
Abstract
BACKGROUND AND PURPOSE: The relationship between the MR imaging features and clinical outcomes in patients with hypoglycemic encephalopathy has always been evaluated retrospectively. The aim of this study was to prospectively evaluate whether MR imaging features of patients presenting with hypoglycemic coma are predictive of short-term (1-week) outcomes.
MATERIALS AND METHODS: Subjects were 36 consecutive patients with hypoglycemia who were in a comatose state on arrival at our hospital from April 2006 to March 2010. MR imaging findings on arrival in relation to the patients' clinical course after glucose infusion were evaluated.
RESULTS: Thirteen of the 36 patients showed no MR imaging abnormalities on arrival. DWI revealed focal lesions involving the internal capsule in 13 patients and lesions involving bilateral hemispheric white matter in 10 patients. After glucose administration, the patients without lesions and patients with focal internal capsule lesions recovered completely within 1 day. However, patients with diffuse white matter lesions did not recover even within 1 week despite glucose administration. There was no statistical difference in the initial blood glucose levels among patients with the various types of MR imaging findings.
CONCLUSIONS: On early MR imaging, hypoglycemic brain injury may first appear in the internal capsule and then spread into the hemispheric white matter. The absence of a lesion or the presence of a focal internal capsule lesion may suggest a good outcome. However, diffuse hemispheric white matter lesions may indicate a poor 1-week outcome.
A sudden decrease in the serum glucose level may cause coma. Most hypoglycemic comatose patients regain consciousness after glucose infusion. However, hypoglycemia can cause irreversible brain damage that reduces the patient to a persistent vegetative state or death.
With widespread use of high-field MR imaging scanners, various MR imaging findings have been reported in patients with hypoglycemia. DWI in various cases has led to the identification and description of hyperintensity lesions in the cerebral cortex,1⇓⇓–4 basal ganglia,1,2,5 subcortical white matter,3,6,7 posterior limb of the internal capsule,4,6,8⇓–10 and splenium of the corpus callosum.4,7,8,10 A series of 11 patients with hypoglycemic encephalopathy in whom lesions were identified by MR imaging has been reported recently.11 The reports have all been based on retrospective evaluation of the MR imaging findings.
We conducted a prospective study in which we evaluated MR imaging findings with respect to early prognosis after glucose infusion in a consecutive series of patients hospitalized with hypoglycemic coma. The aims of the study were to document the evolution of hypoglycemic brain injury neuroradiologically and to determine the early MR imaging features of hypoglycemic brain injury that indicated reversible functional brain damage and those that indicated irreversible brain damage.
Materials and Methods
Design
The study was designed as a prospective observational study to be conducted at a single institution. The study was approved by the institutional ethics committee. Oral informed consent was obtained from patients' family members.
Patients
Subjects were identified from among 114 patients with hypoglycemia who visited our emergency department between April 2006 and March 2010. The patients who were included in the study were transferred to our hospital in a comatose state on arrival and diagnosed with hypoglycemia by blood laboratory tests. In this study, patients with borderline blood glucose levels (40–69 mg/dL) were included when they had a history strongly suggestive of hypoglycemia such as insulin overdose. We excluded patients with another underlying condition that could contribute to their mental state, such as hypoxia, hypotension, or hypothermia detected by a vital-signs monitoring system in the emergency department; acidosis, infection, or intoxication detected by blood laboratory tests; or epilepsy suspected by focal or generalized seizure. Thus, the final study group comprised 36 patients. When hypoglycemia was diagnosed, patients were treated immediately with 40 mL of 50% glucose, administered intravenously. Thereafter, patients' blood glucose levels were maintained at 150–200 mg/dL. Blood glucose levels and MR imaging findings on arrival and changes in the neurologic and MR imaging findings during the first week after admission were evaluated; after the first 1-week period, some patients were discharged from our hospital or transferred to another hospital for rehabilitation.
MR Imaging
Each comatose patient underwent brain MR imaging, including DWI on arrival just after blood sampling as long as the patient had no contraindication for MR imaging such as an implanted cardiac pacemaker. Follow-up MR imaging was performed on the following day (day 2) if a DWI abnormality (lesion) was found on arrival. If the DWI abnormality had not disappeared by day 2, additional MR imaging was performed 1 week after admission. All MR imaging studies were performed with a 1.5T Symphony MR imaging scanner (Siemens, Erlangen, Germany). Imaging sequences of the brain included spin-echo T1-weighted, T2-weighted, FLAIR, and DWI sequences. From DWI, ADC maps were constructed. The MR imaging parameters were as follows: for T1-weighted imaging: TR/TE = 525–570/12–14 ms, matrix = 256 × 230; for T2-weighted imaging: TR/TE = 3550–4000/107–113 ms, matrix = 269 × 448; for FLAIR imaging: TR/TE/TI = 8580–9000/77–107/2200–2300 ms, matrix = 272 × 320; and for DWI: TR/TE = 3200/95 ms, matrix = 128 × 102, b = 1200 s/mm2. For all imaging sequences, the section thickness was 5 mm and the FOV was 22 × 22 cm.
Analysis
Clinical and MR imaging evaluations of each patient were done by one of the authors (K.J., Y.N., or Y. Kudo) who examined the patient in the emergency department. Signal intensities of lesions were visually assessed on all MR imaging sequences. Results of the first MR imaging evaluations were confirmed by another author who was blinded to clinical data (T.N.Y. or Y. Kuroiwa).
After the initial DWI study (on admission), patients were divided into groups according to the initial findings. ANOVA was used to examine between-group differences in patient age and blood glucose levels on arrival. JMP, Version 7 (SAS Institute, Cary, North Carolina) was used for all statistical analyses. P < .05 was considered statistically significant.
Results
There appeared to be no significant differences in the patients' consciousness levels. All 36 patients were incapable of sensing or responding to verbal and painful stimuli on arrival; there were no patients who lost brain stem reflexes such as the pupillary reflex or who developed decorticate or decerebrate postural changes.
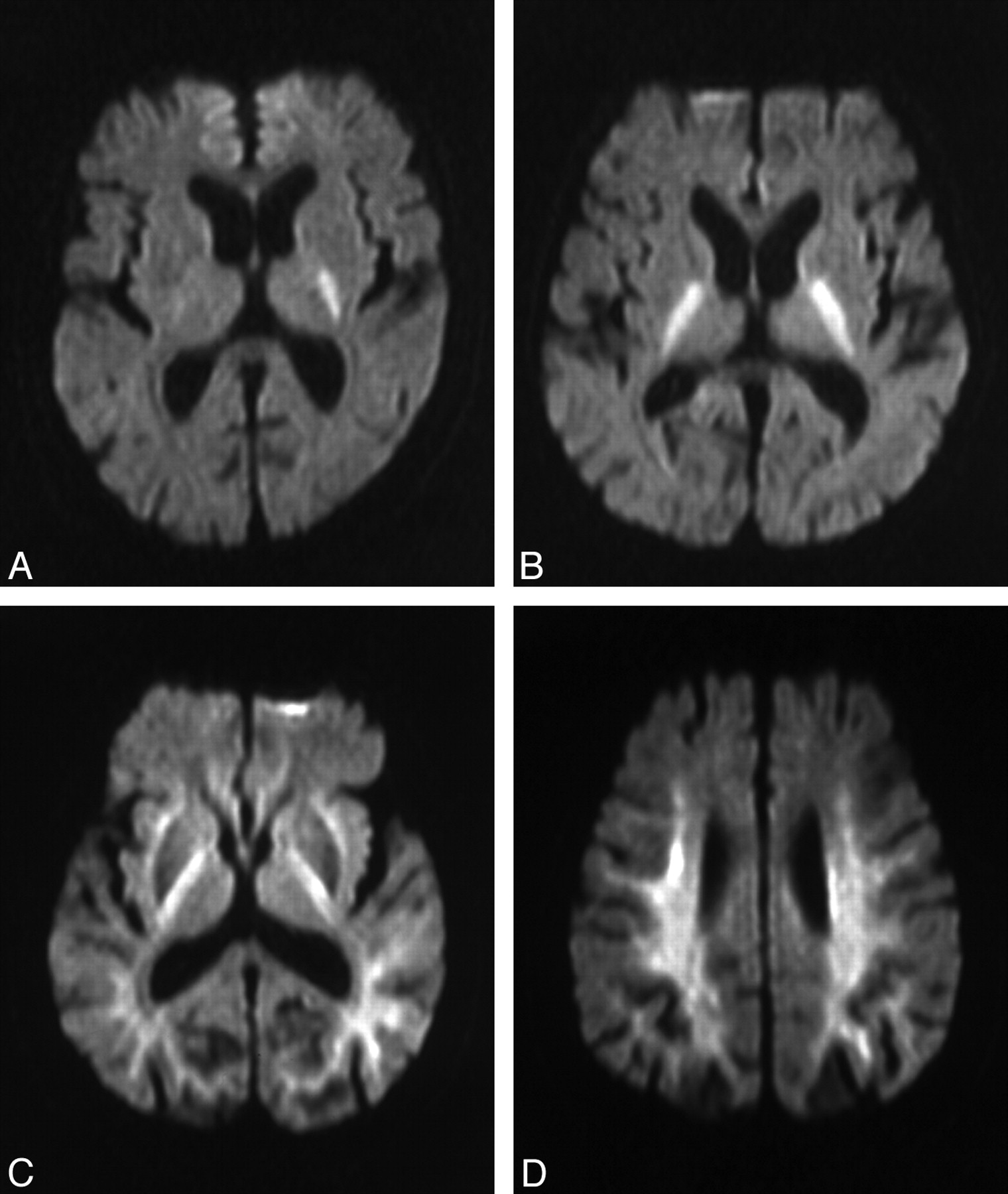
DWI on arrival showed areas of abnormal hyperintensity in 23 of the 36 patients. In 13 of these 23 patients, hyperintensity lesions corresponding to hypointense signals on an ADC map were seen in the posterior limb of the internal capsule; the internal capsule lesions were bilateral in 7 patients, left-sided in 4, and right-sided in 2 (Fig 1A, -B). Additional focal lesions involving other highly directional large white matter tract fibers were seen in 2 of the 13 patients; one had a lesion in the cerebellar peduncle, and the other, in the splenium of the corpus callosum in addition to the internal capsule lesion (Table 1). These lesions were not detected in other MR imaging sequences (Fig 2A–E). In the remaining 10 patients, diffuse hyperintensity lesions with decreased ADC involved the bilateral hemispheric white matter, including the corona radiata and centrum semiovale, in addition to the internal capsule (Fig 1C, -D). The basal ganglia were also involved in 4 of the 10 patients in whom diffuse white matter lesions were identified on arrival; in 2 of the 4 patients with basal ganglia lesions, the cerebral cortices were also involved (Table 2).

Two different DWI lesion patterns in patients with hypoglycemic coma are indicative of 2 different outcomes. When focal lesions involving the posterior limb of the internal capsule (eg, patient 4, unilateral lesion, A; patient 9, bilateral lesions, B) were seen, outcomes were good. C and D, However when diffuse lesions involving bilateral hemispheric white matter including the internal capsule, corona radiata, and centrum semiovale (eg, patient 19), were seen, outcomes were poor.
Clinical characteristics of comatose patients with hypoglycemia with focal DWI lesions

Example of a hypoglycemic lesion in the internal capsule depicted by MR imaging (patient 4). DWI (A) reveals a hyperintensity lesion with decreased ADC (B). No lesion is seen in other MR imaging sequences such as FLAIR (C) and T2-weighted (D) and T1-weighted (E) sequences. F, The DWI lesion disappeared completely next day.
Clinical characteristics of comatose patients with hypoglycemic and diffuse DWI lesions
Initial DWI showed the absence of abnormal hyperintensity areas in 13 comatose patients with hypoglycemia. These 13 patients regained consciousness immediately after glucose infusion. The 13 patients with hyperintensity lesions involving the internal capsule also regained consciousness within 1 day after glucose infusion; they were without any neurologic deficit. It took several hours to recover in this group. Transient hemiparesis was observed in 4 of these 13 patients before their full recovery. The hyperintensity lesions disappeared completely by day 2 (Table 1 and Fig 2F). On the other hand, the 10 patients with diffuse white matter lesions did not regain consciousness by day 2 despite continuous adjustment of their blood glucose levels: Two patients died, 5 patients remained in a vegetative state, and 3 patients remained totally dependent during the next week due to severe disorientation. The white matter lesions did not disappear by day 2 or by 1 week after admission. In fact, basal ganglia lesions became more conspicuous by day 2 in 1 of these patients (Fig 3). These lesions became visible in other MR imaging sequences such as T2-weighted and FLAIR sequences after day 2. The white matter lesions became slightly less visible after 1 week (Fig 3).

Follow-up images of hemispheric white matter and basal ganglia lesions on DWI (A, B, E, F, I, J) and FLAIR (C, D, G, H, K, L) (patient 21). The white matter lesions on arrival (A−D) did not disappear by day 2 (E−H) or by 1 week (I−L) after admission. The basal ganglia lesions became more conspicuous by day 2 (E−H) and became slightly less visible after 1 week (I−L).
Mean blood glucose levels of patients without hyperintensity lesions on arrival (mean age = 72.7 years), patients with focal lesions involving the internal capsule (mean age = 76.2 years), and patients with diffuse white matter lesions (mean age = 81.0 years) were 26.5, 29.8, and 35.0 mg/dL, respectively. There were no statistical differences in age or blood glucose levels among the 3 groups.
Discussion
Neuroradiologically, our patients with hypoglycemia who were in a comatose state on arrival comprised 3 groups: 1) patients without hyperintensity lesions; 2) patients with focal lesions involving highly directional large white matter tract fibers of the internal capsule (and sometimes involving other fibers of the cerebellar peduncle or splenium of the corpus callosum); and 3) patients with diffuse lesions involving bilateral hemispheric white matter including the internal capsule, corona radiata, and centrum semiovale (and sometimes the basal ganglia or cerebral cortices). There are previous reports of lesions involving not only white matter but also gray matter in patients with hypoglycemic encephalopathy; selective involvement of gray matter has also been reported in such patients.11,12 In our study, however, most lesions were localized in the white matter. This difference in the topographic lesion pattern may arise from the severity of the disease and the time of the MR imaging study. Hypoglycemic comatose patients were included in our study regardless of the absence of MR imaging abnormalities. MR imaging was performed prospectively in all patients upon arrival. However, previously reported subjects were included only when MR imaging studies, performed within the first several days after admission, revealed areas of abnormal signaling.11,12 Thus, the previous reports might have included only the most serious cases of hypoglycemic encephalopathy, whereas we included patients at various stages of hypoglycemic encephalopathy. In 1 of our patients (patient 21), gray matter lesions were more conspicuous on day 2 images than on the initial images. Thus, it might be possible that in some of the previously reported patients, gray matter lesions had developed by the time MR imaging studies were performed.
Our findings suggest that in comatose patients with hypoglycemia, the absence of hyperintensity lesions or the presence of only focal lesions involving the internal capsule on initial DWI predicts complete recovery within 1 day after glucose administration. Indeed, immediate recovery after glucose infusion in patients with DWI-detected focal lesions involving the internal capsule or other large white matter tract fibers has been reported previously.4,7⇓⇓–10 Our findings also suggest that diffuse lesions involving hemispheric white matter are a sign of a poor 1-week outcome despite glucose administration. Previously, both poor outcomes2⇓–4,11 and good outcomes6,11 were reported for patients with diffuse white matter lesions on initial DWI. However, when outcomes were good, it took several weeks for patients to recover completely.6,11 Although 1-week outcomes were poor for our 10 patients with diffuse white matter lesions, gradual recovery might be expected during the next several weeks.
There was no significant difference in blood glucose levels on admission between patients grouped according to the 3 imaging patterns. Lack of correlation between initial blood glucose levels and prognosis has been reported.4,12 It might be that the duration of the hypoglycemic state, not the blood glucose level, reflects the prognosis of patients with hypoglycemic encephalopathy. Evaluation of the relationship between the duration of hypoglycemic state and the prognosis of patients will be needed in the future.
Glucose deprivation leads to severe energy failure and induces massive release of excitatory amino acids.13 Excessive excitatory amino acid levels cause cytotoxic edema (ie, excitotoxic edema affecting neuronal and glial cells).14 Early brain change in hypoglycemia is thought to comprise the excitotoxic edema that propagates through neuron–glial cell units and through transaxonal or trans-synaptic routes along the white matter tracts.14,15 White matter lesions observed on MR images in our patients with hypoglycemic encephalopathy may result from this excitotoxic edema. When excitotoxic edema, detected by DWI focally involves large white matter tract fibers such as the internal capsule, irreversible hypoglycemic neuronal damage may be minimal.14 However, when the excitotoxic edema spreads diffusely to the hemispheric white matter, there is irreversible neuronal damage, mainly in the cerebral cortices and basal ganglia, which are thought to be the areas most vulnerable to glucose deprivation.1
Our study had several limitations. It was designed as a prospective study, but initial MR imaging evaluation was not done by an observer blinded to clinical data. The possibility of other concomitant brain damage such as hypoxic-ischemic encephalopathy was not completely ruled out. Initial and outcome neurologic measurements of the patients were too simplified. Longer follow-up data, especially in patients with diffuse white matter lesions, may be needed.
Conclusions
To the best of our knowledge, ours is the first-reported prospective observational study of early MR imaging in comatose patients with hypoglycemia. The white matter lesion pattern depicted by DWI seems to have prognostic significance: No lesions or only focal lesions involving the internal capsule on initial DWI suggest complete recovery within 1 day after glucose administration, whereas diffuse lesions involving hemispheric white matter seem to be a sign of a poor 1-week outcome despite glucose administration.
References
- Received July 4, 2011.
- Accepted after revision September 5, 2011.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Hyperglycemia selectively increases cerebral non-oxidative glucose consumption without affecting blood flow
- Suspecting unwitnessed hypoglycaemia
- Neuroimaging in Patients with Abnormal Blood Glucose Levels
- Diffusion-Weighted Imaging Changes Caused by Acute Hypoglycemia and Prolonged Febrile Convulsion in Childhood
- Diagnostic approach to restricted-diffusion patterns on MR imaging