
A primary manifestation of a highly malignant B-cell lymphoma is an important, albeit uncommon, cause of radiculopathy. Rarely, a primary central nervous system lymphoma (PCNSL) disseminates outside the central nervous system (CNS) as seen in the patient described in this case.
A previously healthy 79-year-old man presented with a progressive paresis and proximal paresthesia of the left lower extremity. Neurologic examination demonstrated paresis in the muscles innervated by the left L3, L4, and L5 nerve roots, absence of the Achilles tendon reflex, and sensory disturbances in the left dermatomes of L4 and L5. Other neurologic functions were intact. Except for a slightly increased erythrocyte sedimentation rate and a decreased absolute lymphocyte count, blood test results were negative or within normal limits. Initial examination of the CSF showed lymphocytic pleocytosis (0.143 × 109 cells/L), an elevated protein level (1130 mg/L), and a mildly depressed glucose concentration (2.6 mmol/L). Bacterial and mycobacterial cultures were negative, as were the tests for Borrelia organisms, syphilis, herpes simplex virus, and Epstein-Barr virus. CSF cytology was negative for malignancy. Electromyography and nerve conduction studies revealed a sensorimotoric axonal polyneuropathy. To rule out underlying malignancy, we performed integrated [18F]-fluorodeoxyglucose–positron-emission tomography/CT (FDG-PET/CT), showing an intense 18F-FDG-uptake in the cauda equina, stretching out along the left nerve root on levels L3 and L4 (Fig 1). MR imaging of the lumbar spine confirmed thickening and contrast enhancement of the nerve roots of the cauda equina, more pronounced on the left side (Fig 2). Subsequent imaging of the brain, chest, and abdomen did not demonstrate any other lesions. A repeat CSF analysis with flow cytometric immunophenotyping confirmed the presence of B-cell lymphoma, which was treated with local radiation therapy (40 Gy). Follow-up FDG-PET/CT no longer demonstrated the hypermetabolic lesion in the spinal canal. Unfortunately, a new lesion was seen in the liver, considered a metastasis on the basis of imaging results, which responded well to chemotherapy (cyclophosphamide, rituximab, and prednisone). Vincristine was omitted due to the already prominent polyneuropathy. The neurologic condition of the patient remained stable.

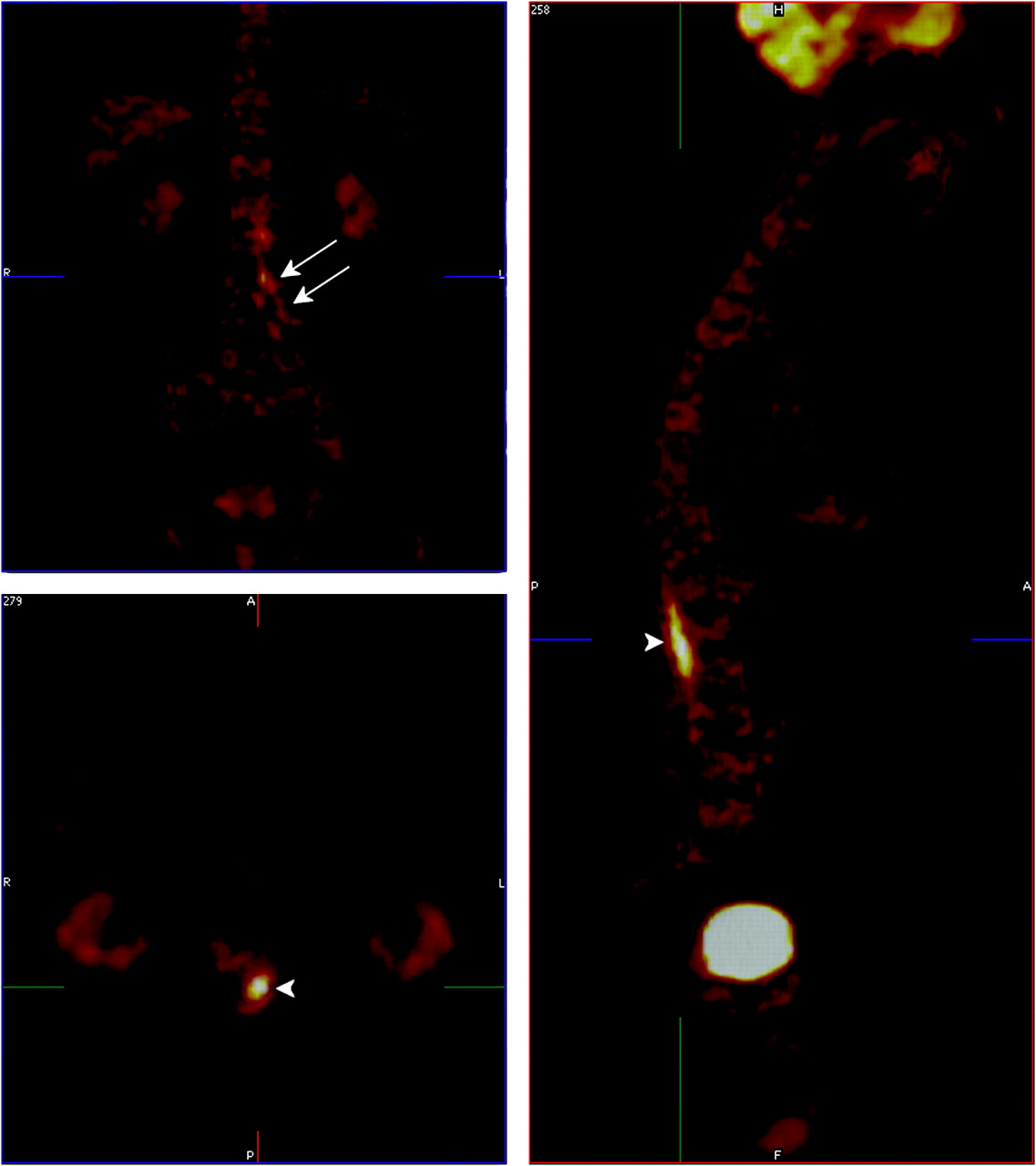
Integrated [18F]-fluorodeoxyglucose (FDG)–PET/CT scan shows an intense FDG uptake in the cauda equina (arrowhead) and nerve roots L3 and L4 on the left side (arrows).

Gadolinium-enhanced T1-weighted images obtained in the sagittal plane with fat-suppression (FS) (A) and in the coronal plane without FS (B and C) show enhancement of the nerve roots of the cauda equina (A and B) and of the L3 and L4 dorsal root ganglia (arrows, C), the left more pronounced than the right.
Lymphomas in the CNS can occur in 3 settings. Most commonly, involvement of the CNS is a late manifestation of advanced lymphoma. A PCNSL is an unusual manifestation of extranodal non-Hodgkin lymphoma, usually consisting of a diffuse lymphomatous infiltration affecting the brain, leptomeninges, eyes, and, rarely, the spinal cord. Although considered a stage IE lymphoma, PCNSL is usually associated with a worse prognosis compared with other localized extranodal lymphomas with similar histologic characteristics. Rarely, a PCNSL disseminates outside the CNS as seen in our patient.1
Diagnosis of a PCNSL is often difficult. The presence of malignant lymphocytes distinguish it from infectious diseases, paraneoplastic or inflammatory neuropathies, and complications of medical interventions. The first objective of diagnostic work-up is to obtain tissue for pathologic diagnosis and immunophenotyping; and second, to evaluate the extent of the disease. Although a biopsy remains indispensable for providing tissue samples, a blind biopsy can be inconsequential because malignant infiltration in neurolymphomatosis affecting a peripheral nerve can be patchy, possibly resulting in sampling error.2 Currently, FDG-PET is increasingly being used for staging, restaging, and response assessment of lymphomas.3 Its role in the evaluation of PCNSL has not been established yet but seems promising.4
Our case highlights the diagnostic approach when evaluating a patient with a subacute sensorimotor loss. Diagnosis of PCNSL should be kept in mind. Although FDG-PET is currently mainly used for staging or restaging and response assessment of systemic lymphomas, our case illustrates the potential role in the diagnostic work-up of PCNSL.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.