
Abstract
SUMMARY: Subacute MTX-induced encephalopathy is characterized by an abrupt onset of focal neurologic deficits within days after intrathecal or systemic therapy. Demyelination is one proposed mechanism. We describe the neuroimaging features of 2 patients with clinical symptoms of subacute encephalopathy after intrathecal and systemic MTX therapy. DWI showed restricted diffusion, indicating cytotoxic edema. MTI yielded no evidence of demyelination in either patient because there was no loss of MTR in areas of restricted diffusion.
Abbreviations
- ADC
- apparent diffusion coefficient
- ALL
- acute lymphoblastic leukemia
- DWI
- diffusion-weighted imaging
- IT
- intrathecal
- IV
- intravenous
- MTI
- magnetization transfer imaging
- MTR
- magnetization transfer ratio
- MTX
- methotrexate
In the prophylaxis of central nervous system leukemia, IT MTX has largely replaced cranial irradiation and has lead to improved survival outcomes.1 Toxic effects of MTX include mucositis, myelosuppression, nephrotoxicity, hepatotoxicity, and neurotoxicity with acute (within hours), subacute (days to weeks after administration), and chronic (after months and years) encephalopathy.2
Subacute MTX-induced encephalopathy is characterized by a delayed onset of strokelike symptoms, such as aphasia, hemiparesis, and ataxia. Complete resolution of symptoms after therapy is usually seen in patients with encephalopathy. The pathophysiology of MTX-induced encephalopathy is incompletely understood. Demyelination and adenosine release have been proposed to contribute to the development of the disease.3–5
DWI has been used to diagnose cytotoxic edema in subacute MTX-induced encephalopathy6 but does not assess demyelination. MTI is a diagnostic tool known to be sensitive to demyelination.7 We report on 2 cases of subacute MTX- induced encephalopathy following IT MTX therapy in pediatric patients with ALL, who presented with typical neuroimaging without signs of demyelination on MTI.
Case Reports
Patient 1, a 13-year-old girl with biphenotypic ALL, received chemotherapy according to the COALL-07–03 protocol (high-risk standard).8 Twelve days after the third treatment with 12 mg of IT MTX, she developed prickling sensations and a central facial nerve paresis on the right side.
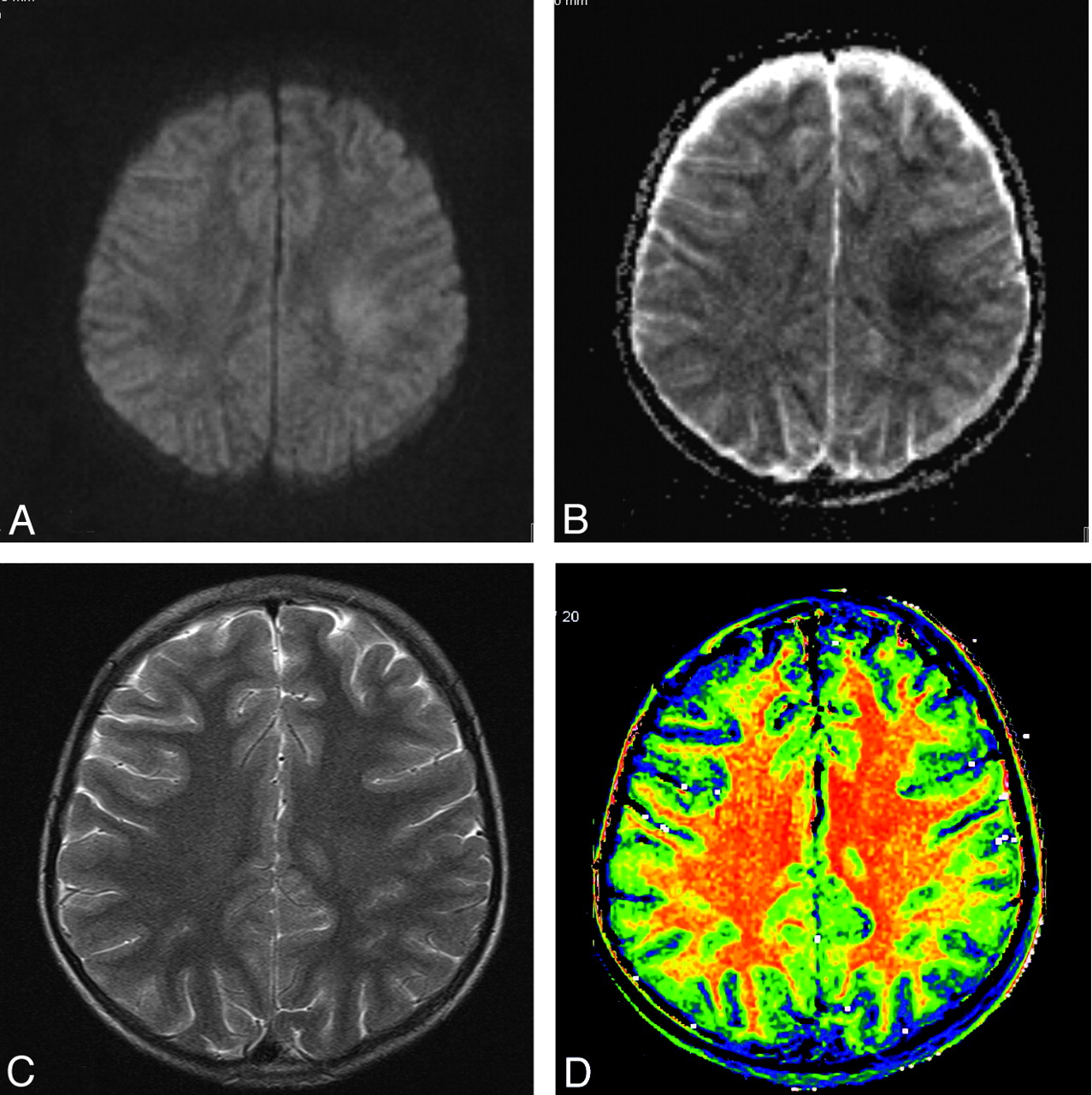
Conventional MR imaging showed changes on T2-weighted imaging with faint hyperintensity of the white matter in both hemispheres. DWI hyperintensity and low ADC were observed in the centrum semiovale of both hemispheres, corresponding to restricted diffusion.
MTI used two 2D gradient-echo sequences. The first acquisition had no saturation pulse. The second used a saturation pulse 1.2 kHz below H2O frequency. The MTR is the percentage of signal-intensity loss induced: MTR = (S0 − Ss) / S0 × 100%, where S0 is the signal intensity of a pixel obtained from the sequence without the saturation pulse and SS is the signal intensity with the saturation pulse.
MTR maps showed symmetric values of the white matter, and there was no loss of MTR in areas of DWI or T2 hyperintensity (Fig 1). Contrast-enhanced T1-weighted images and time-of-flight angiography findings were normal.

A, Diffusion-weighted image shows bilateral white matter hyperintensity. B, ADC map with low ADC is suggestive of cytotoxic edema. C, T2-weighted image shows white matter hyperintensity. D, MTR map shows normal white matter without signs of demyelination.
Treatment with 600-mg vitamin B6, 50-mg vitamin B12, and 2 × 80 mg of tetrahydrobiopterin per day was started. Her neurologic status improved quickly. Seven days later, no more neurologic problems could be detected.
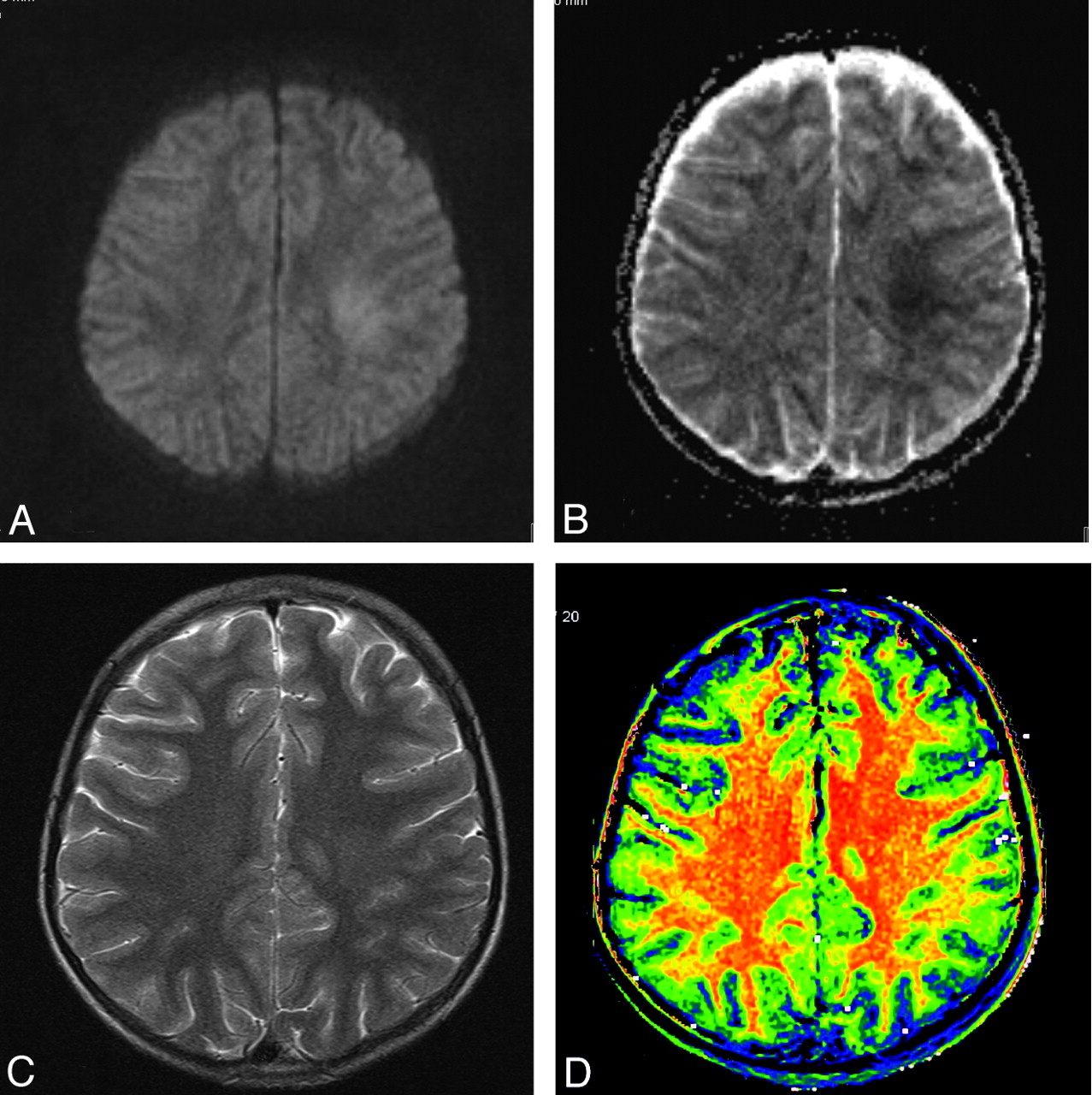
Patient 2, an 11-year-old girl, was treated with the protocol ALL-BFM 20009 for central nervous system negative precursor ALL. Ten days after the third series of high-dose IT MTX, the patient developed inarticulate speech, paraesthesia of the left arm and leg, and a hemiparesis of the left body. Cranial MR imaging showed a focal hyperintensity on T2-weighted images in the left centrum semiovale and restricted diffusion, 3.5 hours after the onset of symptoms. MTI findings were normal, with symmetric and homogeneous MTR of the white matter of both hemispheres (Fig 2).
A, Diffusion-weighted image shows bilateral white matter hyperintensity. B, ADC map shows low ADC, suggestive of cytotoxic edema. C, T2-weighted image shows white matter hyperintensity. D, MTR map shows normal white matter without signs of demyelination.
The treatment started with 600-mg theophylline, 600-mg vitamin B6, and 100-μg vitamin B12 per day and 30-mg folic acid every 6 hours. Due to clinical deterioration, the treatment with theophylline was discontinued the next day and a tetrahydrobiopterin therapy was initiated. Vitamin B12 and B6 were continued. Within a few days, the symptoms vanished. The treatment continued according the ALL-BFM 2000 protocol without any further MTX therapy.
Discussion
Subacute MTX-induced encephalopathy is a rare complication after chemotherapy including systemic or IT MTX in pediatric patients with cancer. The acute onset of focal neurologic deficits within days after chemotherapy with vincristine and intravenous high-dose MTX was first described in 1978 in children receiving chemotherapy for osteosarcoma.10 MTX encephalopathy has an incidence of 1%–3%11 in association with high-dose MTX and IT MTX therapy in children with ALL.12 Symptoms include hemiparesis, bilateral weakness, dysphasia, confusion, and movement disorders. Symptoms may fluctuate and spread to involve both hemispheres.6 Resolution of neurologic symptoms usually occurs within days.
DWI hyperintensity with low ADC was typical in subacute MTX-induced encephalopathy.6 T2 hyperintensity developing in several days has been reported to be irreversible in some cases.12 To the best of our knowledge, no reports of MTI in this condition are available in the literature. Our imaging findings are consistent with cytotoxic edema in both cases. The absence of vascular pathology and the patients' symptoms within 14 days after IT MTX are in accordance with subacute MTX-induced encephalopathy.
The pathogenesis of subacute MTX-induced encephalopathy remains incompletely understood. Demyelination has been a proposed mechanism in the development of this condition3,4 based on a study by Chu et al,5 who reported increased choline/creatine ratios in MR spectroscopy 20 weeks after combined IV-IT MTX in children treated for ALL, interpreted to be indicative of a myelinization disorder. Conversely, Davidson et al13 found low choline/water ratios after high-dose IV MTX, reported to reflect disturbances of myelin metabolism.
We used the MTR in our patients as a means of imaging known to be sensitive to demyelination.7 In a number of demyelinating conditions, such as multiple sclerosis,14 experimentally induced demyelination in vitro,15 and neuropsychiatric systemic lupus erythematodes,16 studies have demonstrated the decrease of MTR.
Our cases revealed no differences in the MTR between white matter areas with and without cytotoxic edema. We conclude that subacute MTX-induced encephalopathy may not be the result of toxic demyelination.
Footnotes
F.R. Miese and F.R. Schuster contributed equally to the report. Report concept and design and data acquisition and analysis/interpretation; manuscript revision for intellectual content and approval of the final version of the submitted manuscript: F.R. Miese, F.R. Schuster, K. Pierstorff, M. Karenfort, H.-J. Laws, A. Borkhardt and A. Saleh. Manuscript drafting: F.R. Miese, F.R. Schuster. Guarantor of the integrity of the entire study: A. Saleh. Literature research, MR imaging studies analysis, and manuscript editing: F.R. Miese, F.R. Schuster, M. Karenfort, H.-J. Laws, A. Borkhardt, and A. Saleh.
References
- Received April 14, 2010.
- Accepted after revision April 16, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.