
Abstract
BACKGROUND AND PURPOSE: Ulceration is a severe complication of carotid plaque. The purpose of this study was to evaluate the role and the diagnostic efficacy of multidetector row CT angiography (MDCTA) and ultrasound (US) echo color Doppler (US-ECD) in the study of patients with carotid plaque complicated by ulceration through the comparison with the surgical observation.
MATERIALS AND METHODS: From January 2004 to October 2005, 237 patients, for a total of 474 carotid arteries, studied at first with color Doppler US, were analyzed using CT angiography. A total of 103 patients underwent a carotid endarterectomy. We analyzed stenosis degree, plaque composition, and presence of ulcerations. In a second phase, the data were compared with the surgical results when the MDCTA indicated surgical intervention.
RESULTS: MDCTA found 31 ulcerations; the surgical confirmation underlined a 93.75% sensitivity and a 98.59% specificity. US-ECD performances were 37.5% and 91.5% for sensitivity and specificity, respectively. The number of patients who showed plaque ulcerations increased with the severity of stenosis. Furthermore, ulcerations of the carotid plaque occurred more often proximal than distal to the point of maximum stenosis, and this trend increased with the severity of the stenosis. We also determined that fatty plaques were more likely to be affected by ulcerations.
CONCLUSIONS: The results of our study suggest that MDCTA detects with higher sensitivity and specificity the presence of ulcerated plaque compared with US-ECD, which has been demonstrated to be less effective in this evaluation. Considering the high MDCTA sensitivity and specificity for detection of plaque ulceration, we therefore recommend MDCTA as a useful step for correct presurgical planning.
Stroke is the third leading cause of severe disability in the Western world,1 and it represents the second leading cause of death in the world,2,3 producing an enormous health and economic problem for society. Extracranial carotid atherosclerotic disease is the major risk factor for cerebrovascular events. Stenosis degree is considered the leading parameter in the choice of therapeutic options; the North American Symptomatic Carotid Endarterectomy Trial (NASCET)4 and European Carotid Surgery Trial5 proved the benefits of performing endarterectomy in those patients with symptomatic high-grade stenosis (70–99%), and proved that the morbidity rate related to the imaging procedure remains low. In 1995, the Asymptomatic Carotid Atherosclerosis Study6 suggested surgery for high-grade asymptomatic stenosis. On the other hand, factors other than the degree of stenosis are also important in assessing whether a carotid lesion will remain clinically silent; plaques that are more prone to disruption or fracture and ulcerated plaques are associated with a higher risk of embolism and occlusion, producing ischemic neurologic events. In the NASCET study, in the group of patients who received medical therapy, 30% of patients who had a severe carotid stenosis associated with an ulcerated plaque suffered an ischemic cerebral event within 2 years, whereas only 17% of patients with severe stenosis but no ulcerated plaques had an ischemic cerebral event within 2 years.4 The presence of ulceration alone represents an important risk for neurologic symptoms,7 and a high-grade stenosis, combined with plaque ulceration, produces an increased risk of stroke.4,8 An accurate delineation of plaque morphology is therefore very important.7,8 Incidence of ulceration in the carotid artery is variable, ranging from 14% to 68%,9–12 and plaque ulceration is significantly more frequent in symptomatic patients.9–12 and plaque ulceration is significantly more frequent in symptomatic patients.11,13 Plaque ulceration has been defined as “an intimal defect larger than 1000-μm in width, exposing the necrotic core of the atheromatous plaque.”14
Conventional angiography has been considered the standard method for evaluating stenosis of the carotid artery, but it is not sufficiently reliable for detecting plaque ulceration15,16 (angiography has a 46% sensitivity and a 74% specificity for detecting ulcerated plaques in large studies17,18). Moreover, conventional angiography is also associated with an increased risk of thromboembolic events.19 Consequently, noninvasive techniques, such as ultrasound (US) echo color Doppler (US-ECD),20,21 MR,22,23 and CT angiography (CTA)18,24 have been more and more frequently used to study carotid artery pathology.
US-ECD is considered by some authors25 a good tool for establishing a final diagnosis and a treatment plan for patients with carotid artery stenosis. CTA, with the introduction of multidetector row CT and sophisticated software for creating 3D images, has become a valid method for studying pathologic lesions of the carotid artery.26 It is accurate in evaluating the degree of carotid stenosis and, compared with digital subtraction angiography, has fewer associated complications. The purpose of this study was to evaluate the diagnostic efficacy of multidetector row CT angiography (MDCTA) and US-ECD in the evaluation of carotid plaque complicated by ulceration through the comparison with surgical specimens.
Materials and Methods
Patient Population
We obtained institutional board approval for this study. From January 2004 to October 2005, 237 consecutive patients (163 men and 74 women; average age, 64 years; age range, 34–87 years), for a total of 474 carotid arteries, were examined with CTA. None of the patients had contraindications to intravenous injection of iodinated contrast material. A history of symptomatic ischemic episodes was found in 104 patients (43.8%; Fig 1); 133 patients (56.2%) were asymptomatic. CTA was performed when a previous US-ECD examination demonstrated a pathologic stenosis and/or a plaque alteration (Fig 2).

A 68-year-old man with TIA. Axial CTA source image (A) and MIP (B) illustrate an ulcerated plaque with a severe stenosis in the right ICA (yellow arrow). Axial head CT scan (C) demonstrates ischemic lesions in the anterior limb of the left internal capsule. On the surgical specimen (D), the ulceration is clearly visible (D). US was negative for ulceration in this case.

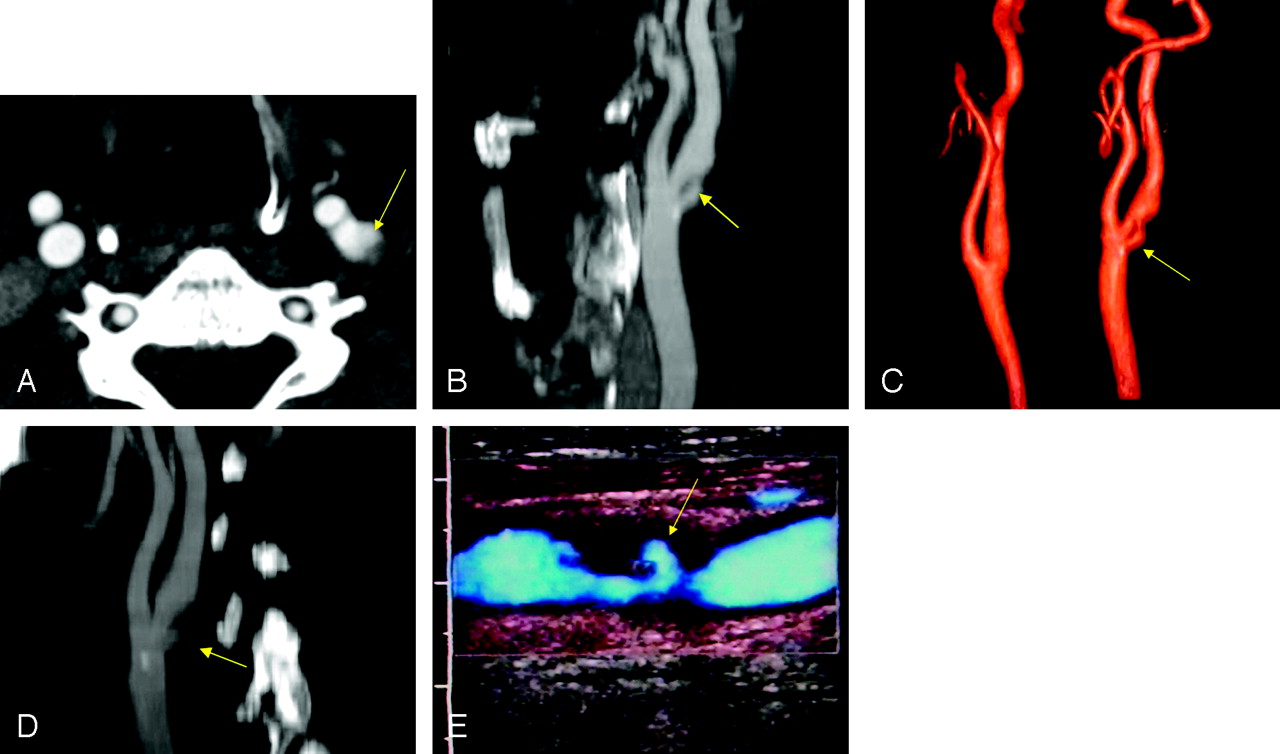
A 71-year-old man with persistent monocular visual loss. Axial scan CTA source image (A), MPR (B), SSD (C), MIP (D), and US-ECD (E) show an irregular ulcerated plaque with moderate stenosis of the ICA. The ulcer is 4 mm and proximal to the point of maximum stenosis (yellow arrows). US was positive for ulceration in this case.
CTA was also performed when ECD could not provide sufficient information about stenosis degree and plaque morphology (ie, in patients with hostile neck [obese patients and those with edema], large calcified plaques with acoustic shadowing [type V plaque at US-ECD], or high carotid bifurcation). CTA examination was obtained within 1 month after US-ECD. Major criteria4,6,27,28 used to decide who had to undergo surgery were as follows: 1) patients with stenosis of >70%; 2) symptomatic patients with stenosis of >50%, with presence, on US-ECD and/or CTA, of intraplaque hemorrhage, fissuration, or an irregular surface; and 3) symptomatic patients with ulceration. US-ECD plaque alteration was defined as the presence of a heterogeneous plaque, irregular surface, and presence of ulceration in the plaque.29 A total of 103 patients underwent surgery (68 men and 35 women; average age, 67 years; age range, 49–85 years). Sixty-seven patients presented with symptoms related to carotid artery lesions, including transient or persistent monocular visual loss, hemispheric transient ischemic attacks (TIAs), and ischemic stroke; 36 patients were asymptomatic.
Imaging: US-ECD and CTA Technique
US-ECD examinations were performed with an Acuson 128 XP/10 (Siemens, Erlangen, Germany) with a 7-MHz linear probe. US-ECD examinations were performed by 1 vascular surgeon and 4 residents.
CTA examinations were performed with a multidetector row spiral CT scanner (Somatom Mx8000; Siemens, Malvern, Pa). After the explanation of the type of investigation, each patient signed an informed consent. To determine the level of the carotid bifurcation and the possible presence of calcification, a CT scan without contrast was obtained, in 5-mm sections, from C2 through C6.30,31 Subsequently, the angiographic acquisition was obtained; arterial enhancement was provided by the intravenous administration in an antecubital vein, through an 18–20 gauge intravenous catheter, of 130 mL of nonionic iodinated contrast material (iopromide [Ultravist 370], Berlex Pharmaceuticals, Richmond, Calif) at an injection speed of 4 mL/s with a power injector. The delay time was 14–18 s, the table speed was 3 mm/s, and the collimation was 3 mm. CT technical parameters included the following: matrix, 512 × 512; FOV, 14–19 cm; mA, 180–200; kV, 120; and section thickness, 1.6 mm. The scan started at the seventh cervical vertebra and proceeded as far cephalad as possible, always including carotid siphon. The total examination time, including preparation of patients, was 10–20 minutes. Axial source images were reconstructed in 1.6-mm increments using 14-cm FOV. Total coverage was 14–18 cm. The window level was preset at 200 HU with a width of 750. Subsequently, the images were processed at a workstation to create multiplanar reconstruction (MPR), shaded surface display (SSD), maximum intensity projection (MIP), and volume-rendered (VR) images (Fig 2). Postprocessing time varied between 10 and 30 minutes.
Image Analysis
To evaluate plaque characteristics in the US-ECD analysis, we used 3 main parameters: plaque echogenicity, plaque surface, and plaque texture. To assess the plaque echogenicity we used the Gray-Weale classification as modified by Geroulakos32,33: type 1 (anechogenic with echogenic fibrous cap), type 2 (predominantly anechogenic but with echogenic areas representing <25% of the plaque), type 3 (predominantly hyperechogenic but with anechogenic areas representing <25% of the plaque), type 4 (echogenic and homogeneous plaque), and type 5 (unclassified plaques reflecting calcified plaques with areas of acoustic shadowing, which hide the deeper part of the arterial layers). We defined the plaque surface as regular and smooth, irregular if we observed variation between 0.3 and 0.9 mm on the contour of the plaque, and ulcerated if we observed an irregularity or break in the surface of the plaque with a depth of ≥1 mm. We characterized the plaque as homogeneous or heterogeneous: we considered a plaque as homogeneous when it showed a uniform consistency irrespective of its echogenicity. We categorized a plaque as heterogeneous when it showed both hypoechogenic and hyperechogenic areas. We considered US-ECD plaque alteration: the presence of a heterogeneous plaque, irregular surface, and presence of ulceration in the plaque. Stenosis degree was evaluated both with the estimation of the area of the residual lumen in transverse section and with the analysis of peak systolic velocity (PSV) and the internal carotid artery (ICA)/common carotid artery PSV ratio.
MDCTA axial images were analyzed with magnifications ranging from 120% to 200% compared with the acquisition. The stenosis of each carotid artery was graded according to the following classification based on the NASCET criteria4: I (normal), II (1%–29% stenosis); III (30%–49% stenosis), IV (50%–69% stenosis), V-a (70%–84% stenosis), V-b (85%–99% stenosis), and VI (occluded). To quantify the degree of the stenosis,34 measurements were made on the axial images perpendicular to the carotid axis.
The value was calculated by comparing the diameter of the stenosed segment with the most distal normal one, where no stenosis was present. We characterized plaque morphology on axial scans with confirmation of our findings on MPR, MIP, VR, and SSD images.
Using internal classification criteria, we studied different plaque types by using axial scans, and we divided them into 3 different groups according to Schroeder et al35: 1) fatty plaques (attenuation <50 HU); 2) mixed plaque (attenuation between 50 and 119 HU); and 3) calcified plaques (attenuation >120 HU). The attenuation was measured in Hounsfield units with the use of a circular or elliptical region of interest cursor in the predominant area of plaque at each level.18
We divided ulcers in relation to their position, referred to the point of maximum stenosis9 as follows: 1) proximal (proximal [upstream] to the point of maximum stenosis); 2) distal (distal [downstream] to the point of maximum stenosis); or 3) level (close to the point of maximum stenosis and therefore unable to be classified with certainty as proximal or distal). Grade of stenosis, carotid plaque surface morphology, presence or absence of ulceration, type of plaque, and plaque position were classified by 2 observers in consensus.
Surgical Specimens
Surgical specimens were characterized by 2 experienced vascular surgeons in consensus. Ulceration was defined as the macroscopic loss of integrity of the intimal layer approximately ≥1 mm in diameter and depth.
Statistical Analysis
We assessed CTA and US-ECD for the following parameters: sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) with their confidence intervals in the evaluation of ulceration of carotid plaque by comparing imaging observations with surgical specimens. To produce these data, we used spreadsheet software (Excel 2003; Microsoft, Redmond, Wash).
Results
CTA
A total of 103 patients underwent carotid endarterectomy after undergoing both US-ECD and CTA examinations. Thirty-two surgical specimens demonstrated ulcerations (Fig 3; 25 men and 7 women; average age, 70 years; age range, 57–81 years; symptomatic, 26; asymptomatic, 6). MDCTA detected 31 ulcerations; 30 correlated with ulcers identified on surgical specimens, and 1 was not confirmed at surgery. These findings resulted in a sensitivity of 93.75%, specificity of 98.59%, PPV of 96.74%, and NPV of 97.2% for CTA in the detection of ulceration (Table 1).

A 65-year-old woman with TIA. Axial scan CTA source image (A), MIP (B), MPR (C), and VR (D) show an ulcerated plaque of the left ICA. Shirt button morphology is visible (B–D). On the surgical specimen, the ulceration is clearly visible (E) (*ICA + CCA, ulceration blue arrow).
Sensitivity, specificity, PPV, and NPV in MDCTA and US-ECD
If we consider the 2 cases of ulcerated plaque not identified by CTA but identified at surgery, CTA probably did not visualize one because it was very small (<2 mm) and the other because abundant plaque calcifications obscured the ulcer. In the 103 patients who underwent surgery, a positive correlation between plaque ulceration and symptoms was found (P=.0206).
US-ECD
US-ECD detected 12 of 32 ulcerations identified at surgery and 6 ulcerations that were not confirmed at surgery. These findings resulted in sensitivity of 37.5%, a specificity of 91.5%, a PPV of 66.7%, and an NPV of 76.5% (Table 1). Of the 12 ulcers detected on US and confirmed at surgery, we most frequently detected ulcers (9 of 12 [75%]) in type 2 plaques. We also noticed that the major number of ulcerations was present in heterogeneous plaques (10 of 12 [83%])
Plaque Characterization
Of the 30 ulcers detected on CTA and confirmed at surgery, 22 were proximal to the point of maximum stenosis, 6 were at the same level of maximum stenosis, and 2 were distal to the point of maximum stenosis. Twenty-one ulcers were in the ICA, 6 ulcers were in the bulb, and 3 ulcers were in the common carotid artery (Table 2). The incidence of plaque ulceration increased with the severity of carotid artery stenosis: 1 ulceration was in group IV (1 of 6 [16.6%]), 7 ulcerations were in group V-a (7 of 31 [22.6%]), and 22 ulcerations were in group V-b (22 of 66 [33.4%]). When we analyzed the incidence of ulceration for each plaque type (fatty, mixed, and calcified), we observed that the number of ulcerations was highest in fatty plaques and was uncommon in calcified plaques (Table 3).
Position of the ulcers relative to the point of maximum stenosis in MDCTA
Incidence of ulceration in fatty, mixed, and calcified plaques in MDCTA
Discussion
The purpose of this study was to evaluate the diagnostic efficacy of MDCTA and US-ECD in the evaluation of carotid plaque complicated by ulceration through the comparison with surgical specimens. Although extracranial carotid artery stenosis is accepted as a significant risk factor for cerebrovascular events, plaque morphology may also contribute to this risk. The degree of stenosis is related only indirectly to the occurrence of cerebral infarction. The concept of “vulnerable plaque”36 has been postulated for coronary arteries37; according to our results, it may be also applicable to the carotid arteries. The vulnerable plaque refers to an atherosclerotic plaque that contains a large necrotic lipid core covered by a thin or disrupted fibrous cap, and it is characterized by a higher tendency to rupture, resulting in embolization or thrombosis. Even low-grade stenosis can result in cerebrovascular events, so it is fundamental to look beyond degree of stenosis38 and to characterize plaque morphology. Many authors have studied plaque ulceration with digital subtraction angiography,39,40 but few have studied plaque ulceration with CTA.24
We demonstrated that MDCTA has a very a high sensitivity (93.75%) and specificity in detecting carotid artery plaque ulcerations. The sensitivity that we reported is higher compared with the works of Link et al,41 Schwartz et al,42 Debernardi et al,24 Oliver et al,10 and Walker et al18; in these works, however, single-section CT scanners were used. We performed CTA examinations with a multidetector row scanner, and we studied each examination with axial and multiple postprocessed reconstructed images (MIP, MPR, SSD, and VR). Moreover, CTA is far superior to US-ECD in detecting ulcerations. In our work, US-ECD sensitivity in detecting ulcers was only 37.5%; these values are similar to data produced by other authors.24,43,44 This can be ascribed, in part, to the fact that acoustic shadowing from calcification obscures ulcers, and the sonography probe may not be parallel to the axis of the vessel in the region of the ulceration. In our radiology practice, we always looked for ulceration when we analyzed carotid arteries, and considering the high MDCTA sensitivity and specificity, a radiologist should look for plaque ulcerations.
CTA also provided useful information with respect to carotid plaque characteristics. We observed that ulcerations in carotid plaques are usually proximal to the point of maximum stenosis (Fig 1B). These data confirmed previous angiographic work of Lovett and Rothwell9 and stress that radiologists should look for plaque ulceration proximal to the point of maximum stenosis. Distal ulcerations are uncommon. Furthermore, we demonstrated that ulcerations are much more common in fatty versus calcified plaques and confirmed the results of Walker et al.18 The relationship between plaque morphology and clinical behavior in the carotid circulation has been incompletely studied, but it has been demonstrated that cerebral infarcts are more frequent in patients with a lipid core than in patients without a lipid core.33 The presence of a lipid core is significantly associated with cerebral infarction on MR imaging, and particular centrum semiovale infarcts are more frequent than cortical ones. Indeed, calcified carotid artery atherosclerotic plaques are less symptomatic than those that are noncalcified.11 Calcium likely confers stability to the plaque, resulting in protection against biomechanical stress and subsequent complications as ulcerations. We also demonstrated that the number of plaque ulcerations increased with severity of stenosis: in fact, in our patient cohort, we observed that 16.6% of carotid arteries with a stenosis degree between 50% and 69% showed ulceration, whereas 33% of carotid arteries with a stenosis degree of 85%–99% showed ulceration.
Determining the presence of an ulceration is particularly important in the moderate stenosis group, because it may change the therapeutic approach. In addition, in the presence of a plaque ulceration, surgeons tend to manipulate carotid arteries with greater carefulness.
We faced some difficulties during the evaluation of CTA images: artifacts on volumetric images because of patient swallowing, the presence of large calcified plaques that produced beam hardening artifacts, and bone structures that could not be separated from the carotid artery on reformatted images, On multidetector row CT, because of the high velocity of acquisition, these artifacts occur with a lesser frequency compared with conventional CT scanners. However, very small ulcerations can still be obscured by any of these artifacts. In particular, we agree with other authors42,45 that calcified plaque is the major limitation of CTA in studying plaque morphology and detecting ulcerations.
We observed an incidence of carotid plaque ulceration of 31.06% (32 ulcers in 103 surgical specimens) in the surgical group. These values appear to be similar to the incidence values described by other authors. In fact, in the pathologic study of Fisher et al,11 where they analyzed 241 plaques, the authors found 59 ulcers with an incidence of 25%. In the angiographic study of Lovett and Rothwell,9 the authors, by analyzing 3007 angiograms, found 421 ulcers (14%). In the pathologic study of Rothwell et al,12 authors described that macroscopic ulceration were detected in 1132 cases (1671 patients [68%]).
Limitations of the study are as follows. There was a selection bias: a large number of patients who underwent a US-ECD examination did not undergo CTA, so that there are no data about sensitivity and specificity of CTA in detecting ulceration in those patients who were not included in this study. Another limitation was that we did not perform carotid endarterectomy in all 237 of the patients who had CTA and US-ECD performed; this fact determined the impossibility of surgically evaluating the presence of ulcerations in 134 patients.
A third limitation was the use of direct visualization of the surgical specimen as reference standard: histopathologic examination would likely have been more accurate. Another bias in this work was the fact that vascular surgeons were not blinded to the sonography and CTA results before surgery.
Conclusions
Results of our study suggest that MDCTA detects with high sensitivity and specificity the presence of ulcerated plaque, whereas US-ECD suffers in this evaluation. Considering the high MDCTA sensitivity and specificity for detection of plaque ulceration, we therefore recommend MDCTA as a useful step for correct presurgical planning.
References
- Received June 7, 2006.
- Accepted after revision November 1, 2006.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Asymptomatic carotid artery stenosis: a summary of current state of evidence for revascularization and emerging high-risk features
- Asymptomatic carotid artery stenosis: a summary of current state of evidence for revascularization and emerging high-risk features
- Carotid Vessel Wall Imaging on CTA
- Carotid Artery Wall Imaging: Perspective and Guidelines from the ASNR Vessel Wall Imaging Study Group and Expert Consensus Recommendations of the American Society of Neuroradiology
- CT Attenuation Analysis of Carotid Intraplaque Hemorrhage
- Imaging Carotid Atherosclerosis Plaque Ulceration: Comparison of Advanced Imaging Modalities and Recent Developments
- Swirling of microbubbles: Demonstration of a new finding of carotid plaque ulceration on contrast-enhanced ultrasound explaining the arterio-arterial embolism mechanism
- CTA for Screening of Complicated Atherosclerotic Carotid Plaque--American Heart Association Type VI Lesions as Defined by MRI
- Carotid Artery Wall Thickness Measured Using CT: Inter- and Intraobserver Agreement Analysis
- Comparison of Carotid Plaque Ulcer Detection Using Contrast-Enhanced and Time-of-Flight MRA Techniques
- Distribution of Inflammation Within Carotid Atherosclerotic Plaques With High-Risk Morphological Features: A Comparison Between Positron Emission Tomography Activity, Plaque Morphology, and Histopathology
- Carotid Plaque Enhancement and Symptom Correlations: An Evaluation by Using Multidetector Row CT Angiography
- Associations between Carotid Artery Wall Thickness and Cardiovascular Risk Factors Using Multidetector CT
- Characterization of Carotid Plaque Hemorrhage: A CT Angiography and MR Intraplaque Hemorrhage Study
- Urgent Carotid Endarterectomy: The Role of Serial Ultrasound Studies in Early Detection of Plaque Rupture