
Abstract
BACKGROUND AND PURPOSE: Prediction of functional outcome immediately after stroke onset can guide optimal management. Most prognostic grading scales to date, however, have been based on established global metrics such as total NIHSS score, admission infarct volume, or intracranial occlusion on CTA. Our purpose was to construct a more focused, location-weighted multivariate model for the prediction of early aphasia improvement, based not only on traditional clinical and imaging parameters, but also on atlas-based structure/function correlation specific to the clinical deficit, using CT perfusion imaging.
MATERIALS AND METHODS: Fifty-eight consecutive patients with aphasia due to first-time ischemic stroke of the left hemisphere were included. Language function was assessed on the basis of the patients admission and discharge NIHSS scores and clinical records. All patients had brain CTP and CTA within 9 hours of symptom onset. For image analysis, all CTPs were automatically coregistered to MNI-152 brain space and parcellated into mirrored cortical and subcortical regions. Multiple logistic regression analysis was used to find independent imaging and clinical predictors of language recovery.
RESULTS: By the time of discharge, 21 (36%) patients demonstrated improvement of language. Independent factors predicting improvement in language included rCBF of the angular gyrus GM (BA 39) and the lower third of the insular ribbon, proximal cerebral artery occlusion on admission CTA, and aphasia score on the admission NIHSS examination. Using these 4 variables, we developed a multivariate logistic regression model that could estimate the probability of early improvement in aphasia and predict functional outcome with 91% accuracy.
CONCLUSIONS: An imaging-based location-weighted multivariate model was developed to predict early language improvement of patients with aphasia by using admission data collected within 9 hours of stroke onset. This pilot model should be validated in a larger, prospective study; however, the semiautomated atlas-based analysis of brain CTP, along with the statistical approach, could be generalized for prediction of other outcome measures in patients with stroke.
Abbreviations
- AIF
- arterial input function
- AUC
- area under the curve
- B
- the constant coefficient of the regression equation
- BA
- Brodmann area
- BASIS
- Boston Acute Stroke Imaging Scale
- CBF
- cerebral blood flow
- CBV
- cerebral blood volume
- CI
- confidence interval
- CTA
- CT angiography
- CTP
- CT perfusion
- DWI
- diffusion-weighted imaging
- EXP(B)
- exponentiation of the B coefficient
- FLIRT
- Functional Linear Image Registration Tool
- FSL
- Functional Software Library
- FN
- false-negative
- FP
- false-positive
- GM
- gray matter
- IA
- intra-arterial
- ICA
- internal carotid artery
- IV
- intravenous
- JHU
- Johns Hopkins University
- MCA
- middle cerebral artery
- MNI
- Montreal Neurological Institute
- MTT
- mean transit time
- NIHSS
- National Institutes of Health Stroke Scale
- rCBF
- relative cerebral blood flow
- rCBV
- relative cerebral blood volume
- rMTT
- relative mean transit time
- ROC
- receiver operating characteristic
Aphasia can be one of the most devastating consequences of acute stroke, present in 16%–37% of patients. Those with aphasia have poor long-term functional outcome,1 reduced probability of returning to work,2 and an increased mortality rate,3 compared with patients with stroke without aphasia.
The importance of predicting language recovery early in the course of stroke is highlighted by recent reports showing that brain reorganization occurs earlier than previously thought and that early targeted poststroke rehabilitation therapy significantly improves outcome.4 Thus, identifying patients with aphasia for early intervention could be valuable in designing an effective treatment program, including interventions such as acute thrombolytic therapy, neuroprotective agents, and acute speech therapy. Few studies, however, have provided clinicians with practical information for predicting the extent to which a patient may recover communicative abilities.
Age, aphasia type, and infarct size have been associated with long-term improvement of aphasia.5 However, early improvement of stroke symptoms is mostly dependent on reperfusion of distressed but still viable brain tissue (penumbra). The decrease in CBF (hypoperfusion) during stroke may result in cessation of neuronal activity without immediate cell death in areas surrounding the infarct core.6 Depending on perfusion hemodynamics, neurons in these areas may ultimately die, remain hypoperfused, or reperfuse with restoration of normal neuronal function. Prior studies have revealed a correlation between different types of aphasic syndromes and the location of hypoperfused brain.7,8 Indeed, Hillis et al9 reported that MR perfusion/diffusion mismatch in BA 37 was associated with recovery of “naming” function in patients with stroke.
CTP imaging of the brain is commonly used in clinical practice to assess cerebral hemodynamics in patients with acute stroke, due in part to its practicality in terms of availability, speed, and cost. In the present study, we sought to develop a location-weighted multivariate model to predict early improvement of aphasia in patients with acute stroke based on admission clinical and imaging findings, by using a semiautomated method of CTP image analysis. Short-term recovery was evaluated in our study because it is more closely related to early reperfusion brain-tissue salvage compared with long-term clinical outcome that is largely affected by rehabilitation therapy, structural reorganization, and recruitment of unrelated brain areas.
Methods and Materials
Patients
We retrospectively reviewed our prospectively collected data base to find patients with acute ischemic stroke admitted between December 2006 and April 2008 in our center. A total of 119 consecutive patients were identified; among these, 58 patients were included on the basis of the following criteria: unilateral left-hemispheric stroke; any signs of aphasia associated with stroke onset according to medical records; CTP within 9 hours of symptom onset; no evidence of chronic infarction; and technically usable CTP images. This study received approval from our institutional review board and was compliant with the Health Insurance Portability and Accountability Act.
Aphasia symptoms of each patient were extracted from the medical records on the basis of physical examination notes, including component NIHSS examination scores recorded at admission and discharge. Patients were categorized into 2 groups: those with improvement of language function by the time of discharge and those with no clinically detectable improvement. Improvement of language function was considered when there was a decrease in the NIHSS aphasia score or an unequivocal statement in the medical record confirming the improvement of language. Patients with equivocal or inadequate data were excluded.
Patients were treated with standard therapies, including IV thrombolysis or IA therapy, as clinically indicated.
Image Acquisition
All CT was performed on a 64-detector row volume CT helical scanner (LightSpeed; GE Healthcare, Milwaukee, Wisconsin). In all patients, unenhanced CT scanning was followed immediately on the same scanner by CTA and CTP imaging. CTA was performed at 120 kV, 200 mA, 1.25-mm section thickness, helical scanning mode, with IV administration of 65–75 mL of nonionic iodine contrast material (iopamidol, Isovue Multipack 370; Bracco Diagnostics, Princeton, New Jersey) at 4 mL per second. For each of the 2 anterior circulation CTP slabs studied (1 with lowest section at the level of the circle of Willis and 1 immediately superior to this), a total of 40 mL of contrast material was injected by using a power injector at a flow rate of 7 mL/s. Five seconds after the start of injection, dynamic scanning was performed as a 66-second biphasic cine series by using the following parameters: 8 contiguous 5-mm-thick sections (4-cm vertical coverage per slab), 80 kV(peak), 200 mA, 1-second rotation time, 1 image per second for 40 seconds with 9 additional images 1 every third second. The total estimated effective radiation dose to the head was 11.6 mSv (unenhanced CT of the head, 2.5 mSv; CTA of the head, 2.5 mSv; and 2-slab CTP of the head, 6.7 mSv).
The acquired CTP series was transferred to an Advantage Workstation (GE Healthcare) for postprocessing of CTP maps including CBF, CBV, and MTT, by using delay-corrected deconvolution-based commercial CTP software (CT Perfusion 4; GE Healthcare); the software automatically excludes vessels on the basis of a preset threshold. The reference AIF was selected by the software in a region of interest that the user manually drew around the terminal ICA or anterior cerebral artery. Care was taken not to select the AIF anywhere distal to the site of major arterial occlusions.10
Image Analysis
All CTP maps were automatically coregistered to MNI-152 standard brain space by using 12-parameter affine linear transformations (FLIRT, Version 5.5; Oxford Centre for Functional Magnetic Resonance Imaging of the Brain, Oxford, United Kingdom).11 In most cases, the lower and upper slabs were appended to create a single 16-section CTP map. All scans were visually controlled for satisfactory coregistration, and there was no need for any further manual correction. Custom-written software (Matlab 7.8; MathWorks, Natick, Massachusetts) was used for automated image analysis. Briefly, all CTP maps were subsegmented into paired mirror cortical and subcortical areas on the basis of preset atlases implanted in FSL 4.1.2 (Oxford Centre for Functional Magnetic Resonance Imaging of the Brain). We modified the Talairach and JHU atlases supplied with the FSL package and divided the large subcortical areas into smaller subregions for more precise evaluation of different brain areas. A total of 146 pairs of regions were automatically segmented. The average region volume was 6.4 ± 2.1 mL. Then, the relative CTP values (rCBF, rCBV, and rMTT) for each brain region were calculated as the ratio of left-hemispheric (stroke-side) mean value divided by contralateral mirror-region mean value (hence, each relative CTP parameter value is defined as the following: [ischemic region CTP value]/[contralateral mirror-region CTP value]; all values reflect the mean quantitative units from the scan region of interest).
In each patient, intracranial arterial occlusion was determined on the basis of the admission CTA study as recorded in the prospective clinical report.12 Patients were identified as having proximal cerebral artery occlusion in case of either distal/terminal ICA or proximal (M1 or M2) MCA cutoff. The presence of proximal cerebral artery occlusion was a binary variable assigned as 1 in the presence of occlusion and 0 in the absence of occlusion.
Statistical Analysis
For statistical analysis, we categorized patients into 2 groups: those with and those without improvement of aphasia at discharge. First, we compared all clinical and imaging variables between the 2 groups in a univariate analysis by using the Student t test, the Wilcoxon rank sum (Mann-Whitney) test, or the χ2 test, as appropriate.
To determine which brain areas and CTP parameters were best predictive of language improvement, we generated ROC curves to identify those CTP parameters that could predict improvement of speech most accurately on the basis of the AUC (a larger AUC value suggests that the corresponding variable can predict improvement of speech more accurately). For each brain region (146 pairs totally), we compared rCBF, rCBV, and rMTT values between study groups separately.
Next, a multiple logistic regression model by using stepwise selection was constructed to determine which of the CTP regions were independent predictors of language improvement. Given the size of our study cohort relative to the potential number of variables in our model, only those variables that had the highest possibility for independent prediction of outcome in our logistic regression were included. Specifically, only those CTP parameters that could distinguish between the 2 study groups with ROC AUC > 0.75 were included in the initial calculation of stepwise regression. If for a particular brain region, 2 CTP parameters (eg, both rCBF and rMTT) had ROC AUC > 0.75, only the one with the higher AUC was included in the stepwise logistic regression calculation. Moreover, due to incomplete coverage of the more inferior brain regions for some patients (particularly in the inferior MCA distribution), 5 regions that were not scanned in 15 cases were excluded from the model; of note, Broca and Wernicke areas were not among the regions excluded.
An additional stepwise multiple logistic regression model was constructed to determine the independent clinical and CTA variables (Table 1) predictive of language improvement. Finally, by using the imaging and clinical variables determined to be independent predictors of language improvement in the above stepwise models, forced-entry multiple logistic regression was also performed to develop overall predictive models for language improvement, with ROC AUC analysis used to determine the accuracy of these models.
Comparison of clinical/CTA characteristics between patients with and without improvement of aphasia (univariate analysis)
The probability of improvement for each patient was computed by entering the values for the independent predictors of the final logistic regression equation into the standard statistical formula
All statistical analyses were performed by using STATA 10 (StataCorp, College Station, Texas) and the Statistical Package for the Social Sciences, Version 17.0 (SPSS, Chicago, Illinois); all values are reported as either mean ± standard error of mean or median (range).
Results
A total of 58 patients (26 men, 32 women) with aphasia due to first-time left-hemisphere ischemic stroke were included in our study (Fig 1). The mean age was 74 ± 1.8 years, and the median NIHSS score at the time of admission was 13 (range, 2–28). Only 16 patients received IV thrombolytic therapy within 3 hours of stroke onset; of these, 4 also underwent thrombectomy at 8–9 hours after stroke onset.

Of 119 patients with acute ischemic stroke who underwent CTP at our hospital between December 2006 and April 2008, 58 were included in this study.
By discharge (median, 6 days; range, 3–22 days), 21 (36%) patients had clinically detectable improvement of language function. In Table 1, admission clinical characteristics, CTA findings, and time intervals are compared between patients with and without improvement of aphasia. Those with improvement had significantly lower total NIHSS scores and NIHSS aphasia scores at admission, compared with those without improvement. Moreover, patients with aphasia who had proximal cerebral artery occlusion at admission were significantly less likely to experience any improvement of language function by discharge (odds ratio for language improvement, 0.117; 95% CI, 0.034–0.397).
There was no significant difference in the percentage of patients with improvement for the subgroups who received IV thrombolysis or thrombectomy. There was only 1 patient (of 4) who had complete recanalization of occlusion following thrombectomy (Table 1).
Of note, most CTP scans were acquired following IV thrombolytic treatment (11/16, 69%). The ictus-to-treatment, treatment-to-scan, and ictus-to-scanning-time intervals were not significantly different between the 2 study groups (Table 1). All thrombectomies were performed approximately 8–9 hours after stroke onset in patients who had already received IV therapy.
The only independent predictors of language improvement based on the regional CTP logistic regression model were rCBF values in the lower third of the sublobar insular ribbon and angular gyrus GM, BA 39 (Fig 2).

Upper row: orthogonal sections of the lower third of the sublobar insular ribbon. Middle row: orthogonal sections passing through the angular gyrus GM of BA 39. The mean relative rCBF values of these 2 regions were the only CTP parameters that were independent predictors of early aphasia improvement. Lower row: a 3D standard MNI-152 brain space reflecting the main cortical BAs directly involved in language function (labeled by corresponding number), as well as the lower third subinsular ribbon and angular gyrus GM, as noted above.
In the subsequent clinical/CTA-based stepwise multiple logistic regression, the only independent predictors of language improvement, among all variables listed in Table 1, were the admission NIHSS aphasia score and the presence or absence of proximal large-vessel occlusion on admission CTA. (Because there was a high level of colinearity [R > 0.5] between the overall admission total NIHSS score and the component aphasia score of the NIHSS examination, only the specific aphasia score was included in this model.)
Next, an imaging-based forced-entry multiple logistic regression model was constructed by using only the admission CTA and CTP variables that could predict language improvement independently on the basis of the above stepwise models (Table 2). ROC curve analysis of the resulting regression equation predicted early language improvement with 85% sensitivity, 85% specificity, and 85% accuracy (AUC = 0.89). There were 5 false-positive cases (positive predictive value, 76%) and 5 false-negative cases (negative predictive value, 87%).
Details of the forced-entry multiple logistic regression model derived only from the admission CTP/CTA independent predictors of language improvement
Finally, we constructed a forced-entry multiple logistic regression model that included all 4 of the imaging and clinical variables that were independent predictors of language improvement. Table 3 shows the details of this final logistic regression equation, resulting in an arbitrary value. On the basis of the ROC curve analysis, a cut-point of >0 for this value results in a 90% sensitivity, 91% specificity, and 91% accuracy for prediction of language improvement. This full model, which included the clinical examination data, showed a trend toward improved prediction versus the imaging model only (P = .103). The boxplot graph confirms the significance of this model for predicting language improvement (Fig 3). With the final model, there were only 3 false-negative cases (positive predictive value, 86%) and 3 false-positive cases (negative predictive value, 92%). One of the 3 false-negative cases was a patient who underwent successful thrombectomy almost 9 hours after stroke onset. This patient received IV thrombolytic 30 minutes after stroke onset and was scanned 47 minutes after stroke onset. There was 1 false-positive case who had also received IV thrombolytic therapy; the remaining 4 false-positive and false-negative cases had received no thrombolytic therapy.
Details of the forced-entry multiple logistic regression model derived from both the admission CTP/CTA imaging and the clinically independent predictors of language improvement
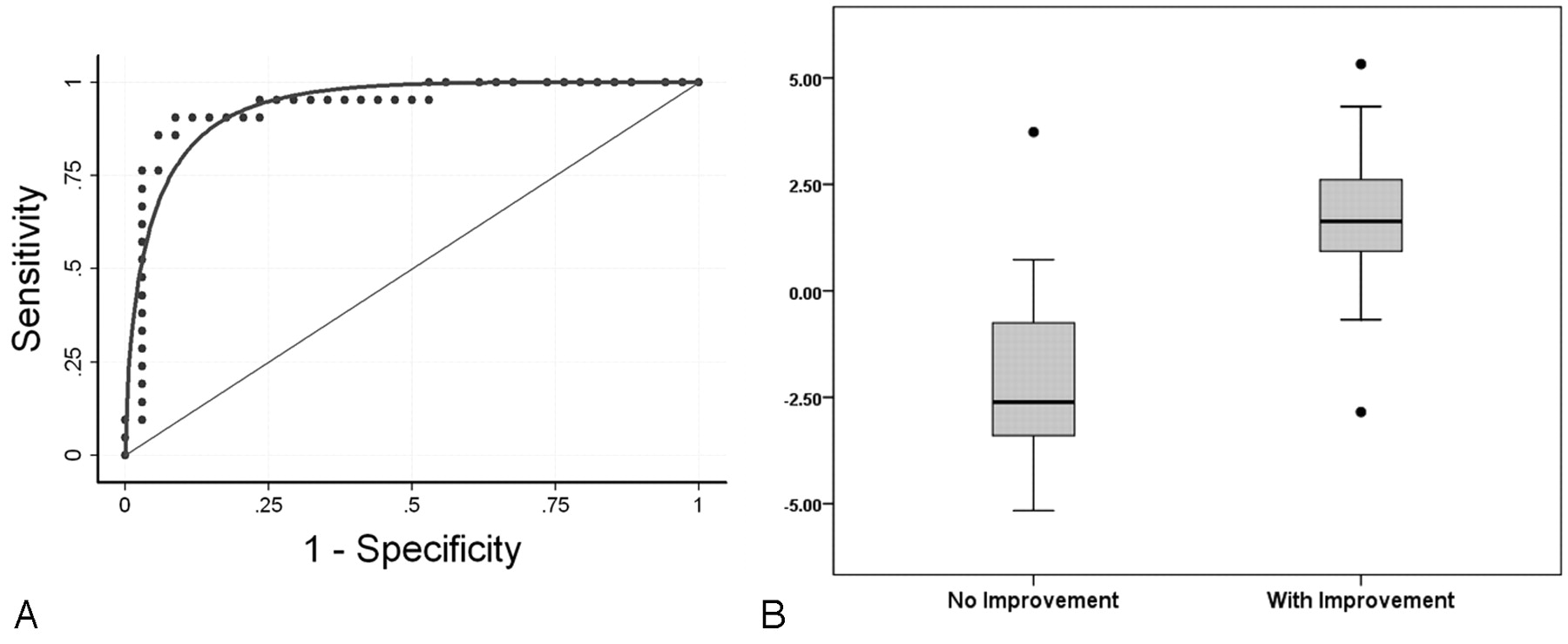
A, The ROC curve for the forced-entry multiple logistic regression model derived from the admission CTP/CTA imaging and the clinically independent predictors of language improvement (Table 3). B, Boxplot graph shows how this model can distinguish between those patients with improvement of language function and those without; the y-axis represents the values of the regression equation (Table 3). Patients with aphasic with positive regression scores (>0) have a >50% probability of language improvement by discharge.
On the basis of the coefficients of this regression equation, we have formulated a pilot practical 8-point “aphasia improvement score” by using the 4 variables listed above to stratify patients into 5 potential improvement groups, ranging from “excellent” to “dismal” (Tables 4 and 5). Probability values were estimated only for patients in the study population with no extrapolation to other possible cases; the scoring system was further modified to best classify patients in our cohort.
Calculation of the 8-point aphasia improvement scorea
Predictive value of the aphasia improvement score
Discussion
The ability to treat patients with acute stroke with thrombolytics has increased the need for rapid detection and evaluation of this condition. Increasingly, newer neuroprotective agents and recovery strategies are targeting these patients, raising demand for diagnostic and biomarker variables to assist patient selection. Stroke imaging can contribute significantly by identifying patients likely to recover during the early subacute phase due to restoration of arterial blood flow, either spontaneously or following thrombolytic treatment. It is important to not only weigh the risks versus benefits of aggressive treatment to restore cerebral perfusion but also to support decisions regarding subsequent management.4 In this study, we developed a pilot model to predict early improvement of aphasia based on admission imaging and clinical data.
This model predicted clinical outcome with high accuracy (91%) on the basis of data collected within 9 hours of stroke onset. In summary, patients with aphasia with normal, near-normal, or hyperemic rCBF of the subinsular ribbon and angular gyrus and without proximal cerebral artery occlusion at admission were most likely to show improvement of language function by hospital discharge (Table 3). Moreover, by using only the 4 independent outcome predictors of our final model—specifically, admission NIHSS aphasia score, presence or absence of a proximal large-vessel intracranial occlusion, and degree of rCBF derangement in the left subinsular ribbon and left angular gyrus—we developed a practical simple-to-apply pilot aphasia improvement score for predicting the likelihood of language improvement, which has the potential to be of value in patient triage pending validation by prospective studies. Notably, the scoring system was constructed on the basis of the regression coefficients of our cohort population, thus requiring validation in larger independent studies.
Using the logistic regression equation of the final model (Table 3), one can more precisely estimate the probability of language improvement in a given patient on the basis of the same 4 variables, as explained in the “Materials and Methods” section. The value of our model may extend beyond the first few days following stroke onset because the severity of aphasia within the first week postictus is one of the most important predictors of long-term language function, accounting for 47% of the variation in the aphasia score 1 year after stroke.13
Most interesting, the 2 brain regions we found to be independent predictors of aphasia improvement are not those most commonly associated with language function (Fig 2). However, the left BA 39 (angular gyrus) has been reported to have a role in semantic processing,14 and hypoperfusion/infarction of this region contributes to the error rate in oral naming.7 An analogous role of the insular ribbon in language function may apply. Although the brain regions identified in our study may directly contribute to language function, to some extent,7 our results only reveal a correlation between aphasia outcome and perfusion status of these regions and do not prove a direct association.
Of note, numerous abnormalities have been reported to be associated with insular infarction, including sympathetic activation,15 stroke-related myocardial damage,16 and positional vertigo.17 These findings, however, may be an epiphenomenon and simply reflect the high frequency of insular damage in large MCA territory strokes. It is also plausible that the perfusion defect in the lower insular cortex reflects edematous damage or hypoperfusion of the adjacent inferior frontal gyrus Broca area or the deep arcuate fasciculus.
Regardless, our findings suggest that ischemia of these 2 left-hemisphere regions is a strong predictor of poor outcome in patients with aphasia, albeit these cerebral areas may not directly contribute to language function. Our data suggest that mean rCBF of these 2 regions better predicts language recovery than other cortical and subcortical areas known to be more directly involved in language production; therefore, potentially reversible hypoperfusion (ie, ischemic penumbra) of these specific regions reflects the overall perfusion status of a complex left-hemispheric language neural network.
Clearly, the acute infarction volume has prognostic value; however, for optimal prediction of language outcome, it is valuable to know not only the size and degree of this ischemic penumbra but also its spatial localization.9 Because the precise definition of “penumbra” remains controversial18 and because the thresholds for distinguishing truly ischemic hypoperfused tissue from benign oligemia have not yet been validated and standardized,19–21 our approach to determine the independent predictors of language improvement has been to directly model the regional normalized perfusion parameter values with a logistic regression, rather than segmenting these regions by using arbitrary threshold values that have not yet been established. Having identified specific brain regions whose rCBF values served as independent predictors of functional improvement, we then integrated this CTP data with the admission CTA and clinical parameters to produce a more accurate optimized model.
Admission aphasia score and cerebral arterial occlusion were also independent predictors of aphasia improvement. This finding is in agreement with previous reports.13 Due to the very high colinearity between the total NIHSS score and the NIHSS aphasia score, we included only the more relevant NIHSS admission aphasia score in our model, though Pedersen et al13 found that the inclusion of an overall admission stroke-severity score, in addition to the admission aphasia quotient, incrementally improved the accuracy of their 1-year aphasia outcome prognosis.
The application of a multivariate model by using imaging variables only (Table 2) could be especially valuable in circumstances in which a clinical examination is unavailable or unreliable, such as the presence of a language barrier or in an obtunded patient. Admission CTA findings were also important in this regard. Based on the BASIS classification system,12 we categorized CTA findings into those patients with versus those without proximal large-vessel cerebral artery occlusion (intracranial ICA and M1 or M2 MCA). Patients with major stroke by BASIS classification are reported to have higher mortality rates, longer durations of hospital stay, and higher rates of discharge to rehabilitation.12 On the basis of our results, one can approximate the probability of language improvement based on the admission CTA and CTP findings alone, albeit the addition of the admission NIHSS aphasia score improves the accuracy of this prediction.
In addition to our clinical results, our methodologic approach is noteworthy in that it has the potential to be generalized to the prediction of other clinical outcomes, such as motor function. We developed an automated method for image analysis, with minimal operator-dependent bias and highly reproducible results. All CTP images were automatically coregistered to standard MNI-152 brain space by using highly robust and effective registration software (FLIRT 5.5).11 For parcellation of the brain, a preset atlas based on widely available Talairach and JHU atlases supplied with FSL freeware was used.22 Thus, our image analysis was totally operator-independent, representing a major advantage over the typical methodology for such studies, which relies on manual registration/overlay for segmentation of the brain.20 In addition, this tool can be used to create a same-language forum for comparison of results across different centers. This elimination of operator-dependent bias underscores the predictive strength of the resulting regression models.
Among patients receiving thrombolytic therapy, there was no significant difference between those with and those without language improvement. Due to the small number of cases in our cohort, we were unable to construct separate blocks for our multivariate model substratified by treatment. Moreover, many patients received IV thrombolytic therapy before CTP acquisition. An ideal model would be able to predict the probability that a particular treatment, at a given time after stroke onset, improves clinical outcome.
The major limitation of our study was that the same cohort was used for both model development and estimation of test characteristics; in an ideal situation, different samples should be used for model development and validation, to avoid bias toward an overestimation of the test characteristics. Another important limitation of our study was the lack of patient evaluation with a specialized language test battery.7,9,13 Using a specialized battery provides not only a more reliable measure of outcome but also the ability to quantitatively rate the degree of improvement.7,9 Moreover, the correlation between specific brain regions and functional outcome cannot be assessed when voxels in those regions, due to artifacts or insufficient coverage of the inferior MCA division territory, are insufficiently scanned in every patient. As noted in the “Results,” it was for this reason that we excluded some brain regions (n = 5) from our model; most important, these exclusions did not include Broca and Wernicke areas. Of note, MR perfusion or CTP with 256- and 320-multidetector CT scanners can potentially improve spatial coverage of the brain.
An additional caveat is the hypotheses relating special functional outcomes to particular regions of brain, whether one identifies areas by BAs, gyri, or groups of voxels on scans registered to spatial coordinates of an “idealized” brain image (MNI-152); even the most robust and effective methods of coregistration or normalization of brain images are imperfect. Each individual patient has a unique pattern of sulci and gyri and a variable degree of structural deformity, which may interfere with coregistration to MNI-152 young brain template. However, visual inspection of coregistered CTP images in our series confirmed adequate cortical coregistration. Moreover, exclusion of patients with previous ischemic stroke and inclusion of patients with acute ischemic stroke in our study minimized asymmetric brain abnormalities that might interfere with effective coregistration.
Conclusions
We have presented a semi-automated operator-independent and reproducible method for atlas-based analysis of brain regions on CTP images. Using this technique, we have developed a pilot logistic regression model that can predict the likelihood of early clinical improvement in patients with stroke presenting with aphasia on the basis of the admission CTP and CTA data, with a high level of accuracy (85%). The accuracy of this model increased to 91% with the addition of the admission clinical data (aphasia score on admission NIHSS examination) to the model. Although structural reorganization largely contributes to the long-term clinical outcome of patients with stroke, early brain perfusion and clinical status also play a major role in acute management—and hence long-term outcome—underscoring the potential clinical utility of this pilot model, which will need to be validated in a larger prospective cohort.
Footnotes
-
This work was supported by the Specialized Programs of Translational Research in Acute Stroke Network grant funded by the National Institutes of Health (P50 NS051343), the Agency for Healthcare Research and Quality grant AHRQ R01 HS11392, and the Massachusetts General Hospital Clinical Research Center (1 UL1 RR025758–01) Harvard Clinical and Translational Science Center, from the National Center for Research Resources.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received February 1, 2010.
- Accepted after revision March 9, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Differential Contribution of ASPECTS Regions to Clinical Outcome after Thrombectomy for Acute Ischemic Stroke
- Location-Specific ASPECTS Paradigm in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis
- Acute Ischemic Stroke Infarct Topology: Association with Lesion Volume and Severity of Symptoms at Admission and Discharge
- Imaging for Prediction of Functional Outcome and Assessment of Recovery in Ischemic Stroke
- Prediction of Aphasia Outcome Using Diffusion Tensor Tractography for Arcuate Fasciculus in Stroke
- Location-weighted CTP analysis predicts early motor improvement in stroke: A preliminary study
- Cerebral perfusion in acute stroke prognostication: Go with the flow, or know with the quo?