
Abstract
SUMMARY: A 66-year-old man with multiple myeloma treated with zoledronic acid, melphalan, and prednisone after a tooth extraction developed severe osteonecrosis of the mandible that was nonresponsive to antibiotic therapy. A CT scan showed innumerable fragmented sequestra in the mandible and some adjacent soft tissue fullness around the mandible. The association between the use of bisphosphonates and osteonecrosis of the jaw has been described only recently.
Multiple myeloma (MM) is a disseminated plasma cell neoplasm characterized clinically by osteolytic bone lesions, monoclonal immunoglobulin detectable in the serum and/or urine (in more than 90% of patients), renal insufficiency, and amyloidosis (in 10% of patients). MM is the third-most-common hematologic malignancy, accounting for nearly 10% of all such neoplasia.1,2 It is often inaccurately viewed as a rare disease because of its short survival (median survival, 2.5–3 years) and its uniformly fatal outcome. Bone involvement is the hallmark of MM, and these findings are manifest in most patients at the time of diagnosis as lytic lesions, osteoporosis, and/or fractures.3
Improved understanding of myeloma-associated bone disease has led to the use of prophylactic bisphosphonate therapy. Apart from delaying the onset of skeletal events, the new generation of bisphosphonates—in particular pamidronate and zoledronic acid—exerts antimyeloma effects indirectly by inducing osteoclast apoptosis or directly by inducing myeloma cell apoptosis.4 Recent reports have shown an increasing association between the use of bisphosphonates and osteonecrosis of the jaw (ONJ).5–8 We report the case of a patient with MM who received chronic bisphosphonate therapy and developed osteomyelitis of the mandible a few days after a tooth extraction. The mandibular disease is documented with CT for the first time in the radiologic literature. The clinical literature contains 2 previous CT images, both cases being far less extensively involved than our case.7,8
Case Report
A 66-year-old man was diagnosed with MM in 2002. Shortly after his diagnosis, treatment with zoledronic acid, melphalan, and prednisone was initiated. After approximately 2–3 months, he developed a loose mandibular molar, which was removed. The extraction socket never healed, and the patient underwent biopsy of the exposed bone, which was consistent with osteomyelitis. He was placed on multiple courses of antibiotics without resolution of the exposed bone. During that interval, the teeth adjacent to the nonhealing socket also became loose and were subsequently removed sequentially.
In October 2003, the patient complained of jaw pain and numbness of his lower lip and chin. On physical examination, the patient had large areas of exposed and seemingly nonvital bone in the mandible bilaterally. This was especially prominent along the mylohyoid ridge areas. There was purulent exudate within the open wounds and a fetid odor. There were multiple mobile teeth within the mandible. The patient had anesthesia along the dermatome distribution of the right inferior alveolar nerve. There were no lesions present within the maxilla, and all of the maxillary teeth were stable. Panoramic radiographs showed areas of patchy radiolucency within the mandible, widened periodontal ligament spaces around the mandibular dentition, and periosteal bone deposition along the inferior border of the mandible. Aggressive local wound care was initiated, and the patient had a satisfactory response with near resolution of the infection and decrease in pain. Reparative granulation tissue in intervening sites along the open wounds was noted during a 2-month period.
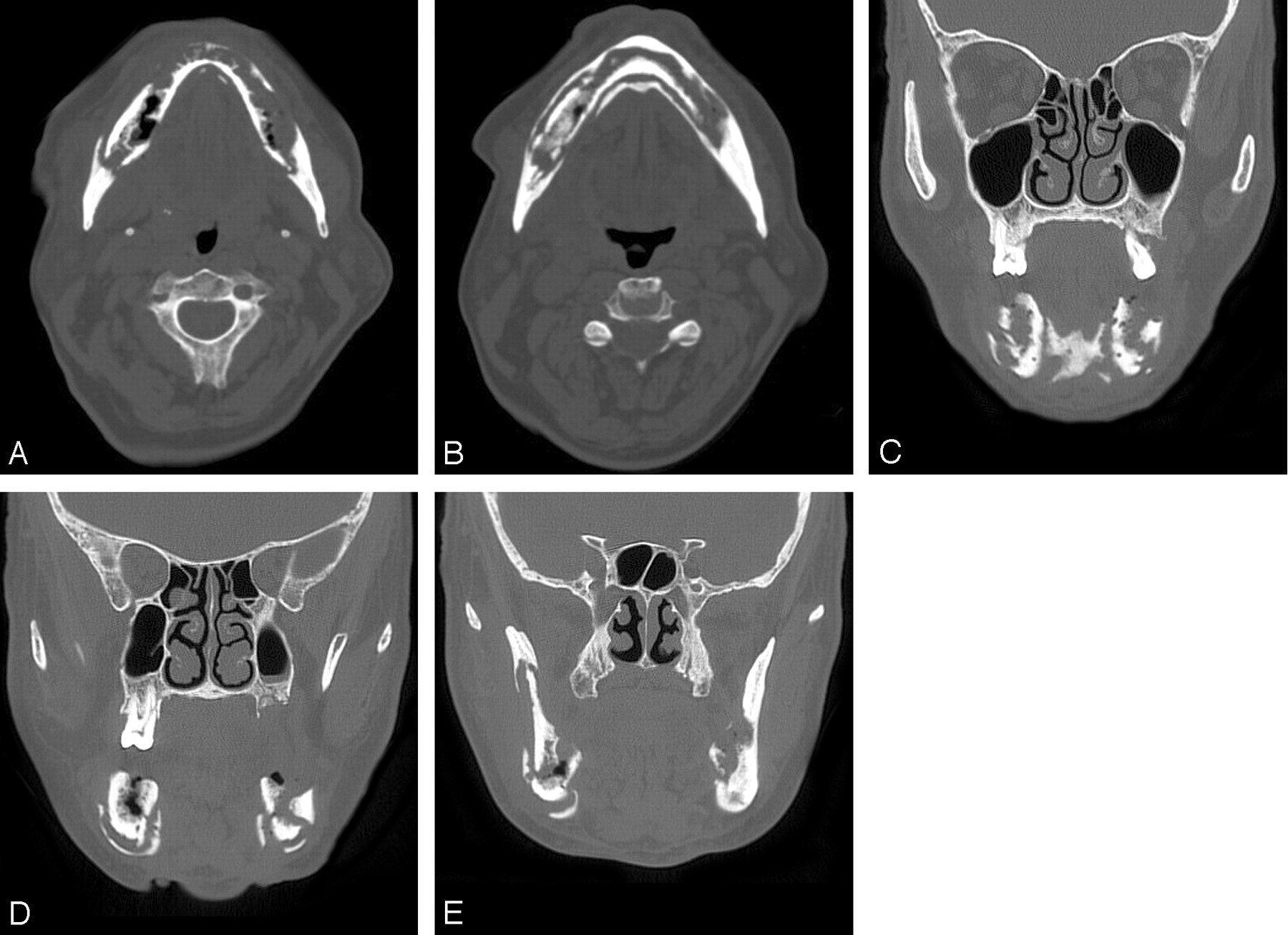
The patient was then lost to follow-up until February 2005, when he returned to the office complaining of severe pain. He had stopped treatment. On intraoral examination, the patient had copious purulence from large areas of exposed, necrotic bone along most of the mandibular alveolar ridge. Thin intervening bands of normal-appearing mucosa were present within the anterior mandible. He was noted to have 2 draining fistulas in the submental area with active purulent exudate. Palpation of the exposed bone in the right posterior mandible resulted in mobility of the exposed bone in the anterior and left mandible. A panoramic radiograph showed large areas of bone destruction throughout the mandible with proliferative bone deposition along the inferior border. A CT scan showed (Fig. 1) innumerable fragmented sequestra in the mandible, starting at the level of the coronoid process on the right and the midramus on the left, extending through the angle and body bilaterally and including the symphysis. There was some soft tissue fullness adjacent to the posterior body of the mandible on the right side and some cellulitic/edematous type changes in the soft tissues around the mandible.

Serial axial (A and B) and coronal (C–E) CT scans of the mandible show extensive fragmentation and sequestration of this edendulous mandible. There was mild adjacent soft tissue fullness. This degree of osteonecrosis would be excessive for the more common radiation-related disease.
Discussion
ONJ has multiple etiologies and is most commonly seen following radiation therapy for the head and neck malignancies.6 Rare cases have been described in association with herpes zoster and in a patient with osteopetrosis.9 The jaw findings in MM are present in 5%–39% of cases and are the first manifestation of the disease in 17% of patients. Patients typically present with painless mandibular swelling. The radiologic features are variable, but most commonly noted are solitary or multiple punched-out lytic lesions, occasionally with septation.10
Bisphosphonates are nonmetabolizated analogues of pyrophosphate that play an important role in bone reabsorption. They inhibit osteoclastic action, have an antiangiogenesis effect, and are helpful in the maintenance of the calcium and phosphate equilibrium. Although the exact mechanism of this bisphosphonate-mediated osteoclast inhibition has not been completely elucidated, their role in decreasing osteoclast-mediated lysis of bone has been well established in clinical trials in patients with MM, breast cancer, Paget disease of bone, and postmenopausal osteoporosis.8 These drugs are effective in reducing bone pain, hypercalcemia, and skeletal-related events in patients with osteolytic metastasis. In fact, according to the American Society of Clinical Oncology Practice Guidelines, the use of intravenous pamidronate and zoledronic acid is recommended for patients with pain due to osteolytic bone disease and as adjunctive treatment for patients receiving radiation therapy, analgesics, or surgical intervention to stabilize fractures or impending fractures.11
ONJ associated with bisphosphonates most commonly occurs in the mandible but can also occur in the maxilla. Most patients present with jaw pain and exposed necrotic bone, which usually starts at the site of a recently extracted tooth (70%–77%), similar to our patient.6,8 The more or less unique involvement of the jaw bones by osteonecrosis has been attributed to their direct exposure to the external environment via the teeth, which in turn are frequently associated with periodontal disease and trauma. The clinical presentation may simulate a dental abscess and osteomyelitis and radiographs usually show regions of mottled bone, consistent with sequestrum formation.6
The differential diagnosis of ONJ should include neuralgia-inducing cavitatory osteonecrosis (NICO). Unlike patients with ONJ associated with bisphosphonate use, patients with NICO present with atypical facial pain or trigeminal neuralgia, which often has been present for years. Tooth loosening and tooth loss because of dissolution of the alveolar medullary bone are also common findings in NICO. The radiographic changes associated with NICO are variable but primarily show a poorly demarcated, nonexpansile radiolucency of the affected alveolus, often with irregular vertical remnants of lamina dura associated with old dental extraction sites.12
Bisphosphonate-associated ONJ has only recently been described in the clinical literature. To the best of our knowledge, imaging features were mentioned in only 2 of these reports, and they were in patients with far more subtle disease than seen in our patient.7,8 Although the exact mechanism of bisphosphonate-associated ONJ is not fully understood, there many patients with MM, metastatic cancers, and osteoporosis who are receiving chronic bisphosphonate therapy. Because imaging studies will be conducted for many of these patients, the radiologist should be aware of this unusual entity.
References
- Copyright © American Society of Neuroradiology





{kind=link}