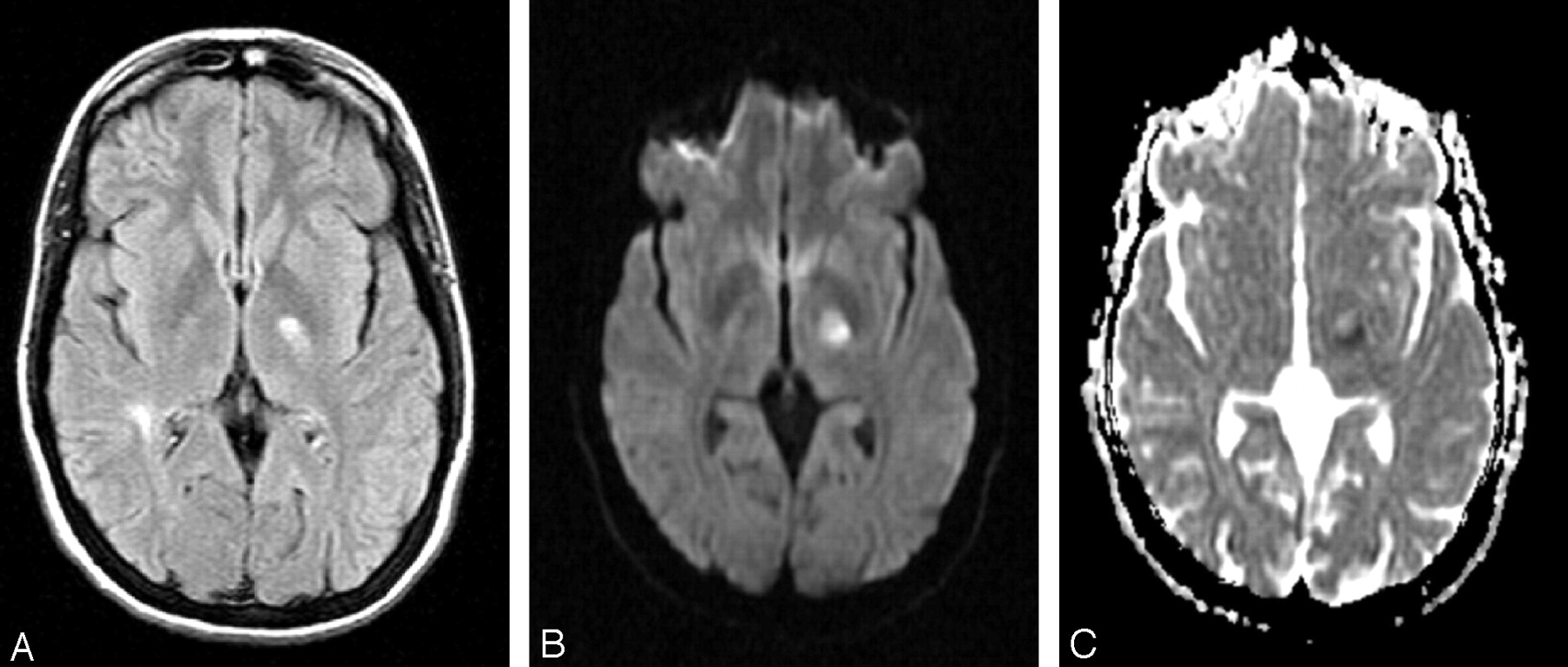
Brain MR imaging 2 hours after onset of symptoms.
A, FLAIR sequence, showing high signal intensity of left internal capsule.
B, DWI, showing high signal intensity of left internal capsule.
C, ADC mapping, showing reduced ADC of the left internal capsule lesion.
In view of the initial recovery of the deficit, the disseminated white matter abnormalities on MR imaging, and the early high signal intensity on FLAIR images, the patient was not treated by thrombolysis, but anticoagulation with heparin was instituted. On the fifth day, the patient suddenly deteriorated with flaccid paralysis of the right face, arm, and leg. MR imaging performed on day 10 after onset of the symptoms showed extension of the left internal capsule lesion presenting a high signal intensity on FLAIR, DWI with b = 1000, and a heterogeneous ADC (one part with reduced ADC and another part with high signal intensity) (Fig 3).

Brain MR imaging on day 10.
A, FLAIR sequence, showing extension of the left internal capsule lesion.
B, DWI, showing extension of the left internal capsule lesion.
C, ADC mapping, showing heterogeneous ADC of the left internal capsule lesion.
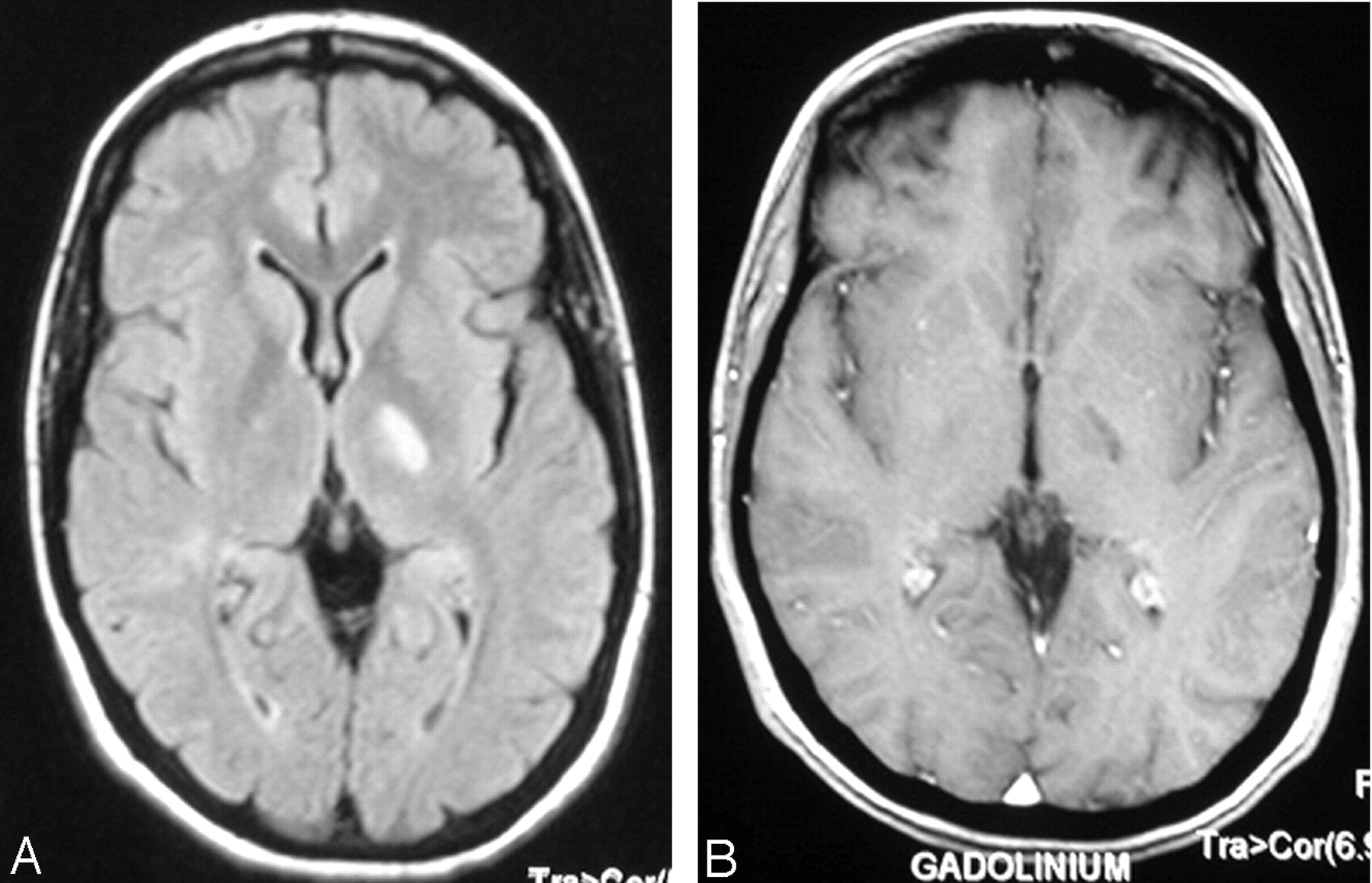
Neurovascular assessment showed no abnormality: electrocardiography, transesophageal and transthoracic echocardiography, and MR angiography of neck vessels and circle of Willis were normal. Cerebral arteriography was normal. A complete immunologic and infectious assessment did not reveal any abnormality. Lumbar puncture revealed a clear fluid liquid with normal cellularity and CSF protein. CSF electrophoresis demonstrated 3 oligoclonal bands with a high IgG index. Evoked potentials showed bilateral altered visual- evoked potentials (VEPs) and altered motor-evoked potentials (MEPs) on the right. An intravenous bolus of methylprednisolone (1 g/day for 5 days) followed by oral treatment for 1 month with tapering of the dose improved the deficit by the first week. The clinical course was favorable with recovery of gait by 1 month, but persistence of a deficit of the right hand and aphasic elements and clumsiness of the right hand at the third month. At 1-year follow-up, the patient presented only fatigability of the right leg on effort. MR imaging revealed regression of the left internal capsule lesion on FLAIR images at 6 weeks with a high signal intensity on DWI (b = 1000 and ADC) and no contrast enhancement at the second month (Fig 4). Wallerian degeneration of the left pyramidal tract was observed at 1 year. Subcutaneous beta interferon therapy was instituted. No new episodes were observed at 20 months of follow-up.

Brain MR imaging at 3 months.
A, FLAIR sequence, showing regression of the high signal intensity of the left internal capsule.
B, Gadolinium-enhanced T1-weighted image, showing no contrast enhancement of the lesion.
Discussion
Sudden-onset pseudostroke forms of MS are rare, and the behavior of these very recent plaques on DWI has not been well described. In the present case, the sudden onset of the deficit, the arterial topography of the symptoms and DWI (high b-1000 signal intensity and reduced ADC) initially suggested a diagnosis of stroke rather than an acute episode of MS. However, because of the temporal dissemination (4 episodes during a 13-year period), the spatial dissemination (VEP abnormalities and motor lesion of the right hemibody with altered MEPs), suggestive MR imaging, a high CSF IgG index, and the absence of data suggestive of cerebral vasculitis, the diagnosis of MS was proposed according to McDonald’s criteria.14
Data in the literature on DWI of MS are contradictory. To the best of our knowledge, the appearance of very acute lesions (within the first few hours after onset of the neurologic signs) has not been described. The high ADC in MS lesions reflects the increase of the extracellular space either by extracellular edema or by demyelination.11 Otherwise, an elevation of perfusion has been detected as an early event in the development of a plaque, before increases in the ADC and before permeability of the blood-brain barrier.15
Gass et al proposed the hypothesis that ADC may be reduced in acute MS lesions due to the release of inflammatory cytokines, which would induce mitochondrial dysfunction responsible for cytotoxic edema.13 This MR image also raises the problem of the etiopathogenesis of this plaque. In a study based on biopsies and autopsies of patients with MS, several histopathologic patterns were described corresponding to various forms of MS. Pattern III is associated with acute pseudostroke forms of MS and is characterized histologically by oligodendrocytes dystrophy and apoptosis similar to myelin destruction in acute white matter ischemia.16 Lassmann et al have recently described a new CSF epitope of hypoxia-like tissue damage in active MS lesion, which is found also in white matter ischemia.17 An extensive apoptotic oligodendrocytes death could be the initial event in new lesion formation.18 Vascular injury has long been considered in the pathogenesis of MS.19–20
The originality of our case concerns the difficult differential diagnosis between stroke and acute pseudostroke form of MS and the appearance of this lesion on DWIs, emphasizing the neuroradiologic diversity of MS lesions.
Conclusion
This case report raises the problem of the differential diagnosis of the sudden onset of a neurologic deficit in a young subject, between stroke and MS. In particular, the case presented here shows that some very recent lesions can behave like ischemic lesions on DWI, with a high signal intensity on DWI and a reduced ADC.
References
- Received December 21, 2004.
- Accepted after revision July 7, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Fulminant tumefactive multiple sclerosis in pregnancy
- Restricted diffusion preceding gadolinium enhancement in large or tumefactive demyelinating lesions
- Reduced Diffusion in a Subset of Acute MS Lesions: A Serial Multiparametric MRI Study
- Diffusion-weighted imaging characteristics of biopsy-proven demyelinating brain lesions
- A weak leg
- Multiple Sclerosis and Chronic Cerebrospinal Venous Insufficiency: The Neuroimaging Perspective
- Teaching NeuroImages: Marked reduced apparent diffusion coefficient in acute multiple sclerosis lesion
- Dot-to-dot