
Abstract
SUMMARY: Nasopharyngeal extension of the glomus tympanicum is rare. Only 2 cases have been reported in the literature to date. We present a reported case of a large nasopharyngeal extension of recurrent glomus tympanicum, with various kinds of imaging and histopathology and a review of the literature.
Glomus tympanicum is a paraganglioma that arises in glomus bodies situated in the cochlear promontory. It is the most common primary neoplasm of the middle ear.1 Glomus tympanicum, in its characteristic location just lateral to the cochlear promontory, may grow larger, abut the inner margin of the tympanic membrane, and present with conductive hearing loss and a vascular retrotympanic mass. Larger tumors may grow into the mastoid or extend through the tympanic membrane to fill the external auditory canal.2 Rare extensions into the eustachian tube and nasopharynx with a clinical presentation of epistaxis have been described.3,4
Case Report
A 61-year-old woman presented with a history of recurrent epistaxis from her left nostril for the past 3 months. Findings of a physical examination revealed a large left nasopharyngeal mass. Two separate biopsies at other hospitals had been performed, and both histopathologic diagnoses were for chronic inflammation. She was subsequently referred to an otorhinolaryngologic surgeon at our hospital. A nasal endoscopic examination revealed a firm reddish hypervascular mass bulging into the nasopharynx and extending from the eustachian tube. Her clinical history for operations of glomus tumor within her left ear in the past 10 years was obtained.
CT revealed an intense enhancing mass, approximately 28 × 18 × 14 mm, at the left nasopharynx, continuing into the smaller portion within the slightly expanded eustachian tube and the middle ear. The degree of enhancement was as pronounced as the nearby vessels and resulted in a radiologist’s report suggesting a differential diagnosis of carotid artery aneurysm (Fig 1). MR imaging confirmed the solid hypervascular nasopharyngeal mass protruding from the smaller mass within the slightly expanded eustachian tube and middle ear (Figs 2 and 3). Recurrent glomus tympanicum with a eustachian tube and nasopharyngeal extension was diagnosed. Angiography also confirmed the diagnosis with the demonstration of an intense parenchymal blush in the left tympanic region extending anteriorly into the eustachian tube and nasopharynx. Feeding arteries from branches of the ascending pharyngeal artery, internal maxillary artery, middle meningeal artery, and posterior auricular artery were noted (Fig 4).

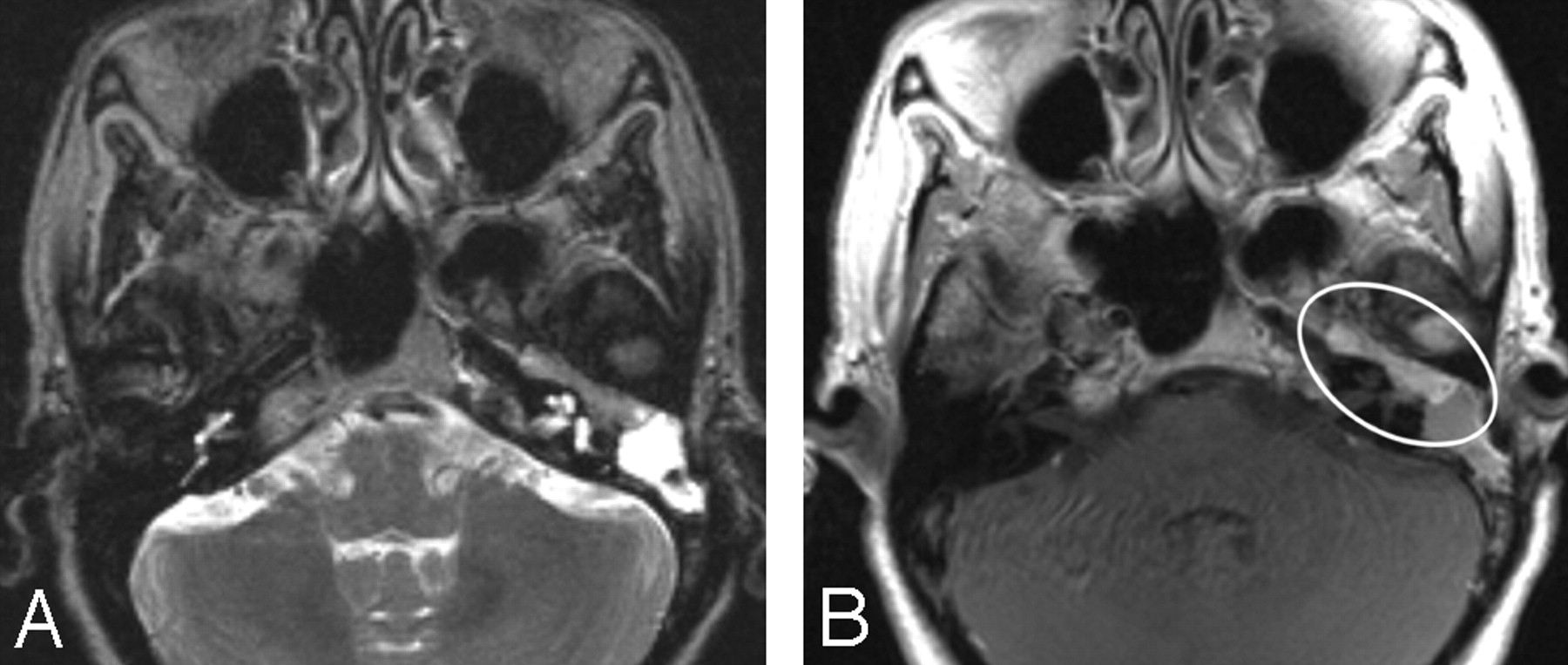
Contiguous 3-mm contrast-enhanced axial CT scans were obtained.
A, At the level of the nasopharynx, an intense homogeneous enhancing mass was seen within the left nasopharynx.
B, At 2 upper consecutive levels, continuation with the smaller part within the left eustachian tube and middle ear cavity was noted (circle).

MR images obtained at the level of nasopharynx. An isosignal intensity mass within the left nasopharynx on the spin-echo T2-weighted image (TR/TE, 6821/112) suggests a firm solid-appearing mass protruding from the smaller mass within the slightly expanded eustachian tube (A). Strong enhancement with multiple tiny vascular flow voids indicates hypervascularity on a post-gadolinium-diethylene-triaminepentaacetic acid (Gd-DTPA) spin-echo T1-weighted image (TR/TE, 874/15) (B).

MR images obtained at the level of temporal bone. A, Spin-echo T2-weighted image (TR/TE, 6821/112). B, Post-Gd-DTPA spin-echo T1-weighted image (TR/TE, 874/15). Continuation with the smaller mass within the slightly expanded eustachian tube and the middle ear is demonstrated.

Digital subtraction angiography of the left external carotid artery, lateral view. Hypervascular tumor blush extends further anteriorly than is usual along the course of the eustachian tube and nasopharynx (arrowhead), mainly fed by branches from the enlarged left ascending pharyngeal artery (long arrow). Also note feeding arteries from the internal maxillary artery, middle meningeal artery, and posterior auricular artery.
Definite histopathologic diagnosis is a mandatory requirement before initiating radiation therapy at our institution. Despite high confidence in the diagnosis, the surgeon decided to perform a careful tissue biopsy. Because of the patient’s history of inconclusive histopathologic tissue from 2 previous nasopharyngeal biopsies, a biopsy of the mass observed within the middle ear was performed instead. The histopathologic analysis revealed cholesterol granuloma. Another attempt was performed at the left nasopharyngeal mass. A minor active hemorrhage was well controlled with adrenalin packing. Histopathology revealed a highly vascularized tumor located in the submucosal region with the formation of tumor cell nests called “Zellballen,” which were separated by the thin rims of a highly vascularized fibrous stroma. The tumor cells possessed a granular basophilic cytoplasm and uniformly round-to-ovoid nuclei. The reticulin stain highlighted the delicate stroma around the tumor nests. The immunohistochemical study showed immunoreactivity for chromogranin in the cytoplasm of the tumor cells compatible with paraganglioma (Fig 5). The patient was sent for radiation therapy after a definite histopathologic diagnosis.

A, Histopathology reveals a highly vascularized tumor located in the submucosal region (hematoxylin-eosin, original magnification ×100).
B, At a higher magnification, formation of multiple tumor nests called “Zellballen,” which are separated by the thin rims of highly vascularized fibrous stroma, is seen. The tumor cells possess granular basophilic cytoplasm and uniform round-to-ovoid nuclei (original magnification ×200).
C, The reticulin stain highlights the delicate stroma around the tumor nests (original magnification ×400).
D, Immunohistochemical study shows the immunoreactivity for chromogranin in the cytoplasm of the tumor cells (original magnification ×400).
Discussion
Despite a very rare manifestation and unusual appearance, the imaging diagnosis of the nasopharyngeal extension of the glomus tympanicum should be achievable with a high confidence level. The very intense enhancing solid mass within the nasopharynx, continuing with the mass in the middle ear via the expanded eustachian tube, especially in a patient with a history of glomus tympanicum, should suggest the correct diagnosis. No other comparable differential diagnoses for such findings exist.
Although squamous cell carcinoma of the nasopharynx can easily invade the opening of the eustachian tube, located immediately anterior and inferior to the fossa of Rosenmuller, and can result in serous otitis media, it is usually difficult to identify the continuity of the tumor from the nasopharynx to the middle ear cleft because of its small size.5 Furthermore, its enhancement is much less intense than a glomus tumor and should, therefore, be easily distinguishable. Lymphoma and salivary gland tumors are other common tumors of the nasopharynx but have never been reported to involve the eustachian tube. Primary tumors involving the eustachian tube are exceedingly rare, with only 2 cases of glomus tympanicum reported3,4 and 1 case of a dermoid (William P. Dillon, personal communication; Aug 10, 2005). The first reported case was of a 61-year-old woman with recurrent glomus tympanicum and a clinical history of surgery 7 years earlier.3 Another case was of a 50-year-old woman with a suspected history of glomus tympanicum, but with inconclusive biopsy tissue and a last follow-up 16 years ago.4 As was the case with our patient, both patients presented with recurrent epistaxis and a presumed diagnosis of recurrent paragangliomas. Theoretically, vascular lesions such as Kaposi’s sarcoma or hemangioma may involve the eustachian tube, though neither case is evident in the world literature. Expansion of the eustachian tube is a typical finding. Contrary to erosion of the glomus jugulare, which almost always represents jugular bulb erosion, bone erosion is not usually present, even in the larger case of glomus tympanicum.6
Although a CT scan can clarify the extension of the tumor, its degree of intense enhancement can be misleading and can result in a diagnosis of unusual aneurysm. The location of the mass continuing from the middle ear mass via the expanded eustachian tube should suggest the correct diagnosis.
MR imaging is the technique of choice, not only to clarify the extension of a tumor but also to confirm its solid hypervascular nature. In paraganglioma larger than 2 cm, an apparently unique salt-and-pepper pattern of hyperintensity and hypointensity on T1-weighted and T2-weighted images has been described.2 Also identified are serpentine and arborizing flow voids of hypertrophic medium-sized and larger tumor vessels. The isosignal intensity of the mass on spin-echo T2-weighted images suggests a firm solid-appearing mass, and the nearby multiple small flow voids with intense enhancement indicate hypervascularity. MR imaging may make possible a presumptive diagnosis of glomus tympanicum tumor, extending down the eustachian tube and the nasopharynx, with high confidence. In both previously reported cases, subsequent radiation therapy was performed despite a lack of a definite histopathologic diagnosis.3,4
On angiography, this neoplasm is characteristically hypervascular, with enlarged feeding arteries and rapidly draining veins. The most common feeders are branches of the ascending pharyngeal artery. Other common feeders are the posterior auricular, stylomastoid, and occipital arteries. Larger tumors derive their blood supply anteriorly from the internal maxillary artery and superiorly from the internal carotid artery. Because angiographic vascularity is sufficiently characteristic, some authors believe it to be diagnostic and consider a biopsy unnecessary.2,7
Despite its slow-growing nature and rare tendency to metastasize, paraganglioma can be lethal if left untreated.2,8 Current treatments mainly include resection as a cure or radiation for long-term control.
The histopathologic finding of cholesterol granuloma from the mass biopsied from the middle ear was not surprising. Cholesterol granuloma, brownish fluid containing cholesterol crystals, can be an isolated phenomenon or act in conjunction with other middle ear maladies such as chronic otitis media. Eustachian tube dysfunction with secondary mucosal edema and blood vessel rupture is considered the most likely etiology. Stagnation of hemorrhagic contents occurs because of a lack of drainage, and red blood cell breakdown leads to further formation of cholesterol crystals. Cholesterol granuloma limited to the middle ear may masquerade otoscopically as a vascular mass, which may lead the clinician to initially suspect paraganglioma, an aberrant internal carotid artery, or a dehiscent internal jugular vein. The history is usually a tip-off in this regard.6
This reported case, along with others, confirms the very specific imaging diagnosis of glomus tympanicum seen as an intense enhancing solid mass within the nasopharynx and continuing with the mass in the eustachian tube and middle ear, which can obviate a high-risk tissue biopsy.
- Received June 16, 2005.
- Accepted after revision October 5, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.