
Abstract
BACKGROUND AND PURPOSE: Recent research showed a strong correlation of calcium volume scores with degree of stenosis, suggesting that calcium volume could be used in the diagnosis of carotid artery stenosis. We investigated the accuracy of the use of calcium volume scores to diagnose carotid artery stenosis in our target population of recently symptomatic patients.
MATERIALS AND METHODS: Ninety symptomatic patients suspected of having carotid artery stenosis underwent CTA, resulting in images of 159 evaluable arteries. The correlation between calcium volume and degree of stenosis was calculated by using the Pearson correlation coefficient. With thresholds of 0.03 and 0.09 mL, we assessed the diagnostic performance of a calcium volume−based evaluation of stenosis for a previously reported stenosis cutoff of 40% and for the clinically important cutoffs of 50% and 70%.
RESULTS: In our patients series, the calcium volume score was not related to the stenosis degree on the symptomatic side (R = 0.04, P = .7) and was weakly related on the asymptomatic side (R = 0.29, P = .005). The diagnostic accuracy of the calcium volume score to estimate 40% stenosis was relatively low: a sensitivity of 47% or 64% and a specificity of 52% or 82%, for the 0.09 and 0.03 mL thresholds, respectively. The diagnostic accuracy decreased with increasing degree of stenosis.
CONCLUSIONS: We could not confirm the previously reported strong correlation of calcium volume with stenosis degree in our population of patients with recent neurologic symptoms. We conclude that in this particular domain, calcium volume cannot be used to estimate the degree of stenosis.
Abbreviations
- CEA
- carotid endarterectomy
- CTA
- CT angiography
- DSA
- digital subtraction angiography
- ICA
- internal carotid artery
- MPR
- multiplanar reformations
- NASCET
- North American Symptomatic Carotid Endarterectomy Trial
- NPV
- negative predictive value
- PPV
- positive predictive value
- ROC
- receiver operating characteristic analysis
- SD
- standard deviation
- VR
- volume-rendering
Carotid artery stenosis is an important risk factor for ischemic stroke. Large randomized trials showed that CEA is beneficial for recently symptomatic patients with a severe stenosis (70%–99%).1,2 Subgroups of patients with a 50%–69% stenosis may also still benefit from CEA.3 The degree of stenosis is a strong predictor for outcome; therefore, precise assessment of the degree of stenosis is crucial in the decision to perform CEA. In these trials, the degree of stenosis was assessed with intra-arterial DSA. Since then, the noninvasive technique, CTA, has increasingly been used to assess the degree of carotid artery stenosis.4 A systematic review of CTA versus DSA in determining stenosis grade revealed a pooled sensitivity of 85% and a specificity of 93% for detection of a 70%–99% stenosis.5
Previous studies suggested a correlation between calcium volume and the degree of stenosis in coronary and carotid arteries. The amount of coronary artery calcification determined by CT correlates with coronary artery stenosis of >50%.6 There are many differences between coronary and carotid artery disease; however, similar relations have been found for the carotid arteries: Severe calcification of the carotid siphon was correlated with a >50% carotid stenosis in the study of Woodcock et al.7 In a recent study of McKinney et al,8 a relatively strong correlation between calcium volumes at the carotid artery bifurcation and the degree of stenosis of the ICA has been demonstrated. In another study, the quantitative calcium burden of the common and extracranial ICAs was associated with luminal stenosis.9 These findings suggest that calcium may play an important role in the vulnerability of plaques and that calcium volume measurement may be a useful tool in selecting patients suspected of having carotid stenosis.
Previous studies on carotid artery stenosis have been performed on neurologically asymptomatic patients with various indications, mostly evaluating head and neck cancer,10 and on a population of 32 asymptomatic patients and 21 patients with ischemic neurologic symptoms.9 The aim of our study was to determine the value of carotid calcium volume scoring in a patient population in which accurate stenosis-degree measurement is of utter importance: symptomatic patients suspected of having carotid artery stenosis, for which carotid artery surgery is considered.
Materials and Methods
According to our local medical ethics committee and because the tests were performed in the clinical setting, informed consent did not have to be obtained.
Patient Selection
In our center (Academic Medical Center, Amsterdam, the Netherlands), symptomatic patients suspected of having carotid artery stenosis are primarily evaluated by duplex sonography. With sensitive cutoffs (ie, when stenosis degree is >30% [male] or >50% [female]), subsequent CTA is performed according to current guidelines.11
All consecutive patients who underwent CTA for carotid stenosis evaluation between April 1, 2006, and December 31, 2008, and all patients who underwent CTA on a 64-section CT scanner were included in our evaluation. Patients with a previous carotid intervention and those with CTA studies of insufficient quality were excluded.
CT Imaging Protocol
CTA scans were performed with a 64-section scanner (Brilliance 64; Philips Healthcare, Best, the Netherlands). An 18-gauge intravenous catheter was placed in the antecubital vein and 80 mL of contrast (iodixanol, Visipaque 320; GE Healthcare, Milaukee, Wisconsin) was infused at 4 mL/s after an initial injection delay, depending on an attenuation of 150 Hounsfield units in the aortic arch. Acquisition and reconstruction parameters were as follows: 120-kV tube voltage, 265 effective mAs, pitch of 0.765, section thickness of 0.9 mm, increment of 0.45 mm. The scan ranged from the aortic arch up to 3 cm above the sella turcica.
Stenosis Measurements
Manual stenosis measurements were performed by a senior neuroradiologist (C.B.L.M.M) by using a review workstation with MPR functionality (Impax, Version 5.2; Agfa-Gevaert, Mortsel, Belgium). The method of Bartlett et al10 was used to determine the narrowest diameter in a plane that was perpendicular to the center lumen line of the vessel. A central axis of the lumen image was used when determining the narrowest diameter by a caliper tool. In determining the stenosis degree by using NASCET criteria, the distal ICA diameter was measured by using the same method in a plane at least 2 cm above the site of narrowing or plaque. In addition, the arteries were categorized according to the standard carotid stenosis degrees1: minimal stenosis (0%–29%), mild stenosis (30%–49%), moderate stenosis (50%–69%), severe stenosis (70%–99%), and occlusion (100%).
NASCET stenosis measurements of carotid arteries with a near-occlusion are fallacious because of a reduction of the distal diameter. Therefore, carotid arteries with a near-occlusion according to the criteria of Bartlett et al12 were excluded to avoid correlation to inaccurate stenosis degrees.
In general, all patients who undergo the diagnostic tests in the clinical setting are symptomatic, according to our guidelines. Retrospective analysis of our patient cohort, however, showed that 4 patients should be considered asymptomatic according to the definition. In all patients, the 2 carotid arteries were labeled as “symptomatic side” or “asymptomatic side,” with regard to the symptomatic hemisphere. In the 4 asymptomatic patients and in patients who had symptoms from the posterior circulation, both carotid arteries were labeled “asymptomatic.”
Calcium Volume Scores
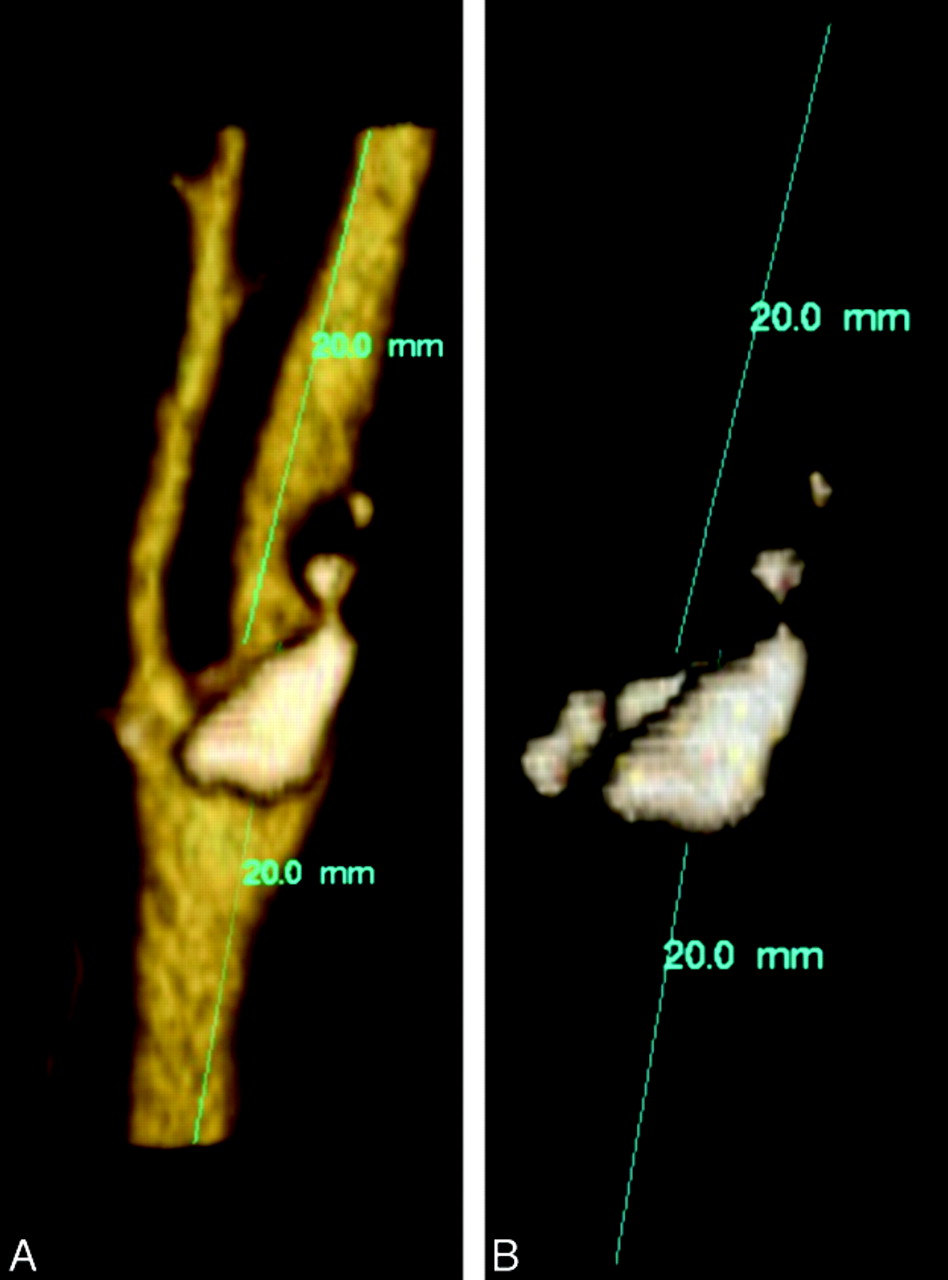
To acquire calcium volume scores, a single observer (L.S.) who was accustomed to the software used the same method and workstation as McKinney et al8 (Vitrea 2, Version 4.1.2.0; Vital Images, Minnetonka, Minnesota). This method consists of carefully “sculpting” 2 cm below and above the bifurcation by drawing the area intended for inclusion so that other high-attenuation structures were excluded from calcium scoring (Fig 1). After this, window level and width were manually altered to maximize the amount of visualized calcium while not including vascular contrast (level: 250–500; width: 10–20). The resulting calcified plaque volume was measured in milliliters by using the volume calculation function of the workstation.
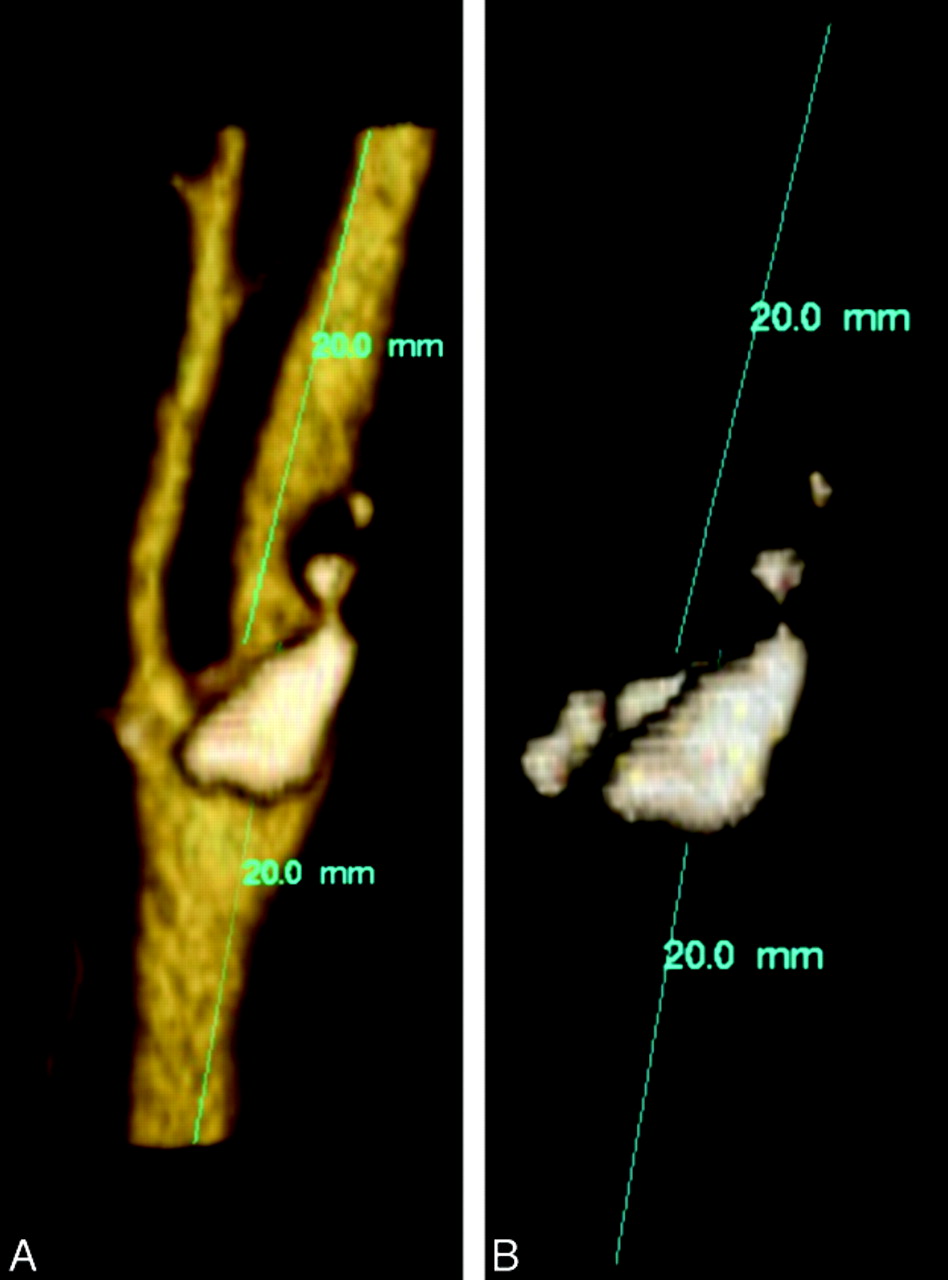
Illustration of the calcium volume measurement according to the method of McKinney et al.8 First, the carotid bifurcation is sculpted (left). After further adjustment of the window level and width, only the calcium is displayed (right). With the volume calculation tool, the calcium volume is displayed.
Statistical Analysis
Pearson correlation coefficients (R) were calculated to determine the correlation between the calcium volume scores and the degree of stenosis. The statistical significance of R was tested by using a t test. Correlations were calculated for all arteries combined and for the symptomatic and asymptomatic sides separately. The sensitivity, specificity, PPV, and NPV of a previously reported calcium volume–based stenosis measurement of ≥40%8 was determined in our patient population. Ninety-five percent confidence intervals were calculated. The chosen calcium volume thresholds used in our test were the largest (0.09 mL) and smallest (0.03 mL) that performed well in the study of McKinney et al.8 We extended this analysis by calculating the sensitivity, specificity, PPV, and NPV for the clinically crucial thresholds of 50% and 70% with regard to the decision on carotid endarterectomy. ROC curves were constructed for the stenosis thresholds of 40%, 50%, 60%, and 70%.
Results
Data were available for 170 consecutive patients who underwent CTA specifically for assessment of a carotid stenosis according to our protocol. One hundred forty-eight patients were scanned on a 64-section CT scanner; 113 scans from these patients had the required 0.9-mm section thickness.
We excluded patients for the following reasons: previous carotid intervention (n = 17; stent placement, n = 13 and CEA, n = 4); scans of insufficient quality (n = 2); scans with nonvisualization of the carotid bifurcation (n = 2); and scans visualizing additional pathology (n = 2; carotid dissection, n = 1 and fibromuscular dysplasia, n = 1), resulting in scans of 90 patients with suspected artery stenosis. The mean age was 66.8 years (range, 35–89 years), and the male-female ratio was 1.46.
Of the 180 ICAs available, 21 near-occlusion arteries were excluded, resulting in 159 carotid arteries used in the statistical analysis. One of the 90 patients had a posterior cerebral artery stroke. Of the 159 arteries, 67 were labeled “symptomatic side”; 92, “asymptomatic.”
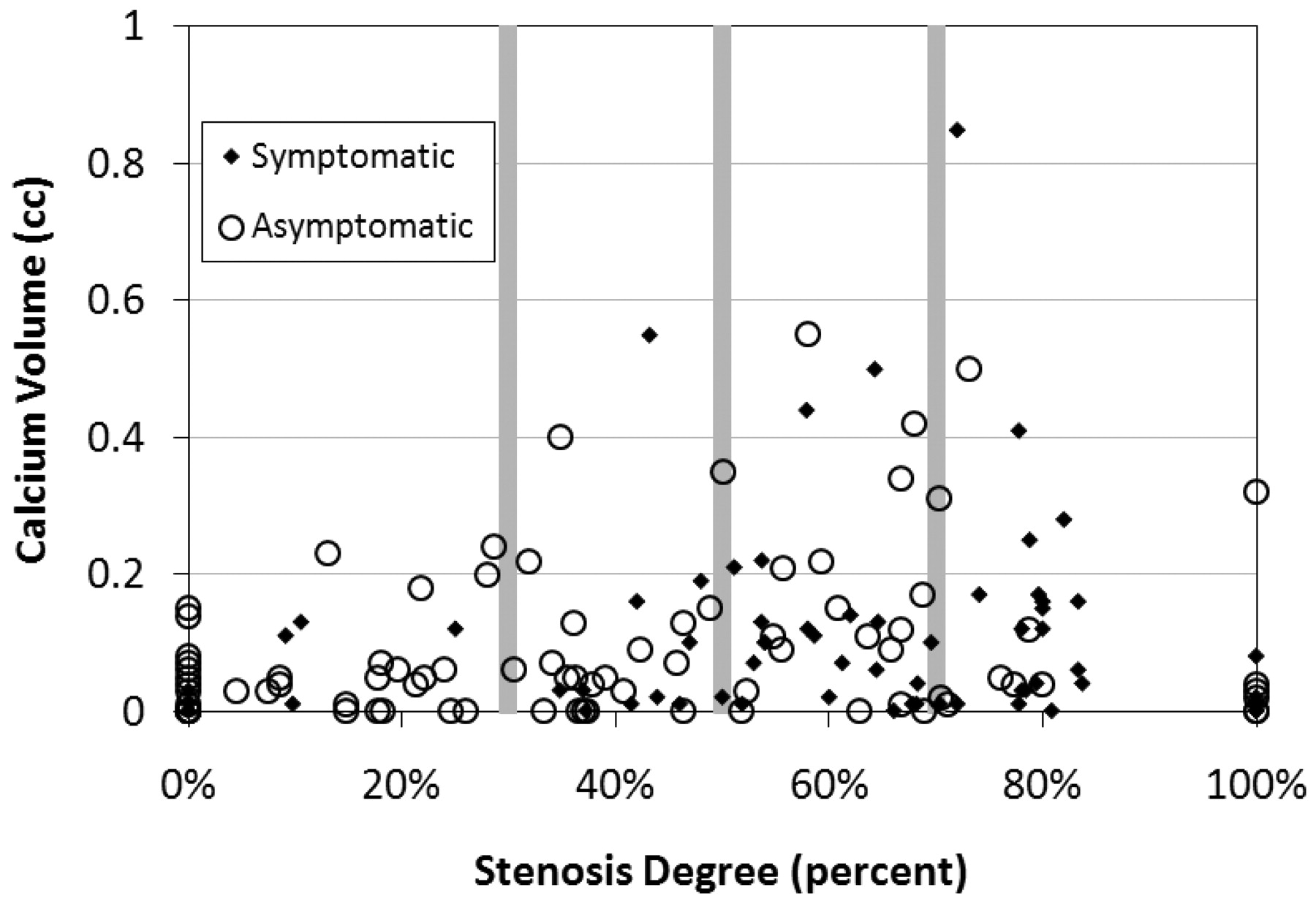
Figure 2 shows all measurements of the combined calcium volumes and stenosis degrees. One hundred twenty-five of 159 carotid arteries demonstrated measurable carotid bifurcation calcification. The volume of the carotid bifurcation calcium ranged from 0 to 0.85 mL. The mean calcium burden was 0.10 ± 0.13 mL. Twenty-one arteries with a nonzero stenosis contained no measurable calcium burden. The largest calcification burden without a measurable stenosis was 0.15 mL. The largest calcification burden for a minimal-stenosis classification was 0.24 mL.
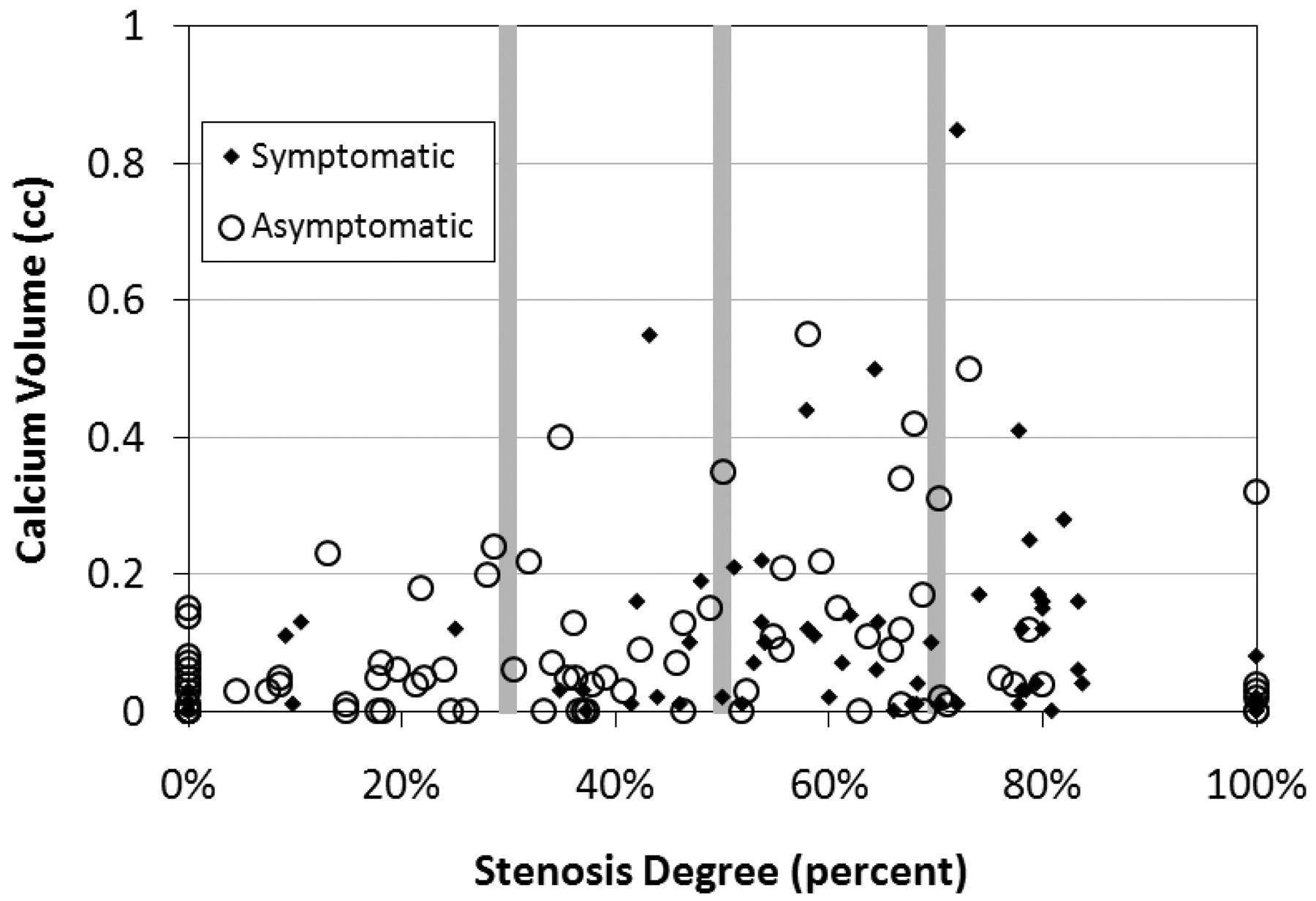
Scatterplot showing all measurements for the symptomatic and asymptomatic ICAs. The stenosis categories are illustrated with the gray vertical lines.
One hundred forty-three of 154 carotid arteries have a nonzero stenosis according to the NASCET criteria. The measured stenosis degree of the ICA ranged from 0% to 100% with a mean of 47% and an SD of 31%.
Calcium volume measurements for the stenosis categories for all and for the symptomatic and asymptomatic arteries are given in Table 1. This Table shows that there was a large spread of calcium volume for all stenosis categories. It also shows that there was no significant difference between the symptomatic and asymptomatic side. For the symptomatic side, a small not significant increase was shown with the increasing stenosis category up to the severe category. For the asymptomatic side, the increase was up to the moderate category, and the calcium volume decreased with the severe and occlusion categories. The calcium burden for the occluded arteries was smaller than that for mild category up to severe category. For all stenosis classifications, at least 1 artery with a zero calcification volume was present.
Calcium volume for stenosis degree groupsa
Table 2 shows the computed correlations between calcium volume and stenosis degree. For all arteries, there was a weak correlation (R = 0.20, P = .012). For the symptomatic side, there was no correlation (R = 0.04, P = .7); the asymptomatic side showed a weak correlation (R = 0.29, P = .005).
Average calcium volume, stenosis degree, correlation for symptomatic and asymptomatic arteries, and the combination of botha
Ninety-four arteries had a stenosis of >40%; 81 arteries, >50%; and 41 arteries, >70%. The performance of the tests for detecting a stenosis of >40%, 50%, and 70% is presented in Tables 3⇓–5, respectively. For the 70% stenosis test, only the results for a volume threshold of 0.09 mL are shown. The performance of the 0.03 mL threshold was even worse.
Performance of the calcium volume test determining a stenosis degree of ≥40%a
Performance of the calcium volume test determining a stenosis degree of ≥50%a
Performance of the calcium volume test determining a stenosis ≥70%a
In general, there was a low sensitivity: 37% for the 0.09-mL and 65% for the 0.03-mL threshold, respectively. The PPV was larger for the symptomatic side. The NPV was larger for the asymptomatic side. Comparing Tables 3⇑–5 shows that the sensitivity, specificity, and PPV all decreased with increasing stenosis degree. Only the NPV increased with increasing stenosis degree, especially for the asymptomatic side.
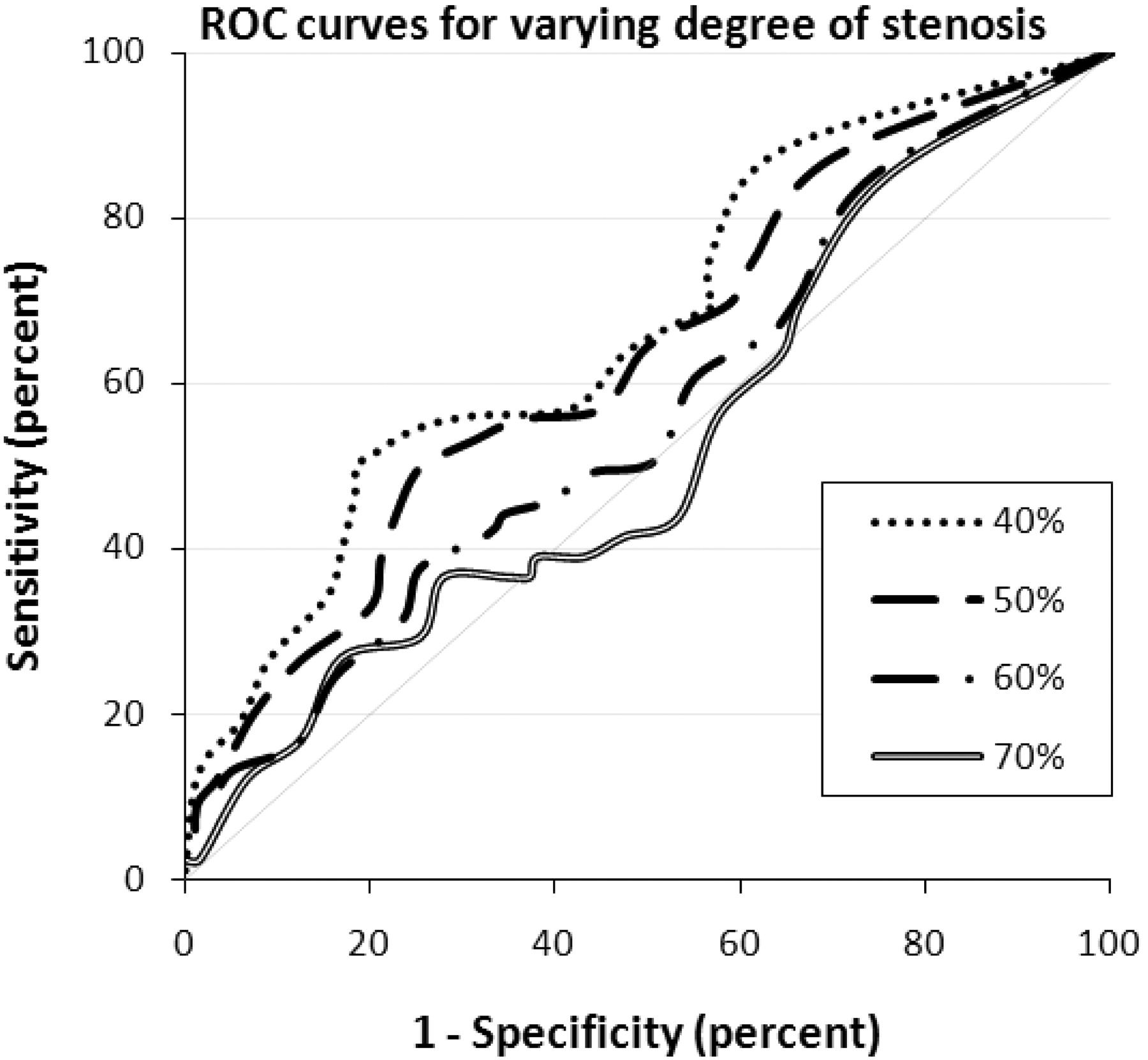
Figure 3 shows the ROC curves for stenosis determination of >40%, 50%, 60%, and 70%. This figure also illustrates that the performance of the calcium volume−based test decreased with increasing stenosis degree. We did not observe a significant difference of the ROC curves between the symptomatic and asymptomatic sides, and these were, therefore, not plotted.
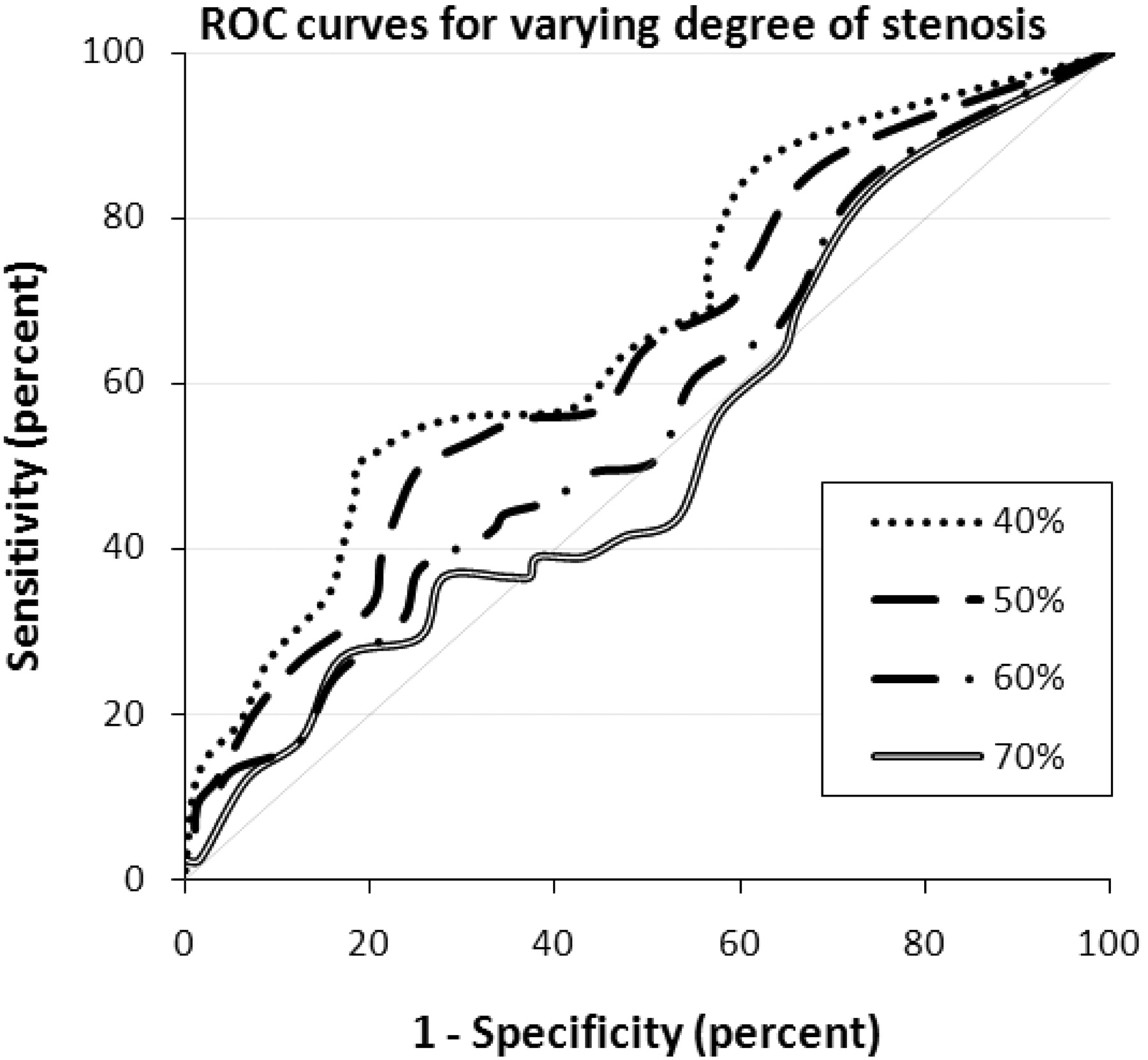
ROC curves for various calcium volume−based degrees of stenosis determination, illustrating the sensitivity and false-positive rate (1-specificity) for the tests. The best possible test yields a point in the upper left corner; a random guess gives a point along the diagonal line. The higher the curve is from the diagonal, the better the prediction test. This figure illustrates that the performance of the calcium volume−based stenosis determination decreases with increasing stenosis degree.
Discussion
In our population of patients with recent neurologic symptoms and in which carotid endarterectomy was considered, we found no correlation between carotid calcium volume and the degree of stenosis at the ICA for the symptomatic side and only a weak relationship for the asymptomatic side. Also the diagnostic accuracy of calcium volume−based evaluation of significant stenosis was significantly lower than that reported previously. We were, therefore, not able to reproduce previously reported correlations.8 We conclude that the calcium volume measurement cannot be used to estimate the degree of stenosis in patients with recent neurologic symptoms and in whom carotid endarterectomy is considered
The calcium volume measurement seemed an attractive alternative to stenosis measurements because its visualization can be established with CT scanning without contrast material administration. Moreover, CT scanning for calcium measurements can be performed with less radiation burden than high-resolution images for stenosis measurements. An additional score for high-grade stenosis could also reduce the commonly observed high inter- and intrauser variability of the carotid stenosis degree.13
The volume of the calcium burden in the cardiac coronary arteries is a well-established predictor for cardiac events. Recently, a correlation between the calcium burden and stenosis degree has been established for a patient population of suspected head and neck neoplasms8 and a combined patient group of asymptomatic patients and patients with ischemic neurologic symptoms.9
The main difference between this study and the 2 previous studies is the domain. McKinney et al8 used a population that underwent CTA of the neck region for various indications, most of which were for evaluating head and neck neoplasms; the mixed patient population in the study of Nandalur et al9 consisted of both asymptomatic and symptomatic patients. Therefore, the observed correlation between calcium volume score and carotid artery stenosis was obtained in a more “general” population. We wanted to test if calcium volume scores could be used to estimate the degree of stenosis in the domain of patients in which this information is crucial (ie, patients with recent neurologic symptoms such as transient ischemic attack or stroke) suspected of having carotid artery stenosis after screening with duplex sonography. In our patient series, the calcium measurement and its relation with the degree of stenosis were different from those of the previously studied patient populations (eg, calcium volumes 3 times as large as those in the population of McKinney et al). Except for the PPV, the results for our patient population were much lower than those reported by McKinney et al. We also observed that the calcium volume−based stenosis evaluation performs worse with increasing (clinically relevant) stenosis degree.
The detected correlation was slightly better for the asymptomatic side, also corresponding somewhat better to the previously reported results. This suggests that the relation between calcium and stenosis of carotid arteries on the asymptomatic side corresponds better than this relation in a general patient population as used in the previous studies.
We observed a number of notable differences between the symptomatic and asymptomatic sides: On the symptomatic side, the PPV was consequently larger than that on the asymptomatic side, meaning that a large calcium burden on the symptomatic side is related to a significant stenosis. This did not hold for the asymptomatic side. On the other hand, the NPV was consequently larger on the asymptomatic side. This means that for this side, the absence of large calcium volumes is related to the absence of a significant stenosis. Again, this relation was not observed on the symptomatic side. This difference becomes smaller for higher stenosis degree tests.
The calcium volume results in Nandalur et al9 were from manual tracing, which is not a sensible approach in clinical practice. Furthermore, in this study, all the calcifications of the common carotid artery and extracranial ICA are summed, whereas we only considered the calcifications at the carotid bifurcation. Also, Nandalur et al reported a stronger correlation when the calcification volumes of both the left and right arteries were summed than for individual vessels. This approach could improve the correlation as we have detected in our patient population; however, the determined very weak correlation suggests that an adjusted measurement would not result in a significant improvement. Furthermore, it has been reported that the stenosis degree correlates slightly better with the square root of the calcium volume.8 Due to the initial absence of a correlation in our patient population, we did not perform this approach.
The motivation for searching for a correlation between calcified volumes and stenosis degree is based on the idea that a stenosis is caused by the buildup of plaques in the vessel wall and that part of the plaques is calcified. Apparently, this elementary thought does not hold for a patient population with suspected carotid artery stenosis. This is illustrated with 2 representative cases: Fig 4 shows a patient with a significant-diameter stenosis of 75% according to the NASCET criteria with a calcium volume score of 0.01 mL. This figure shows that the lumen is surrounded by low-intensity material, indicating that stenosis is caused by the large soft plaque buildup in the vessel wall. Figure 5 shows a patient with a diameter stenosis of 29% according to NASCET criteria with a calcium volume score of 0.55 mL. This figure shows that despite a very large calcium burden, the lumen area is not decreased due to outward remodeling.

VR and MPR reconstructions showing a severe stenosis of 75% according to the NASCET criteria. B shows a display of calcium of the same bifurcation as in A. Total calcium volume is 0.01 mL.
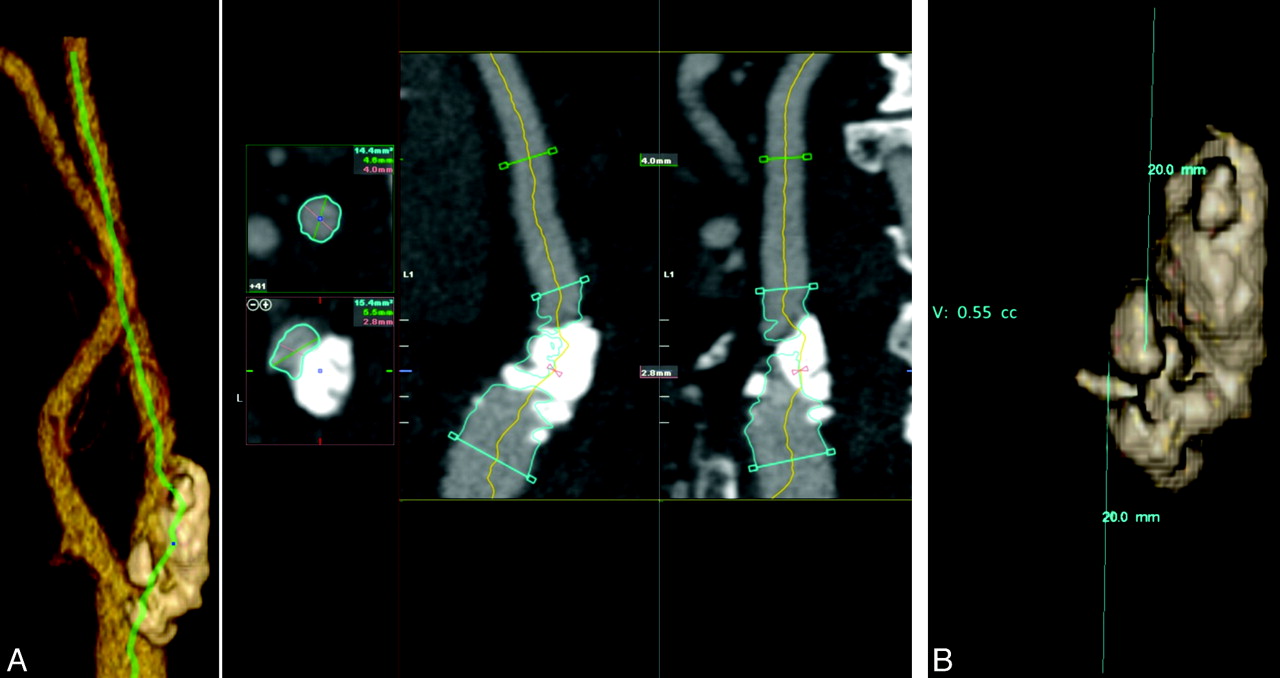
VR and MPR reconstructions showing a low-level stenosis of 29% according to the NASCET criteria. B is a display of calcium of the same bifurcation as Fig 4A. Total calcium volume is 0.55 mL.
The calcium volume score as obtained in CT images is not the actual volume of the calcified plaques. Due to the blooming artifacts, the size of the calcified plaques appears larger than it in reality is. The blooming artifacts are caused by the limited spatial resolution and blurring and create a spillover effect into adjacent voxels. Therefore, volume measurement is a combination of calcium volume, calcium intensity, and image blurring. Because the blurring is dependent on the reconstruction filter, different filters may yield different calcium volume scores.
Because our results indicate that for symptomatic patients, there is no relation between the degree of stenosis and the severity of stenosis, this finding may support the idea of soft atherosclerotic plaques being more of a risk for stroke than hard calcified plaques,13–16 which are associated with plaque stability, and supports the premise that (nonsubendothelial) plaque calcification is associated with plaque stability. This idea is supported by the fact that the occluded arteries had an average calcium volume score of only 0.04 mL. A more interesting approach would be to use the calcified plaque volume as a marker for ischemic symptoms.15 A recent study17 suggested that extensive calcification is more commonly associated with the asymptomatic side. However, Nandalur et al18 have shown that the ratio of calcified plaque volume and total plaque volume is significantly inversely associated with the occurrence of symptoms.
Conclusions
We could not confirm the results of previous studies relating calcium volume to the stenosis degree in our population of patients with recent neurologic symptoms suspected of having carotid artery stenosis. In this particular domain, the calcium volume measurement cannot be used to estimate the degree of stenosis.
Footnotes
-
Indicates Fellows' Journal Club selection
-

Disclosures: Lucas Smagge, Research Support (including provision of equipment and materials): Vital Images; Details: Company provided a laptop with Vitrea software as stated in the article. Laptop had to be returned to the company after use. No further support or conflicts. Hugo A. Gratama van Andel, Other Financial Relationships: Employee of Milabs B.V., Utrecht, the Netherlands; Details: During my PhD at the AMC, I was involved in the research of this article. After obtaining my PhD, I am now an employee of Milabs, a company that produces single-photon emission CT/positron-emission tomography/CT scanners for preclinical imaging. Because this article is not the result of my work for Milabs, only the AMC is mentioned in my affiliation.

References
- Received September 28, 2010.
- Accepted after revision November 22, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Does Vascular Calcification Accelerate Inflammation?: A Substudy of the dal-PLAQUE Trial
- Diagnostic Accuracy of 4 Commercially Available Semiautomatic Packages for Carotid Artery Stenosis Measurement on CTA
- Association Between Arterial Calcifications and Nonlacunar and Lacunar Ischemic Strokes
- Reply:
- Spectrum Bias: Patient Selection May Affect Performance of Calcium Volume in Detecting Carotid Stenosis