
Abstract
BACKGROUND AND PURPOSE: IA is a valuable adjunct during surgery for a variety of neurovascular diseases; however, there are no reported series describing IA for DAVFs. This study was undertaken to evaluate the safety and efficacy of IA for DAVFs.
MATERIALS AND METHODS: A retrospective review of DAVF surgical cases during a 20-year period was conducted, and cases with IA were evaluated. Clinical details, surgical and angiographic findings, and postoperative outcomes were reviewed. The incidence of residual fistula on IAs, the utility of the surgical procedure, and the incidence of false-negative findings on IA were also determined.
RESULTS: IA was performed in 29 patients (31 DAVFs) for DAVFs. The distribution of the fistulas was the following: transverse-sigmoid (n = 9), tentorial (n = 6), torcular (n = 3), cavernous sinus (n = 4), SSS (n = 4), foramen magnum (n = 3), and temporal-middle fossa (n = 2). Twelve patients had undergone prior embolization, while 6 patients had unsuccessful embolization procedures. Thirty-eight surgeries were performed for DAVF in 29 patients, and IA was performed in 34 surgeries. Forty-four angiographic procedures were performed in the 34 surgeries. Nine patients underwent multiple angiographies. In 11 patients (37.9%), IA revealed residual fistula after the surgeon determined that no lesion remained. This led to further exploration at the same sitting in 10 patients, while in 1 patient, further surgery was performed at a later date. False-negative findings on IA occurred in 3 patients (10.7%).
CONCLUSIONS: IA is an important adjunct in surgery for DAVF. In this series, it resulted in further surgical treatment in 37.9% of patients. However, there was a 10% false-negative rate, which justified subsequent postoperative angiography.
Abbreviations
- AVM
- arteriovenous malformation
- CCF
- carotid cavernous fistula
- DAVF
- dural arteriovenous fistula
- ECA
- external carotid artery
- IA
- intraoperative angiography
- ICA
- internal carotid artery
- LECA
- left external carotid artery
- LVA
- left vertebral artery
- NPV
- negative predictive value
- PPV
- positive predictive value
- SSS
- superior sagittal sinus
DAVF is an abnormal connection between an arterial feeder and a dural venous sinus or a leptomeningeal vein, with the nidus located within the dural leaflets. These lesions compose 10%–15% of all the intracranial vascular malformations.1 Although a large number of DAVFs are benign and do not bleed, the presence of leptomeningeal venous drainage predisposes them to hemorrhage and venous hypertension.2 Endovascular techniques from both arterial and venous accesses are used to treat a majority of DAVFs and have become the treatment of choice for most of these lesions.3–8 However, there is a small subset of patients who have DAVFs with anatomic features requiring surgical treatment.9–11 Because DAVFs do not have a compact nidus and are surgically treated by various means, including packing of the sinus, disconnection of the leptomeningeal veins, and disconnection of the dural feeders from the sinus,12–14 it is important to document complete resection of the DAVF and absence of any early draining veins intraoperatively to avoid the risk of hemorrhage postoperatively and to avoid a second surgery for the patient.
IA is an important tool for assessing the adequacy of surgical treatment of various vascular lesions of the brain, including aneurysms, AVMs, and DAVFs.15,16 Various authors have reported their experience in the use of IA in aneurysms and AVM surgery.15–24 IA can detect the residual neck of a aneurysm, other aneurysms, and unnoticed parent vessel occlusion in aneurysm surgery.15–18 It is used in AVM surgery to assess the presence of residual AVMs and early draining veins18–22; to localize small AVMs, determining whether the feeding vessel is a dedicated feeder or a vessel en passage; and during emergency surgery for AVM, for hematoma evacuation. Previous reports of IA for vascular malformations have included only a few DAVFs. To our knowledge, there is no report describing the use of IA during surgery for DAVF alone. We evaluate our experience with the utility of IA in surgery for cranial DAVFs.
Materials and Methods
A retrospective review was conducted of all patients with intracranial DAVFs treated at our institution by surgical resection between 1990 and 2010. All patients who had IA at the time of their resections were included in this study. Patient age, sex, location of the DAVF, clinical presentation, preoperative embolization, and preoperative clinical condition were documented. The operative notes and the angiographic images and report were used to record the results of the IA.
IA Procedure
Informed consent was obtained from all patients for IAs performed with the surgical procedure. After general anesthesia was induced, a right femoral sheath was introduced and was connected to a heparinized saline flush. During the positioning, the patient's head was fixed by using a radiolucent head frame to allow imaging. IA was performed after the surgeon thought that the fistula was obliterated. The vessels injected depended on the preoperative angioarchitecture of the DAVF. Hand injection of contrast was used in all the patients. The predominant angiographic finding suggesting a residual DAVF was the presence of an early draining vein. If there was a residual DAVF, the surgeon generally explored the fistula further; angiography was then repeated until early venous drainage was not seen.
Postoperative Angiography
A formal biplane postoperative angiogram was obtained in all patients in the angiography suite. In most patients, it was performed during the same hospital admission, within 1–3 days of surgery. In some patients, it was obtained after discharge for logistic reasons. Absence of an early draining vein or sinus was taken as a sign of angiographic cure of the DAVF. Residual fistulas were managed with repeat surgery, embolization, or a combination of these.
Statistical Analysis
Findings of the IA were compared with the surgical findings and postoperative angiography results. The sensitivity and specificity of IA and the positive predictive value were calculated. The relationship between the presence of residual fistula on IA and the location of the DAVF was evaluated by using a χ2 test.
Results
During the study period, 49 patients underwent surgery for cranial DAVFs. Of these, IA was performed in 29 patients, who composed the study population. IA was not performed in 20 patients for the following reasons: surgery for exposure of the sinus (n = 3), superficial temporal artery-middle cerebral artery bypass before sacrifice of the ICA for CCF (n = 2), emergency surgery for hematoma evacuation and planned partial excision (n = 3), surgeon preference (n = 8), patient undergoing surgery in the prone position (n = 3), and data not available (n = 1).
There were 17 women and 12 men, with ages ranging from 24 to 73 years (mean age, 50.8 years). These 29 patients had 31 DAVFs, with 2 patients having multiple DAVFs.
The distribution of the fistulas was the following: transverse-sigmoid (n = 9), tentorial (n = 6), torcular (n = 3), cavernous sinus (n = 4), SSS (n = 4), foramen magnum (n = 3), and temporal-middle fossa (n = 2). Presenting features were the following: hemorrhage related to the fistula (n = 13), hemorrhage not related to the fistula (n = 2), tinnitus (n = 7), nonhemorrhagic neurologic deficits (n = 3), ophthalmoplegia (n = 3), and intracranial hypertension. (n = 1). Twenty-two patients had cortical venous drainage (6 patients had venous aneurysms). Twelve patients underwent prior embolization, while 6 patients had attempted but unsuccessful embolization procedures. The Borden grades25 of the fistulas were the following: grade 1 (n = 7), grade 2 (n = 21), and grade 3 (n = 3).
IA
A total of 38 surgeries were performed for the DAVFs in 29 patients (31 DAVFs), and IA was used in 34 of those surgeries (Figs 1 and 2). It was not performed in 4 of the surgeries because of surgeon preference. A total of 44 angiographic procedures were performed in the 34 surgeries, with 9 patients undergoing multiple angiographies until fistula obliteration. IA was performed without moving patients from their surgical positioning. During their surgery, patients were positioned supine (n = 20 patients), lateral (n = 4), or three-quarter prone (n = 10). Postoperative angiography was performed in all patients to look for any residual fistula/early draining vein. In 26 patients, postoperative angiography was performed on postoperative days 1–3, while it was done after 1–2 months in 3 patients.
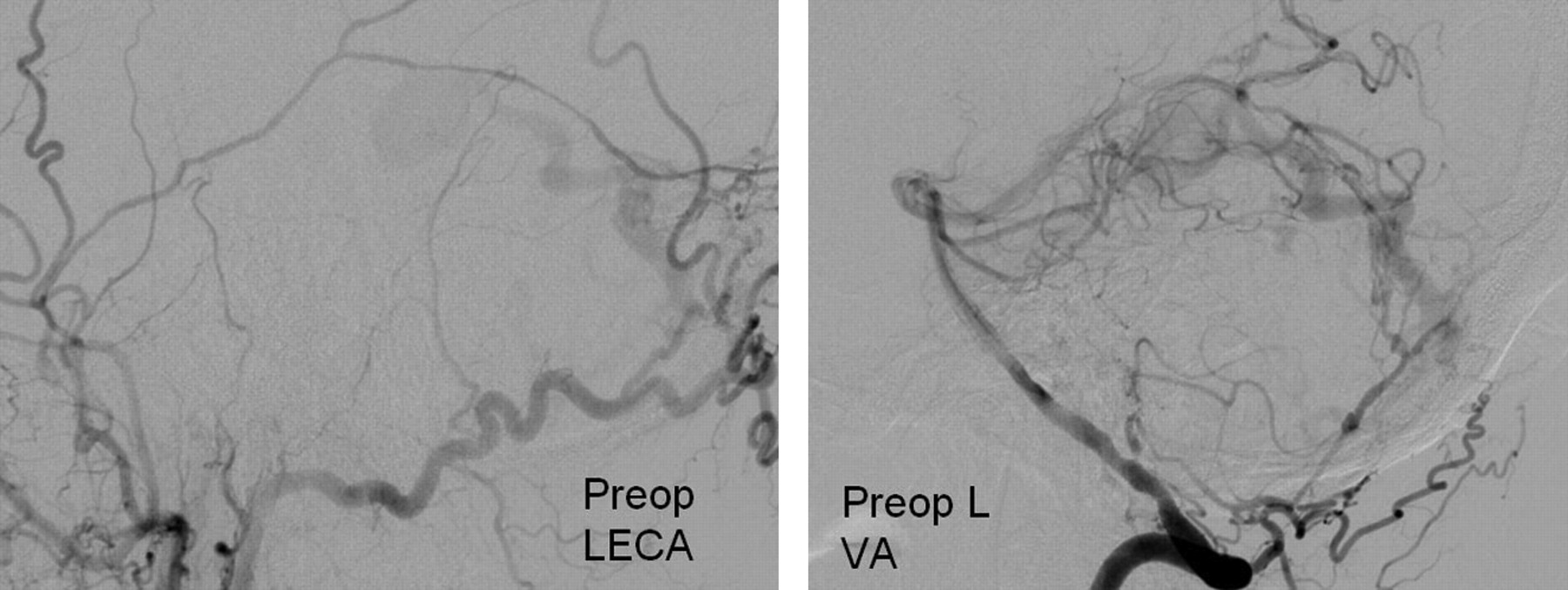
Preoperative angiogram with LECA and LVA injections showing a posterior fossa DAVF with feeders from the left occipital artery and the muscular/meningeal branches of the LVA, with a single large draining cortical vein. The patient underwent partial embolization of the fistula, and it was decided to treat the remaining portion of the fistula with surgery.

IA (left) showing no residual fistula. Postoperative angiogram, LECA and LVA injections, shows no residual fistula.
In 11 patients (37.9%), IA revealed residual fistula and an early draining vein after the surgeon determined that there was no residual fistula (Fig 3). The locations of these fistulas were the following: tentorial (n = 4), SSS (n = 3), cavernous sinus (n = 2), transverse-sigmoid (n = 1), and torcular (n = 1). Ten patients had immediate further exploration. One patient with a parietal parasagittal DAVF with bilateral dural and pial feeders had further surgical exploration at a later date. In 1 patient, a total of 3 intraoperative angiograms were obtained, while in another patient, 4 intraoperative angiograms were obtained. In all patients except 1, the final intraoperative angiogram was obtained before the surgeon closed. In 1 patient, however, the final angiogram was not obtained for logistic reasons. This patient had undergone 3 prior IAs, and the surgeon thought that there was no need for the fourth IA.

Preoperative left ICA injection, lateral projection showing a CCF. Following an unsuccessful attempt at endovascular treatment, it was treated surgically. The first IA shows evidence of residual fistula, after which the surgeon further packed the cavernous sinus. The second intraoperative angiogram and a postoperative angiogram show no evidence of residual fistula.
In all patients, IA could be performed in all the vessels intended. There was no complication related to the IA procedure. In 1 patient with a torcular DAVF, IA also identified a surgical complication in the form of occlusion of the posterior sss. Attempts to open up the sinus by both surgery and endovascular methods proved unsuccessful. In another patient with a cavernous sinus DAVF who underwent packing of the sinus, IA identified parent vessel (ICA) occlusion, which occurred during the packing of the sinus. This patient had excellent cross-flow through the anterior communicating artery and did well postoperatively and on follow-up. Postoperative angiography confirmed the parent vessel occlusion, as revealed by IA.
False-negative IA findings occurred in 3 patients (10.3%). In all these patients, IA revealed that there was no residual fistula, but a postoperative study revealed a residual one. The locations of these fistulas were the following: torcular (n = 1), transverse-sigmoid (n = 1), and temporal-middle fossa (n = 1). In 1 of these patients with a temporal-middle fossa DAVF, there was a doubtful residual fistula on IA; however, better visualization was not possible and hence it was reported as near-complete excision. All these fistulas had very slow flow. The 3 residual fistulas were treated respectively with repeat surgery, embolization followed by surgery, and embolization. At the end of the treatment, none of the patients had any residual fistula.
Of the 44 IAs, 41 correctly predicted (93.2%) either the presence or absence of residual fistula. In 3 of the 44 angiograms (6.8%), there was an incorrect finding attributable to the IA. There was no false-positive result, meaning that when the IA showed the presence of a residual fistula, it was a correct finding. Hence the sensitivity and specificity of IA were 82.3% and 100%, respectively, while positive and negative predictive values were 100% and 90%, respectively (Table). The incidence of residual fistula was higher in tentorial (4/6, 75%), SSS (3/4, 75%), and cavernous sinus (2/4, 50%) locations compared with others like torcular (1/3, 33%), transverse-sigmoid (1/9, 11%), middle fossa (0/3, 0%), and foramen magnum (0/3, 0%). However on χ2 testing, the difference between the location of the DAVF and the presence of residual fistula on IA was not statistically significant because of the low number in each group.
Sensitivity, specificity, and predictive values
Discussion
Some DAVFs are preferably treated with surgery due to the anatomy and angioarchitechture of the DAVF. Surgery for vascular malformations is aimed at complete obliteration of the lesion, to protect against future hemorrhage risk. Partial excision/obliteration of AVMs or DAVFs does not offer protection against future hemorrhage risk and, in many reports, increases the risk of hemorrhage in the postoperative period.26,27,34,35 Various surgical techniques, including packing of the sinus, skeletonization of the sinus, disconnection of the feeders, as well as disconnection of the leptomeningeal venous drainage, have been described.9–11,13,36–40 Although it has been mentioned in many surgical series that routine IA for DAVF is recommended and is useful, there is no report specifically analyzing the role of IA in surgery for DAVF, to our knowledge.
Many authors have published their experience with IA in surgery for aneurysms and AVMs.15–16,18–22,24,28–33 IA has been used for many years to look for the presence or absence of a residual shunt before closure, particularly with AVMs.17,28,29 The advantage of performing an intraoperative study is that it alerts the surgeon to an unexpected finding, and the surgeon can re-explore to excise the residual malformation, thus avoiding a second surgery in many instances. This also serves to protect against the high risk of rebleed associated with a small residual vascular malformation.
Vitaz et al18 described a large series of 91 patients with intracranial aneurysms and 98 patients with AVMs. The initial angiographic findings caused the surgical procedure to be modified in 29% of the patients with an AVM. In all these patients, there was a small residual nidus not apparent on microscopic examination. Three or more intraoperative angiograms were obtained in 10% of the patients. Other authors have also reported similar findings, though their rates of residual AVM on intraoperative angiogram are lower.15,22,41 Yanaka et al24 reported their experience in 20 patients with vascular malformations, 2 of which were DAVFs, and found an unexpected residual nidus in 1 patient (5%). They also reviewed the literature and found a residual nidus confirmed by IA in 13.5% of patients. The false-negative rate of IA was 4.6%, while the complication rate related to IA was 2.1%.
IA in patients with DAVFs is especially challenging because the arterial feeders to the fistula can be bilateral, from both the ICA and ECA, as well as from the vertebral artery. The examination might warrant cannulation of multiple arteries for a complete study, depending on the angioarchitecture of the DAVF. In the present series, 13 patients (44.8%) underwent cannulation of multiple vessels for their IA.
We found a relatively high rate of residual DAVF after the surgeon's assessment of complete obliteration of the DAVF. Eleven patients (37.9%) had residual DAVFs on IA, leading to further surgical exploration in all of these patients. This is higher than the residual nidus reported in most series of IA in AVM.15,22,41 It might be explained by the fact that DAVFs do not have a compact nidus. In many patients, packing of the sinus or skeletonization of sinus with obliteration of the feeders is the treatment, and it is difficult to examine the adequacy of the packing and obliteration of the fistula without radiologic evidence. Intraoperative Doppler evaluation frequently yields false-positive findings for residual fistula, when IA demonstrates complete obliteration. Furthermore, concern about overpacking a sinus or performing additional arterial/venous occlusions (if the DAVF was actually obliterated) with the potential risk of incurring cranial nerve or other neurologic deficits often prompted additional IAs. We found a higher incidence of residual fistulas in patients with cavernous, tentorial, and SSS fistulas and a lower incidence for transverse-sigmoid sinus fistulas. This high rate of residual nidus after microscopic surgery leads us to advocate IA in patients with DAVF undergoing surgery. In addition to revealing residual nidus in 11 patients, IA also depicted an unnoticed complication in the form of sinus occlusion.
There was 1 patient in this series who demonstrated residual fistula on IA but did not have a final angiogram to show that there was no further residual. This patient had undergone 3 prior IAs, and the surgeon thought he should not examine the patient an additional time. In general, however, the neurosurgeon found that the demonstrated evidence of continued fistula when it was thought the fistula had been completely obliterated was very valuable.
Limitations of IA
False-negative results were seen in 3 patients (10.3%) and 3 of the 44 angiograms (6.8%). This may be attributed to the slow flow of the DAVF. In addition, at the time of surgery, the patient's blood pressure may well be lower, resulting in poorer filling of the fistula. The false-negative rates of IA for AVMs range from 1.8% to 5.2%.15,16,18,24,41 Although IA helped to avoid a repeat surgery in 10 patients, it cannot replace postoperative angiography as the criterion standard to verify complete cure of the fistula following surgery.
The other objection to IA may be the complication rate associated with the procedure. The complication rates in the previous IA studies ranged from 1.7% to 3.7%, most of which occured in the femoral artery.15,16,18,20,41 The central nervous system complications attributed to the procedure were <0.5% in all the series. In the present series, there were no problems attributed to IA.
Patient positioning for the surgical procedure may create an additional challenge for IA. Fourteen IAs (14/34, 41.2%) were performed while the patients were in either a lateral or three-quarter prone position. Successful IA could be performed in all these patients. Lang et al31 presented their experience of 21 patients in whom IA was performed in patients in the prone or three-quarter prone position. They described 2 different approaches, an extended femoral sheath approach and a radial approach. In the present series, all the angiograms could be obtained with the patient in a lateral or three-quarter prone position, with the femoral sheath inserted before positioning.
Conclusions
IA is an extremely important adjunct in the surgery for DAVF. In this series, IA was technically possible in all the patients, and good-quality images could be obtained with cannulation of multiple vessels. IA resulted in further surgical treatment in 37.9% of patients. However, there was a 10% false-negative rate, which justifies subsequent postoperative angiography. IA appears to be a relatively safe investigation, with no complications attributed to it in the present series.
References
- Received August 28, 2010.
- Accepted after revision October 19, 2010.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}