
Wegener granulomatosis (WG) is a rare multisystem inflammatory disorder characterized by necrotizing granulomas in the respiratory tract with or without focal necrotizing glomerulonephritis and a systemic vasculitis. Meningeal involvement, which may be diffuse or focal, is rarely represented in 4% to 11% of cases.1 We present a patient with WG having meningeal lesions in an unusual location (intraventricular) with consecutive cranial MR imaging scans.
A 33-year-old woman who was diagnosed earlier with WG and was undergoing treatment for approximately 2 months began to experience some neurologic symptoms. Contrast-enhanced MR imaging scans revealed 2 nodular enhancing extra-axial lesions on the posterior wall of the fourth ventricle, which appeared to be slightly dilated. The diameter of the largest lesion was 13 mm; in addition, there was linear meningeal enhancement close to the lesions (Fig. 1). After 20 days of steroid treatment, control MR imaging examination demonstrated regression in both nodular-enhancing lesions; the largest was 10 mm in diameter (Fig 2).

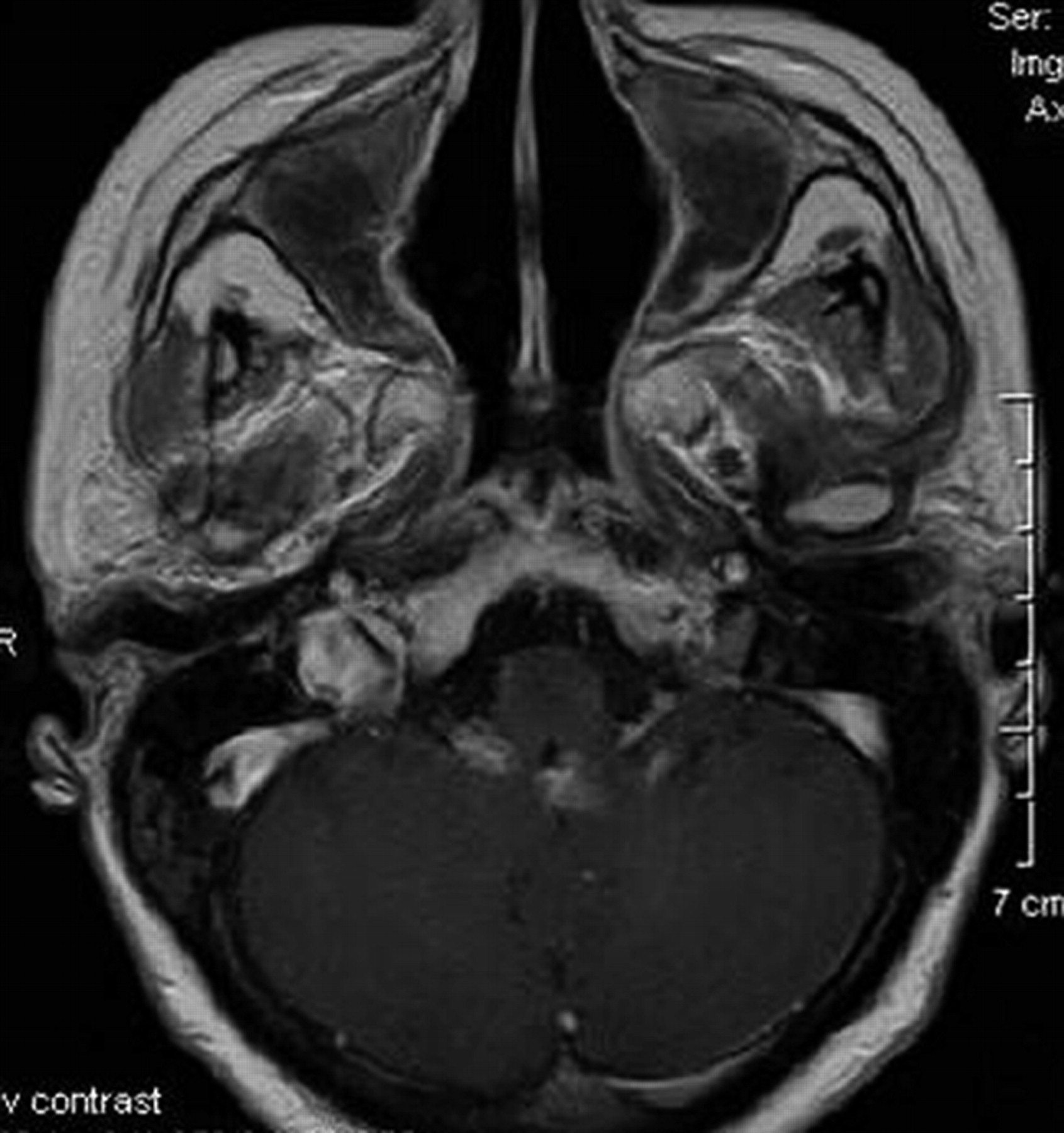
Axial T1-weighted contrast-enhanced MR image reveals 2 nodular-enhancing extra-axial lesions on the posterior wall of the fourth ventricle, which appears to be slightly dilated. The diameter of the largest lesion is 13 mm; in addition, there is linear meningeal enhancement close to the lesions.

Control MR imaging examination, which was performed after 20 days of treatment, demonstrates regression in both nodular-enhancing lesions (the largest was 10 mm in diameter) in an axial T1-weighted contrast-enhanced sequence.
Three major mechanisms causing central nervous system disease (CNS) in WG have been implicated: contiguous invasion of the granuloma from extracranial sites, CNS vasculitis, and remote intracranial granuloma. Meningeal involvement, which usually presents with diffuse or focal forms of dural thickening and enhancement, was previously reported in a small number (< 100) of cases in the literature.2 In the case of our patient, the meningeal lesions were located at the posterior wall of the fourth ventricle and the adjacent parenchyma. Therefore, it is predicated that these lesions did not derive from the dura, which is known to be the first affected meningeal layer throughout the contiguous invasion process. Taking all of these findings into consideration, we determined that the lesions in our patient may have developed secondary to leptomeningeal vasculitis. Leptomeningeal angiitis or isolated angiitis of the CNS is a rare entity, and, to our knowledge, only small case series have been reported.3 The primary cause of this entity, which is also termed primary angiitis, is unknown; however, the secondary form is known to appear as part of a systemic autoimmune disease.
In conclusion, the focal nodular type of meningeal involvement in WG may appear on the ventricle walls in association with parenchymal changes. The leptomeningeal vasculitic process seems to be the most probable mechanism of intraventricular secondary or granulomatous leptomeningeal angiitis vs meningeal involvement. We believe that an MR imaging survey of our patient will contribute to the limited imaging literature available on WG with meningeal involvement. On the other hand, it must be maintained that, as in the case of our patient, nodular-enhancing regions after administration of contrast material may mimic a brain tumor or primary lymphoma on neuroimaging.4
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.