
Abstract
SUMMARY: Posterior reversible encephalopathy syndrome (PRES) is a neurotoxic state coupled with a unique CT or MR imaging appearance. Recognized in the setting of a number of complex conditions (preeclampsia/eclampsia, allogeneic bone marrow transplantation, organ transplantation, autoimmune disease and high dose chemotherapy) the imaging, clinical and laboratory features of this toxic state are becoming better elucidated. This review summarizes the basic and advanced imaging features of PRES, along with pertinent features of the clinical and laboratory presentation and available histopathology. Many common imaging/clinical/laboratory observations are present among these patients, despite the perception of widely different associated clinical conditions.
Initially recognized in association with eclampsia, cyclosporine after transplantation, and in the setting of severe hypertension, posterior reversible encephalopathy syndrome (PRES) has become synonymous with a unique pattern of brain vasogenic edema seen in the setting of neurotoxicity.1-14 On CT or MR imaging studies, the edema is often widespread but predominates in the parietal and occipital regions, likely leading Hinchey et al15 to suggest the “posterior” description.
A substantial experience with PRES has evolved; and though more widely recognized, controversy still exists as to the mechanism responsible for the brain edema. Specifically, what is the role of hypertension and is the edema related to hyperperfusion or hypoperfusion? In this review, the fundamental clinical and imaging features of PRES will be emphasized with controversial issues to follow.
Imaging Patterns in PRES
At CT/MR imaging, the brain typically demonstrates focal regions of symmetric hemispheric edema (Fig 1A, -B). The parietal and occipital lobes are most commonly affected, followed by the frontal lobes, the inferior temporal-occipital junction, and the cerebellum.16-18 Lesion confluence may develop as the extent of edema increases. MR diffusion-weighted imaging (DWI) was instrumental in establishing and consistently demonstrating that the areas of abnormality represent vasogenic edema.19-24 The edema usually completely reverses.

The patient is a 28-year-old man with a history of alcohol abuse and drug use, presenting with a necrotic pneumonia and empyema growing Pseudomonas and Klebsiella species. He developed altered mentation and asymmetric neurologic findings on examination. Blood pressure at toxicity fluctuated between 130/100 mm Hg and 130/77 mm Hg. A and B, Axial MR images (fluid-attenuated inversion recovery) demonstrate extensive vasogenic edema in the frontal lobes (arrows), parietal region (curved arrows), occipital lobes (open arrows), and temporal lobes (arrowheads), bilaterally, consistent with PRES. The edema distribution clearly separates medial (ACA and PCA) from lateral (MCA) hemispheric regions typical of the holohemispheric PRES pattern. Cerebellar involvement was also present (not shown). C, Lateral view of the left internal carotid artery injection with left and right ACA opacification. Areas of vessel dilation and constriction are noted in the secondary and tertiary branches of both medial hemispheric vessels (left [arrows] and right [arrowheads] ACAs) and lateral hemispheric vessels (left MCA [curved arrows]) consistent with vasculopathy. D, Lateral view of the vertebral artery CA injection demonstrates a string-of-beads appearance (arrowheads) and areas of vasodilation/vasoconstriction (arrows) in parietal branches of the PCA. E, Oblique 3D TOF MRA reconstructed images of the posterior circulation demonstrate areas of focal vasodilation and vasoconstriction in the PCAs bilaterally (arrows), consistent with vasculopathy, similar to the vertebral artery CA appearance. Posterior inferior cerebellar artery (arrowheads) irregularity is also present.
The basic PRES pattern resembles the brain watershed zones, with the cortex and subcortical and deep white matter involved to varying degrees.12,14,16,25,26 Three hemispheric pattern variants may be encountered with similar frequency (holohemispheric [Fig 1], superior frontal sulcal, and primary parietal-occipital).27 These demarcate lateral hemispheric blood supply (middle cerebral artery [MCA]) and medial hemispheric supply (anterior cerebral artery [ACA], posterior cerebral artery [PCA]) and further reflect the junctional/watershed nature of PRES.
Characteristic lesion locations such as the inferior temporal-occipital junction, superior frontal sulcus, and parietal/occipital region likely represent junctional expression between second-order branches or distal hemispheric branches.16 Linearly oriented focal deep white matter involvement may represent expression of PRES in the deep (intrahemispheric) watershed.27 A continuum is noted between diminutive and extensive expression of PRES; and partial, asymmetric, or mixed forms of these patterns may be encountered.
Focal/patchy areas of PRES vasogenic edema may also be seen in the basal ganglia, brain stem, and deep white matter (external/internal capsule).20,27-31 When they accompany hemispheric or cerebellar PRES, it is easy to recognize these areas as companion lesions. Present in isolation or when the hemispheric pattern is incompletely expressed (partial/asymmetric), the diagnosis of PRES can be challenging.27,32 If cerebellar or brain stem involvement are extensive, hydrocephalus and brain stem compression may occur.33-35
Focal areas of restricted diffusion (likely representing infarction or tissue injury with cytotoxic edema) are uncommon (11%–26%) and may be associated with an adverse outcome.20,21 Hemorrhage (focal hematoma, isolated sulcal/subarachnoid blood, or protein) is seen in approximately 15% of patients.16,27,32
Basic Clinical Features of Neurotoxicity with PRES
Patients at risk for PRES are summarized in the Table. Neurotoxicity with characteristic watershed CT/MR imaging features was initially noted in eclampsia, allogeneic bone marrow transplantation (allo-BMT), solid organ transplantation (SOT), and in association with severe hypertension. With similar clinical/imaging presentation recognized the mid 1990s, additional associations were noted (autoimmune conditions, thrombotic thrombocytopenic purpura, and medical renal disease), and the term “PRES” was introduced.15,20,22 PRES is seen with unique or high-dose cancer chemotherapy (Table) and has recently been associated with infection, sepsis, and shock.36 Additional considerations have been suggested in numerous case reports as reviewed in the Table.
Conditions at risk for PRES
Clinical/Laboratory Characteristics in PRES
Clinical symptoms at toxicity are broad but include headache, vision change, paresis, hemianopsia, nausea, and altered mentation.37,38 Symptoms may develop over several days or may be recognized only in the acute setting. Generalized seizures are common and coma may develop. In approximately 70%–80% of patients, moderate-to-severe hypertension is observed. Toxicity blood pressure is normal or only minimally elevated in 20%–30% of patients in eclampsia, allo-BMT, and most large reported PRES series.11,15,17,22,27,39-42
Best studied in preeclampsia/eclampsia, laboratory evidence of endothelial injury is often present with platelet consumption (thrombocytopenia) and evidence of red cell fragmentation (schistocyte formation, increase in lactate dehydrogenase [LDH]).43,44 Developing hypertension in preeclampsia is related to systemic vasoconstriction with accompanying reduced intravascular volume and hemoconcentration. Renal dysfunction with proteinuria and hypomagnesemia occur; systemic edema develops due to a combination of altered endothelial function and reduced oncotic pressure. Hepatic ischemia may lead to liver dysfunction and, when severe, hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome.
In infection/sepsis/shock–associated PRES, a clinical pattern consistent with systemic inflammatory response syndrome develops with evidence of multiple organ dysfunction syndrome (MODS), including alteration of coagulation (thrombocytopenia), liver function (increased bilirubin), renal function (increased creatinine), pulmonary function, and cardiovascular instability.36
Similar features may develop in patients after allo-BMT. The effects of graft-versus-host disease (GVHD) are managed by immune suppression with cyclosporine or tacrolimus (FK-506). Cyclosporine can injure the endothelium.45,46 At toxicity, diffuse endothelial dysfunction is often present, termed “bone marrow transplant thrombotic microangiopathy,” with development of significant schistocyte counts (exceeding 10% when severe) and marked elevation of LDH.16,17,47 A MODS pattern can develop with systemic or pulmonary edema and ischemic hepatic dysfunction, similar to preeclampsia.48
Major PRES-Associated Clinical “Conditions”
Preeclampsia/Eclampsia.
The association of PRES with toxemia of pregnancy is well established.1-3,5,21,24,26,49,50 Preeclampsia develops in approximately 5% of pregnancies and eclampsia, in approximately 1 in 3000 births with current management.43,44 Eclampsia develops before gestation in 50% of patients, interpartum in 25%, and within 48 hours of delivery in 25%. Although most women are hypertensive at toxicity, blood pressure is reported as normal or only minimally elevated in 23% of patients.39 The placenta is thought to be the primary cause of toxemia, with placenta removal and fetal delivery considered curative.43,44
“Delayed Eclampsia” (PRES within several weeks after delivery) can occur, and the clinical presentation is often confusing.4,51 Blood pressure may be normal or mildly elevated, severe headache is common, and conventional angiography is often performed to exclude intracranial aneurysm. In a recently reported case, delayed eclampsia appeared to have been associated with retained placental fragments.52 PRES has also been reported 3 weeks following resection and chemotherapy for hydatidiform mole.53
Infection/Sepsis/Shock.
In infection, sepsis, and shock–associated PRES, gram-positive organisms predominate, and in 40% of patients, toxicity blood pressure is normal or only minimally increased.36 At imaging, vasogenic edema is greater in normotensive patients and lower in severely hypertensive patients; and at MR angiography (MRA), reversible “vasculopathy” (diffuse/focal vasoconstriction) or vessel pruning is noted.36 Recent reports note PRES in the setting of post-streptococcal glomerulonephritis, Henoch-Schonlein purpura, and infection-induced hypercoagulable state.54-56
Autoimmune Disease.
PRES has been identified in patients with systemic lupus erythematosus, Wegener's granulomatosis, systemic sclerosis (scleroderma, Fig 2), and polyarteritis nodosa.15,20,22,27,57-60 Detailed accounts of the clinical circumstances surrounding PRES in association with autoimmune disease are infrequent.57-60 Patients are commonly managed with intermittent doses of immunosuppression (cyclophosphamide, cyclosporine) for disease control.

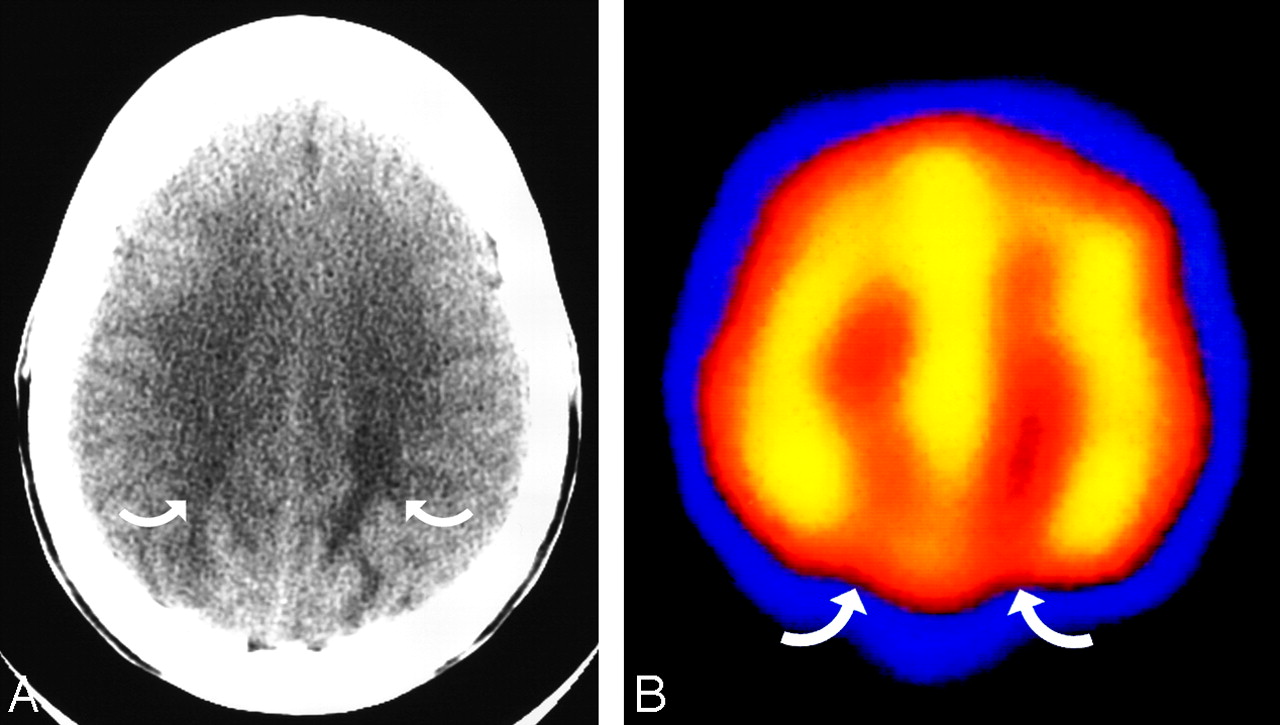
The patient is a 38-year-old woman with scleroderma, severe hypertension (190/110 mm Hg), and acute renal failure, with altered mental status that progressed to seizure. A, Axial brain CT image obtained at toxicity demonstrates vasogenic edema in the parietal region bilaterally (curved arrows), consistent with PRES. B, Axial technetiumTc-99m-HMPAO SPECT study performed the following day demonstrates reduced radiopharmaceutical uptake bilaterally in the parietal region (curved arrows), consistent with hypoperfusion.
Cancer Chemotherapy.
PRES is usually encountered after high-dose multidrug cancer therapy, typically in hematopoietic malignancies.61-64 A variety of cancer chemotherapeutic drugs have also been noted in association with PRES (Table).
Transplantation.
PRES is well recognized in the setting of bone marrow or stem cell transplantation.11,17,18,65-68 The incidence of PRES after allo-BMT using myeloablative marrow preconditioning and cyclosporine immune suppression is approximately 7%–9% and appears to vary with a preconditioning regimen.11,67,69 A greater frequency (16%) is reported with higher dose myeloablative regimens, and a lower frequency (3%) is noted with nonmyeloablative preconditioning.65,69 PRES occurs most commonly in the first month after allo-BMT, with the remainder during the subsequent year after transplantation.11,40,67,69 Reported incidence of PRES with tacrolimus immune suppression appears variable.66,68 A high incidence of GVHD is also noted in patients with allo-BMT PRES, and a GVHD effect has been suggested.68,70-72 Variation in cyclosporine toxicity with human leukocyte antigen match has been noted, and the rate of tacrolimus-associated PRES appears to increase with the degree of graft mismatch.66,67
PRES is also noted after SOT.9,12,13,34,40,73-80 The reported incidence of PRES after SOT varies between 0.4% and 6%.78,81 The onset of PRES varies among subtypes but tends to occur earlier after liver transplantation.81 Systemic hypertension was found to be common in patients who develop PRES after renal transplantation but uncommon after heart, lung, or liver transplantation.77,81,82 In our experience, transplant rejection and infection often accompany PRES in SOT.83 After liver transplantation, PRES typically occurs early (within 2 months after transplantation), blood pressure tends to be normal, and the extent of brain edema is significant. In contrast, patients with kidney transplantation appear to develop PRES late after transplantation, are severely hypertensive, and have significantly less brain edema.83
After transplantation, several PRES-related risks coexist. The immune-suppressive drugs cyclosporine/tacrolimus (FK-506) inhibit T-cell activation, proliferation, and interleukin-2 production through inhibition of the calcineurin pathway.84,85 These drugs are associated with low-level neurotoxicity in 10%–40% of patients (tremors, anxiety, psychiatric dysfunction).37,86 Immunosuppressant blood levels do not appear to correlate with severe neurotoxicity or PRES, but immunosuppressant discontinuation or switch usually results in clinical improvement.11,37,67,69,77,86,87 Cyclosporine can induce endothelial injury/dysfunction leading to enhanced vasoconstrictive effects (increased endothelin and thromboxane, decreased nitric oxide and prostacycline), increased sympathetic activation, and coagulation effects.37,45-47,84,88 Immune challenge from the transplant (transplant rejection, GVHD), effects of chemotherapy (preconditioning), and the risks of infection in the immunosuppressed state may further contribute to toxicity. Clearly, a balance exists between adequate immunosuppression and infection risk.
Hypertension.
PRES is commonly seen in the setting of hypertension. The upper limits of autoregulation are not typically reached, but moderate-to-severe hypertension is seen in approximately 75% of patients with PRES. Often termed “hypertensive encephalopathy,” the reported imaging patterns can vary.6-8,35,89-93 Areas of deep white matter abnormality have been noted, which may overlap with lacunar disease and may relate to the known histologic findings in hypertension.8,93,94 Hemispheric PRES patterns have been reported as well as isolated reversible brain stem and cerebellar edema, occasionally resulting in obstructive hydrocephalus.35
Recurrent PRES
Recurrent PRES has been anecdotally reported in severe hypertension and after allo-BMT.66,80 In a recent reported series, recurrent PRES was noted in 3 (3.8%) of 78 patients and was associated with sickle-cell disease with infection, allo-BMT with infection, or atypical autoimmune disease and possible viral infection.95 Recurrent eclampsia is well recognized with a reported incidence of ∼2% of live births.96
Histopathology in PRES
Histologic evaluation of PRES is uncommon and often obtained late in the course of complex systemic disease. Biopsy/autopsy obtained during acute toxicity demonstrates vasogenic edema, paralleling observations on DWI.17,76,97-99 Activated/reactive astrocytes, scattered macrophages, and lymphocytes have been often noted without inflammation, ischemia, or neuronal damage. Late autopsy studies have generally demonstrated evidence of demyelination and myelin pallor along with evidence of ischemia, neuronal anoxic damage, laminar necrosis, or older hemorrhage in the white matter and cortex.11,13,17,100
Evidence of acute and chronic vessel injury has been described in late autopsy studies with identification of intimal thickening, segmental vessel narrowing, intimal dissection, and organized thrombi.11,101 Acute vasculopathy has also been described in a patient with a liver transplant with vessel inflammation and adjacent deep basal ganglia and periventricular infarction.102
Advanced Imaging in PRES
Cerebral Blood Vessels in PRES
At catheter angiography (CA), diffuse vasoconstriction, focal vasoconstriction, vasodilation, and even a string-of-beads appearance have been noted in PRES, consistent with what is typically described as vasospasm or arteritis (Fig 1C, -D).2,4,14,51,54,103,104 Reported blood pressure in most of these patients demonstrated moderate but not severe hypertension (mean arterial pressure <130 mm Hg). CA in PRES is typically performed in eclampsia, delayed eclampsia, and after cancer chemotherapy, usually in the setting of a clinical presentation in which aneurysm is suspected.
At MRA using a 3D time of flight (TOF) technique, patterns resembling vasculopathy have been noted, with vessel irregularity consistent with focal vasoconstriction/vasodilation and diffuse vasoconstriction (Fig 1E).17,36,60,95,103,105-108 When performed, repeat MRA often demonstrates reversal of the vasculopathy. In normotensive patients, vessels may appear normal or demonstrate pruning of distal intracranial branches, in particular the PCAs.36
Abnormal internal carotid or vertebral arteries have, on occasion, been noted in PRES, with intimal irregularity resembling fibromuscular disease demonstrated by CA in delayed eclampsia and dissection noted in PRES on MRA.51,109 These CA/MRA features reflect previously described vessel histologic observations. MR venography has tended to be normal in PRES.107
Cerebral Blood Flow in PRES
The state of brain blood flow in PRES remains controversial (Review, Part 2). Vasoconstriction seen by CA in early studies prompted the authors to postulate that reduced brain perfusion led to the imaging features. In contrast, animal studies suggested that experimentally induced hypertension above the autoregulatory limit (mean arterial pressure >150–160 mm Hg) led to hyperperfusion, breakdown of the blood-brain barrier, and hemispheric edema.
Hyperperfusion was suggested in a single patient with PRES and Wegener's in an early study using technetium Tc99m-hexamethylpropyleneamine oxime (Tc99m-HMPAO) single-photon emission CT (SPECT), with a second patient (eclamptic) demonstrating variable radiotracer distribution.18 In a later study, increased Tc99m-HMPAO SPECT activity suggesting hyperperfusion was reported in a single patient with a molar pregnancy and eclampsia.110 In patients with aneurysmal subarachnoid hemorrhage and vasospasm, Tc99m-HMPAO studies demonstrated patterns of variable perfusion.111 Increased radiopharmaceutical activity in Tc99m-HMPAO brain studies has been noted in many circumstances associated with stroke but remains controversial.112
In contrast, watershed hypoperfusion has been demonstrated by using Tc99m-HMPAO SPECT in a large series of women with eclampsia, with focal hypoperfusion also noted after chemotherapy and in autoimmune disease (Fig 2).63,113 Reduced perfusion has also been demonstrated using MR perfusion (MRP) in PRES (Fig 3).103,114,115 Cortex and white matter relative cerebral blood volume (rCBV) has been shown to be reduced moderately in areas of PRES (average, 65%), when compared with normal uninvolved regions in 2 studies.103,115 Comparing anterior-to-posterior hemispheric flow, Brubaker et al114 found that MRP has also demonstrated significant posterior brain hypoperfusion with increased mean transit time, reduced CBV, and reduced cerebral blood flow.114 Critical cortex hypoperfusion (12.2 mL/100 g brain per minute) has been demonstrated by stable xenon CT after blood pressure reduction in a child with hypertensive encephalopathy and PRES, which partially reversed with re-established moderate hypertension (mean arterial pressure, 114 mm Hg).116

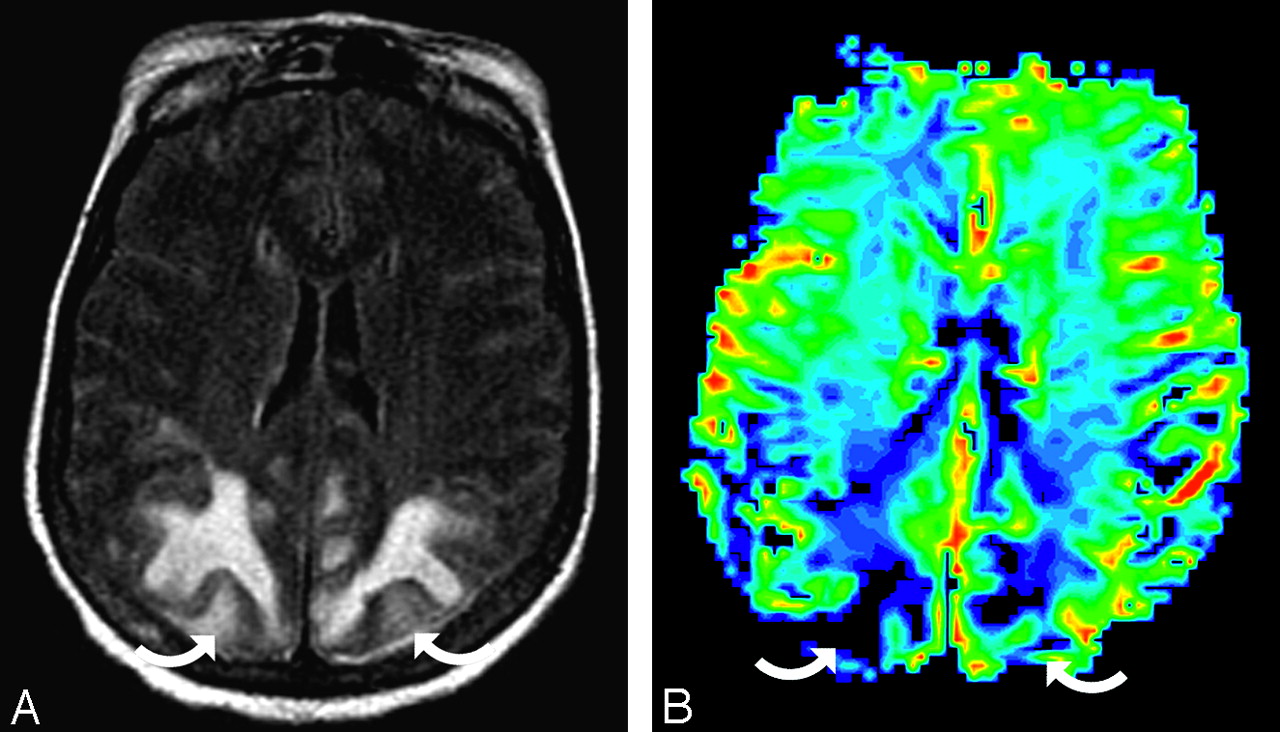
The patient is a 56-year-old woman with a thigh abscess (Klebsiella and Enterococcus species), baseline blood pressure of 156/68 mm Hg, and multiple organ failure (coagulopathy, acute respiratory distress syndrome, hepatic dysfunction with shock liver, and renal failure). She developed altered mentation and a seizure with toxicity blood pressure 164/75 mm Hg. A, Axial MR image (fluid-attenuated inversion recovery sequence) demonstrates extensive PRES vasogenic edema in the parietal region bilaterally (curved arrows). B, rCBV color map demonstrates severe flow reduction in the parietal region bilaterally (curved arrows), consistent with the regions of PRES imaging abnormality. PRES cortex rCBV relative to the reference cortex is 31% in the right parietal and 33% in the left parietal region.
Proton MR Spectroscopy in PRES
Reduced N-acetylaspartate:choline and N-acetylaspartate:creatinine ratios have been described by MR spectroscopy in regions of PRES vasogenic edema as well as in unaffected regions.107,117,118 Quantitative metabolite assessment in 2 patients demonstrated an absolute reduction of metabolite concentration (considered a dilution effect from vasogenic edema), which corrected in 1 patient on follow-up MR spectroscopy.117 Abnormal metabolite ratios may persist.107 Lactate has been reported in PRES, and when accompanied by vasoconstriction, a contribution from ischemia has been suggested.42,107
The Controversy over the Mechanism of PRES
The cause of PRES is not yet understood. Hypertension with failed autoregulation and hyperperfusion remains a popular consideration for the developing brain edema.18,92,119,120 Alternatively, endothelial dysfunction/injury, hypoperfusion, and vasoconstriction may lead to altered integrity of the blood-brain barrier.4,121,122
Although commonly cited, several problems exist with the hypertension/hyperperfusion theory. PRES is seen in the absence of hypertension in 20%–40% of patients.17,27,36,39 In the remainder, though some degree of hypertension is present, reported blood pressure does not typically reach the limit of autoregulation (mean arterial pressure >150–160 mm Hg).123 Also, several recent studies have noted less vasogenic edema in severely hypertensive patients when compared with normotensive patients, contrary to the expected result if severe hypertension with failed autoregulation was the mechanism behind PRES.36,103 The biologic observations (strengths/weaknesses) related to both theories will be reviewed in detail in Part 2.
Conclusion
PRES develops in patients with complex systemic conditions such as eclampsia, after transplantation, in infection/sepsis/shock and autoimmune disease, and after cancer chemotherapy. Hypertension is absent in ∼25% of patients and, when present, does not typically reach the level of failed autoregulation. The imaging appearance typically demonstrates symmetric vasogenic edema with several characteristic patterns, generally representing a distribution between lateral and medial cerebral arterial branches (ie, a watershed distribution). Vasculopathy is commonly identified by CA or MRA, and most studies have demonstrated reduced brain perfusion in regions of PRES. The mechanism responsible for the imaging appearance remains unclear and controversial.
References
- Received November 5, 2007.
- Accepted after revision November 5, 2007.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- COVID-19-Associated PRES-like Encephalopathy with Perivascular Gadolinium Enhancement
- Posterior reversible encephalopathy syndrome (PRES): presentation, diagnosis and treatment
- Posterior reversible encephalopathy syndrome associated with the use of chemotherapeutic agents: a rare complication after treatment with vinorelbine
- Delayed Leukoencephalopathy: A Rare Complication after Coiling of Cerebral Aneurysms
- Tumour-like presentation of atypical posterior reversible encephalopathy syndrome with prominent brainstem involvement
- Encephalopathy in a kidney transplant recipient
- Posterior reversible encephalopathy syndrome due to hypercalcaemia: a rare cause
- Controversy of posterior reversible encephalopathy syndrome: what have we learnt in the last 20 years?
- Reversible brain lesion following growth hormone replacement therapy in an adolescent
- Oxaliplatin-induced posterior reversible encephalopathy syndrome (PRES)
- Glucocorticoid-associated worsening in reversible cerebral vasoconstriction syndrome
- Republished: Posterior reversible encephalopathy syndrome with thalamic involvement during vasopressor treatment of vertebrobasilar vasospasm after subarachnoid hemorrhage
- Distinguishing Neuroimaging Features in Patients Presenting with Visual Hallucinations
- Utility and Significance of Gadolinium-Based Contrast Enhancement in Posterior Reversible Encephalopathy Syndrome
- Clinical outcomes and risk factors for posterior reversible encephalopathy syndrome in systemic lupus erythematosus: a multicentric case-control study
- Posterior Reversible Encephalopathy Syndrome as an Overlooked Complication of Induced Hypertension for Cerebral Vasospasm: Systematic Review and Illustrative Case
- Management of Posterior Reversible Encephalopathy Syndrome Induced by Carfilzomib in a Patient With Multiple Myeloma
- Posterior reversible encephalopathy syndrome with thalamic involvement during vasopressor treatment of vertebrobasilar vasospasm after subarachnoid hemorrhage
- Generalised reversible encephalopathy syndrome: a variant of posterior reversible encephalopathy syndrome (PRES)
- Cytotoxic Edema in Posterior Reversible Encephalopathy Syndrome: Correlation of MRI Features with Serum Albumin Levels
- Reversible cerebral vasoconstriction syndrome: a rare cause of postpartum headache
- Neuroimaging Features and Predictors of Outcome in Eclamptic Encephalopathy: A Prospective Observational Study
- Clinical Reasoning: Progressive visuospatial problems in a 71-year-old man
- The challenges of antiphospholipid syndrome: experience from diagnosis to self-care
- Lesson of the month (2): All that glitters is not stroke
- Posterior reversible encephalopathy syndrome (PRES) in a patient with late postpartum eclampsia
- Imaging Characteristics of Ischemic Strokes Related to Patent Foramen Ovale
- Clinicopathologic and MRI Characteristics of Presumptive Hypertensive Encephalopathy in Two Cats and Two Dogs
- Posterior Reversible Encephalopathy Syndrome: More Than Meets the Eye
- Changes in Ophthalmic Artery Doppler Indices in Hypertensive Disorders During Pregnancy
- Posterior reversible encephalopathy syndrome after bevacizumab therapy in a normotensive patient
- First reported case of posterior reversible encephalopathy syndrome occurring in a weightlifter
- The many faces of posterior reversible encephalopathy syndrome
- Neurotoxicology: Five new things
- Posterior Reversible Encephalopathy Syndrome: A Truly Treatable Neurologic Illness
- Posterior reversible encephalopathy syndrome: the importance of early diagnosis
- Multimodal Imaging of Reversible Cerebral Vasoconstriction Syndrome: A Series of 6 Cases
- The posterior reversible encephalopathy syndrome in HIV infection
- A review of the clinical presentation, natural history and inheritance of variegate porphyria: its implausibility as the source of the 'Royal Malady'
- Reversible Posterior Leukoencephalopathy in a Venomous Snake (Bothrops asper) Bite Victim
- Posterior Reversible Encephalopathy Syndrome During Ipilimumab Therapy for Malignant Melanoma
- Reversible Cerebral Vasoconstriction Syndrome: Treatment with Combined Intra-Arterial Verapamil Infusion and Intracranial Angioplasty
- Short-Term Effects of Rituximab in Children with Steroid- and Calcineurin-Dependent Nephrotic Syndrome: A Randomized Controlled Trial
- The posterior reversible encephalopathy syndrome: what's certain, what's new?
- Suspicious Neuroimaging Pattern of Thrombotic Microangiopathy
- Life imitates art: Anti-amyloid antibodies and inflammatory cerebral amyloid angiopathy
- Isolated Acute Nontraumatic Cortical Subarachnoid Hemorrhage
- Influenza A Encephalopathy, Cerebral Vasculopathy, and Posterior Reversible Encephalopathy Syndrome: Combined Occurrence in a 3-Year-Old Child
- ASYMPTOMATIC SPINAL CORD INVOLVEMENT IN POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME
- Reversible cerebral vasoconstriction syndrome
- Hemorrhage in Posterior Reversible Encephalopathy Syndrome: Imaging and Clinical Features
- Reversible posterior leukoencephalopathy syndrome caused by hanging
- MR Imaging Findings of Medulla Oblongata Involvement in Posterior Reversible Encephalopathy Syndrome Secondary to Hypertension
- Reversible Encephalopathy after Cardiac Transplantation: Histologic Evidence of Endothelial Activation, T-Cell Specific Trafficking, and Vascular Endothelial Growth Factor Expression