
Abstract
BACKGROUND AND PURPOSE: Fenestrations of intracranial arteries are variants resulting from incomplete fusion of primitive vessels. An association with aneurysms is suggested in many studies. On conventional angiography, fenestrations are rarely visible. 3D rotational angiography (3DRA) provides improved visualization of cerebral vessels from any desired angle. We used 3DRA to assess the frequency and location of fenestrations of intracranial arteries and a possible relationship with aneurysms.
MATERIALS AND METHODS: In 208 patients with suspected intracranial aneurysms, 3DRA of 1, 2, or 3 cerebral vessels (in 143, 16, and 49 patients) was reviewed for the presence and location of fenestrations and aneurysms. When fenestrations were present in combination with aneurysms, we noted the relationship of the locations.
RESULTS: In 59 of 208 patients, 61 fenestrations were detected (28%). Fenestrations were more frequent in the anterior than in the posterior circulation (23% versus 7%), and the most common location was the anterior communicating artery (AcomA) (43 of 61, 70%). The frequency of fenestrations in 185 patients with aneurysms was not different from the frequency in 23 patients without aneurysms. Of 220 aneurysms present in 208 patients, 10 aneurysms (4.5%) were located on a fenestration. Of 61 fenestrations, 51 (84%) were not associated with an aneurysm.
CONCLUSIONS: With 3DRA, fenestrations were found in 28% of patients. In our study, fenestrations occurred more often in the anterior than in the posterior circulation, and the most common location was the AcomA. A definite relationship between fenestrations and aneurysms cannot be concluded from our data.
Fenestrations of intracranial arteries are segmental duplications of the lumen into 2 distinct endothelium-lined channels, which may or may not share their adventitial layer.1 They can range from a small focus of divided tissue to long-segment duplication. Fenestrations are the result of partial failure of fusion of paired primitive embryologic vessels or incomplete obliteration of different anastomosis in a primitive vascular network.1,2 The association of fenestrations with aneurysms has been suggested in many small case series, though the exact relationship is not well defined. Surgical and anatomic studies indicate that fenestrations of intracranial arteries occur commonly, especially in the anterior communicating artery (AcomA) complex.3–6 Demonstration of fenestrations on conventional angiography is exceptional. Most fenestrations are only visible from 1 specific viewing angle, which is likely not present in the limited available projections of conventional angiography.1,7 Because with 3D imaging any desired viewing angle is on hand, the detection rate of fenestrations has improved.8–12 Few data are available on the frequency and distribution of locations of fenestrations. In this study, we assessed the frequency, location, and relationship with aneurysms of fenestrations of intracranial arteries by using 3D rotational angiography (3DRA) performed in patients with suspected intracranial aneurysms.
Materials and Methods
3DRA
In our practice, in all patients with suspected intracranial aneurysms in whom treatment is being considered, an intra-arterial digital subtraction angiography is performed of all cerebral vessels. When an aneurysm is apparent or suspected, additional 3DRA is performed of the vessel harboring the aneurysm to evaluate its presence and anatomy and to determine the type of treatment (coiling, surgery, or parent vessel occlusion). In patients with aneurysms allocated to coiling, 3DRA is repeated immediately before coiling with the patient under general anesthesia, to find out the best working projection.
Angiographic imaging was performed on a biplane neuroangiographic unit (Integris BN 3000 Neuro; Philips Medical Systems, Best, the Netherlands). 3DRA was performed with an 8-second 180° rotational run with acquisition of 200 images and with injection of 3–4 mL of contrast material per second in the internal carotid or vertebral artery. On a dedicated workstation, 3D reconstructions were made in a maximal matrix of 512 × 512 × 512.3
Patients
For the purpose of this retrospective study, we included patients who had undergone 3DRA and who had the raw 3DRA dataset available for review on a hard disk or a compact disk. Raw datasets were required to make high-resolution reconstructions on the workstation with new sophisticated software to evaluate the presence of fenestrations. Patients were thus not consecutive.
We included 208 3DRA datasets that were made between June 2004 and October 2008. The following patient and imaging characteristics were recorded in a data base: examination date, patient name and sex, date of birth, presence and location of aneurysms visible on the 3DRA dataset, presence and location of fenestrations, and number of vessels with rotational runs.
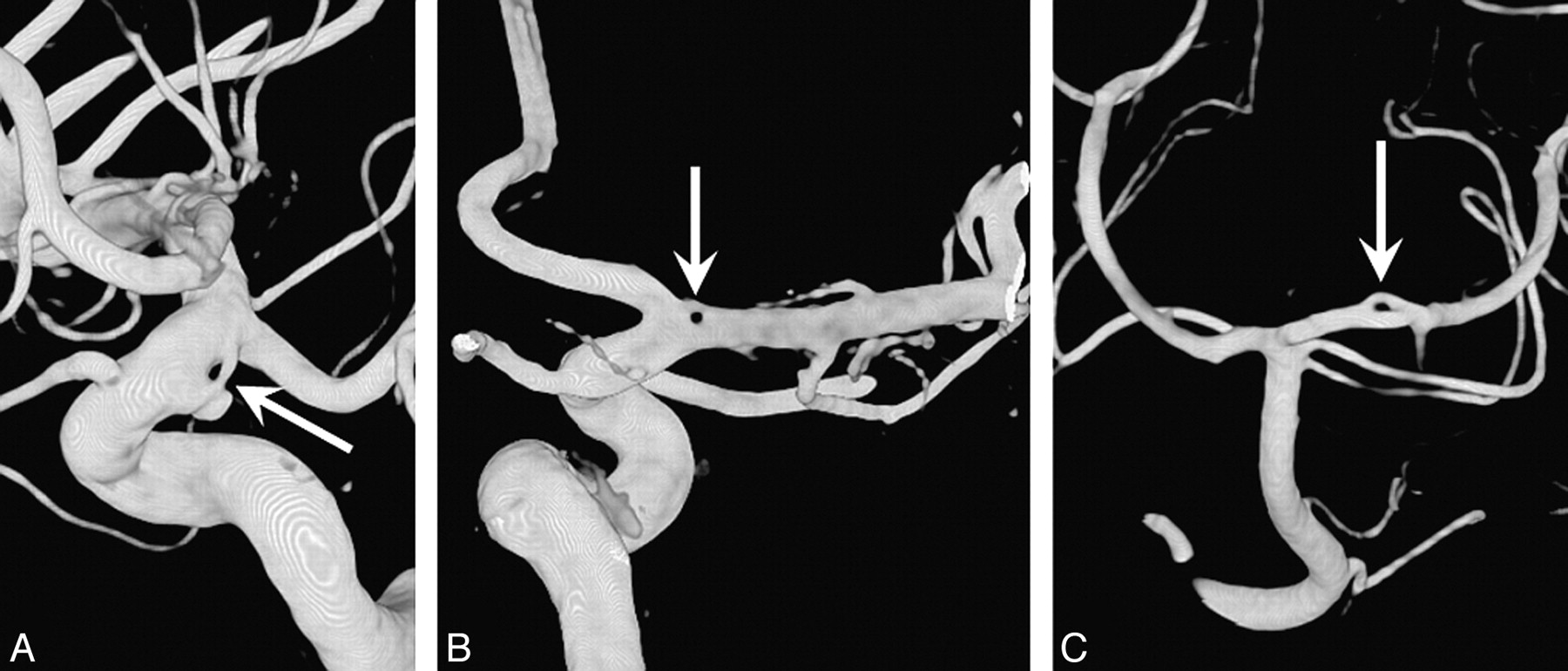
In patients with both aneurysms and fenestrations, we classified the relation of the location of the fenestration with the location of the aneurysms as remote from the fenestration, adjacent but unrelated to the fenestration, or on the fenestration itself (Fig 1). In addition, we assessed whether detected fenestrations were visible in retrospect on standard projections of 2D angiographic images.

Classification of the relation of the location of the fenestration with the location of the aneurysm. A, Aneurysm is located on the fenestration in a patient with a vertebrobasilar junction aneurysm and a proximal basilar fenestration. B, Aneurysm is located adjacent to (but not on) a fenestration in a patient with an AcomA aneurysm and a fenestration of the AcomA. C, Aneurysm is located remote from a fenestration in a patient with a basilar tip aneurysm and a proximal basilar fenestration.
Data Analysis
We compared sex distribution in patients with and without fenestrations. In patients with and without intracranial aneurysms, we compared the proportion of patients with a fenestration with those without a fenestration. In patients with fenestrations, we compared the proportion of fenestrations in the anterior circulation with the proportion of fenestrations in the posterior circulation. For comparison of proportions, the χ2 test was used.
Results
Patients
Of 208 patients with re-evaluated 3DRA datasets, 71 (34%) were men and 137 (66%) were women, with a mean age of 52.8 years (range, 14–84 years). Of 208 patients, 49 had 3DRA of 3 vessels (both carotid arteries and a vertebral artery), 16 had 3DRA of 2 vessels (14 patients with both carotid arteries and 2 patients with a carotid and a vertebral artery), and 143 patients had 3DRA of 1 vessel (carotid artery in 122 patients and vertebral artery in 21 patients). Altogether, 248 carotid arteries and 72 vertebral arteries were imaged with 3DRA.
In 23 patients, no aneurysm was detected. The remaining 185 patients had 218 aneurysms with the following locations: AcomA, 62 (28%); middle cerebral artery, 49 (22%); posterior communicating artery, 40 (18%); basilar artery, 13 (6%); cavernous sinus, 11 (5%); carotid tip, 11 (5%); anterior choroidal artery, 9 (4%); ophthalmic artery, 8 (4%); posterior inferior cerebellar artery, 6 (3%); superior cerebellar artery, 4 (2%); vertebral artery, 3 (1%); P1 segment of the posterior cerebral artery, 1 (1%); and anterior inferior cerebellar artery, 1 (1%).
Fenestrations
Results are summarized in Fig 2. Sixty-one fenestrations were present in 59 of 208 patients (28%, 2 patients had 2 fenestrations) with the following locations: AcomA in 43 (70%), middle cerebral artery in 12 (20%), posterior cerebral artery in 2 (3%), carotid artery in 1 (2%), vertebral artery in 1 (2%), superior cerebellar artery in 1 (2%), and basilar artery in 1 (2%). Of 59 patients with fenestrations, 22 (37%) were men and 37 (63%) were women. Sex distribution did not differ between patients with and without fenestrations. Of 61 fenestrations, 56 were located in the anterior circulation, diagnosed on 248 carotid artery 3DRAs, (23%), and 5 were located in the posterior circulation, diagnosed on 72 vertebral artery 3DRAs (7%). This difference was significant (P = .0043).
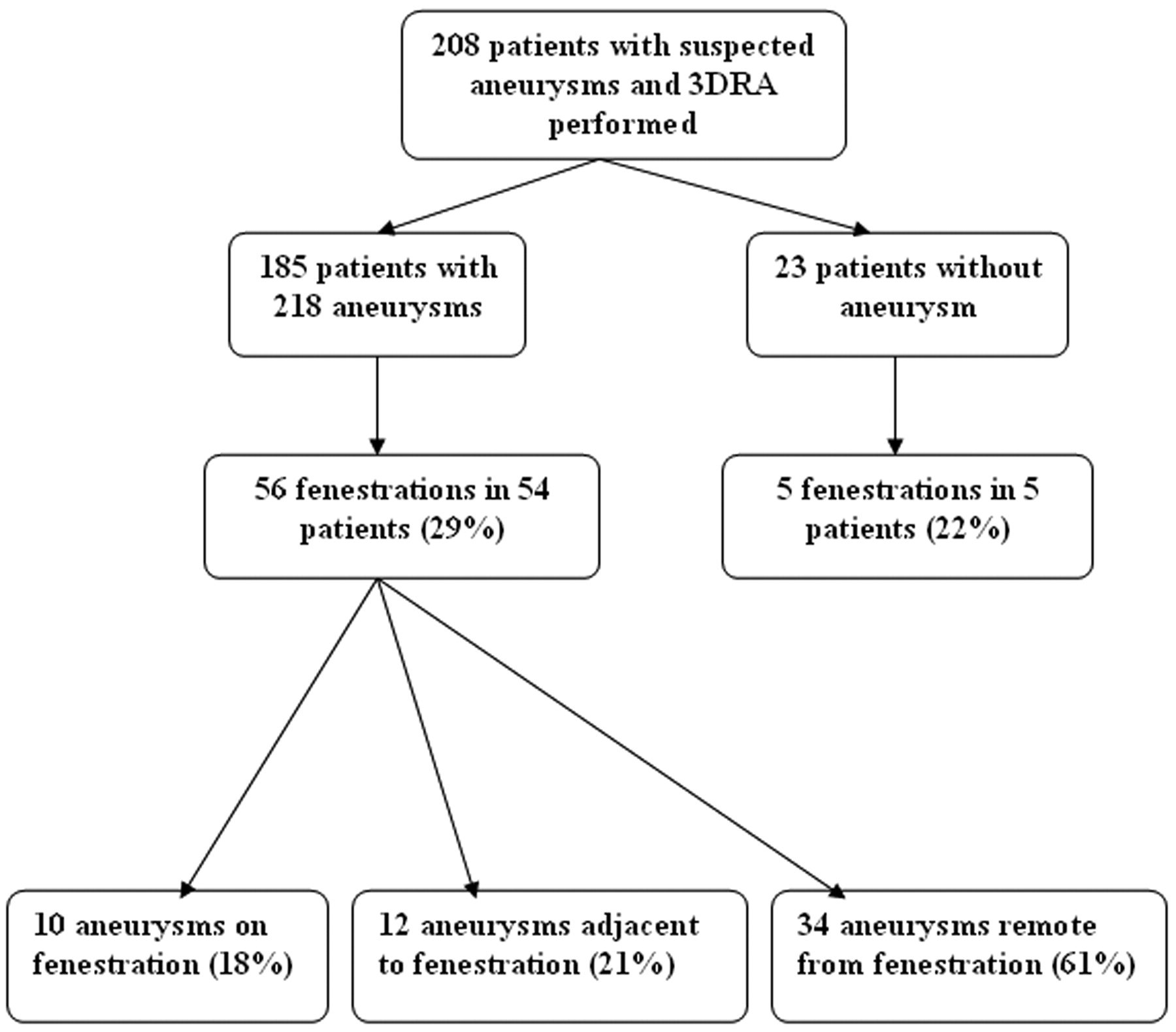
Flow chart of 208 patients with 3DRA.
Fifty-six fenestrations were present in 54 of the 185 patients (29%) with aneurysms. Five fenestrations were present in 5 of the 23 patients (22%) without aneurysms. This difference was not significant.
The anatomic relationship of the 56 fenestrations and the aneurysms in 54 patients with aneurysms was as follows: aneurysm located on the fenestration itself in 10 (18%), aneurysm adjacent to the fenestration in 12 (21%), and aneurysm remote from the fenestration in 34 (68%). In 208 patients with 218 aneurysms, 10 aneurysms (4.5%) were located on a fenestration and 210 were not. Of 61 fenestrations, 51 (84%) were not associated with an aneurysm.
Of 61 fenestrations detected on 3DRA, 10 (16%) were in retrospect visible on 2D angiographic images.
Discussion
In this study, we found that fenestrations of intracranial arteries are commonly found with 3DRA imaging. The frequency of 28% for the presence of fenestrations found in this study is an underestimation because most patients had only 1 vessel territory imaged with 3DRA. With complete 3DRA evaluation of all cerebral vessels, a frequency of approximately 40% would probably be a realistic estimate. Although fenestrations can be located anywhere in the intracranial circulation (Fig 3), they occur more often in the anterior circulation than in the posterior circulation. The most common location is the AcomA, followed by the middle cerebral artery (Fig 4). Although most fenestrations are located on or near the circle of Willis, distal cerebral arteries can also be fenestrated (Fig 4C).
Unusual locations of fenestrations of intracranial arteries. A, Fenestration of the supraclinoid internal carotid artery associated with an aneurysm. B, A very small fenestration on the proximal middle cerebral artery. C, A short-segment fenestration of the posterior cerebral artery.

Examples of middle cerebral artery fenestrations (arrows). A, Fenestration at the bifurcation with an associated aneurysm. B, Small fenestration at the neck of an aneurysm in a patient with 2 middle cerebral artery aneurysms. C, A 10-mm segment fenestration in a distal middle cerebral artery (M3).
The common occurrence of fenestrations of intracranial arteries, especially in the AcomA complex, is well known from anatomic and surgical studies.3–6 However, with 2D angiography, fenestrations are rarely found: In 2 studies of 5190 and 4500 cerebral angiograms, fenestrations were reported in 0.7% and 0.07%, respectively.1,7 Apparently, with 2D imaging, most fenestrations are overlooked or are invisible because of overprojecting vessels, preferential flow in 1 limb, or location remote from the region of interest. Many fenestrations are only visible from specific viewing angles that are usually not available on 2D imaging. Also in our study, just a small minority of fenestrations was, in retrospect, visible on standard 2D angiographic projections. With the advanced postprocessing techniques of 3DRA, cerebral vessels can be evaluated from any desired angle, and complex vascular anatomy can be unraveled effectively, allowing detection of many vessel fenestrations.
The advantage of 3D imaging in the detection of fenestrations has recently also been demonstrated in a study using CT angiography (CTA).8 In this study, fenestrations were reported in 11% of patients. The lower reported frequency of intracranial fenestrations with CTA compared with 3DRA (despite complete imaging of the brain vasculature with CTA) reflects the lower resolution of CTA combined with less-sophisticated postprocessing software. Few data are available on the detection of fenestrations with MR angiography (MRA), but the frequency seems lower as reported with both 3DRA and CTA.10–12
The association of aneurysms with fenestrations has been extensively documented, though the reason for this relationship is not well understood: Vessel wall microstructure at fenestrations is not different from that of normal cerebral vessels. At branching points, medial defects are equally as common in fenestrations as in normal vessel branching points. Aneurysms associated with fenestrations are classically thought to arise at the proximal end of a fenestration due to a combination of a medial defect and hemodynamic stresses, similar to aneurysm formation on the circle of Willis.13 In our study, the frequency of fenestrations was not different in patients with or without aneurysms. Most fenestrations were not associated with an aneurysm on the fenestration itself, and most aneurysms were not located on a fenestration. Our patient group was selected on the suspicion or presence of intracranial aneurysms. These criteria resulted in a maximal bias toward patients with aneurysms and to an overrepresentation of aneurysms in respect to fenestrations. Therefore, a definite relationship between fenestrations and aneurysms cannot be concluded from our data. Also in a recent CTA study,8 fenestrations were found to be equally common in patients with and without aneurysms and an association of fenestrations and aneurysms could not be established either.
On the other hand, a probable relation of aneurysms with fenestrations has been suggested for vertebral junction aneurysms because most of these rare aneurysms are associated with a proximal basilar fenestration.14–16 Also, some unusual locations of fenestrations in combination with aneurysms in our patient group might suggest a relationship (Figs 3A and 4A, -B). Although fenestrations might not be related to aneurysms in general, fenestrations on specific locations could, nevertheless, be associated with aneurysms. Without the availability of robust data on the frequency and location of fenestrations in the general population as a control, no definite relationship between fenestrations and aneurysms can be established. Perhaps, specific aneurysms (for example vertebral junction aneurysms) might be associated with a fenestration at that site.
Presently available data indicate that the detection rate of fenestrations with 3DRA is higher than that with CTA or MRA.
Conclusions
With 3DRA, fenestrations were found in 28% of patients. Fenestrations occur more often in the anterior circulation than in the posterior circulation, and the most common location is the AcomA. A definite relationship between fenestrations and aneurysms cannot be concluded from our data.
References
- Received December 11, 2008.
- Accepted after revision January 24, 2009.
- American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}