
Abstract
SUMMARY: The past decade has seen an increase in the number of articles reporting the use of DTI to detect brain abnormalities in patients with traumatic brain injury. DTI is well-suited to the interrogation of white matter microstructure, the most important location of pathology in TBI. Additionally, studies in animal models have demonstrated the correlation of DTI findings and TBI pathology. One hundred articles met the inclusion criteria for this quantitative literature review. Despite significant variability in sample characteristics, technical aspects of imaging, and analysis approaches, the consensus is that DTI effectively differentiates patients with TBI and controls, regardless of the severity and timeframe following injury. Furthermore, many have established a relationship between DTI measures and TBI outcomes. However, the heterogeneity of specific outcome measures used limits interpretation of the literature. Similarly, few longitudinal studies have been performed, limiting inferences regarding the long-term predictive utility of DTI. Larger longitudinal studies, using standardized imaging, analysis approaches, and outcome measures will help realize the promise of DTI as a prognostic tool in the care of patients with TBI.
ABBREVIATIONS:
- FA
- fractional anisotropy
- GCS
- Glasgow Coma Scale
- MD
- mean diffusivity
- TAI
- traumatic axonal injury
- TBI
- traumatic brain injury
- TBSS
- tract-based spatial statistics
The clinical pathology underlying TBI-related impairment is traumatic axonal injury.1 TAI, referred to as diffuse axonal injury when damage is extensive, is a microscopic injury that occurs even in the absence of frank tissue disruption. Therefore, patients may experience significant impairment despite the absence of abnormal findings on conventional CT and MR imaging. Moreover, focal imaging abnormalities that can be detected by using CT and MR imaging are poor predictors of outcome.1 Diagnostic tests that can discriminate significant TAI are needed to effectively allocate patients to follow-up and treatment, to accurately assess injury severity and safety in sports and military settings, and to guide clinical trials of novel therapeutic agents. DTI is a relatively new MR imaging technique that measures the directional coherence of water diffusion in vivo. Because of the highly uniform collinear structure of normal white matter, DTI is uniquely able to probe its microscopic structure and is, therefore, particularly well-suited for the assessment of TAI. Although gross abnormalities can be identified in some cases of TAI by using CT and conventional MR imaging, DTI can both qualitatively and quantitatively (Fig 1) demonstrate pathology not detected by other modalities and is, therefore, an important tool not only in the research setting but in the clinical setting as well.
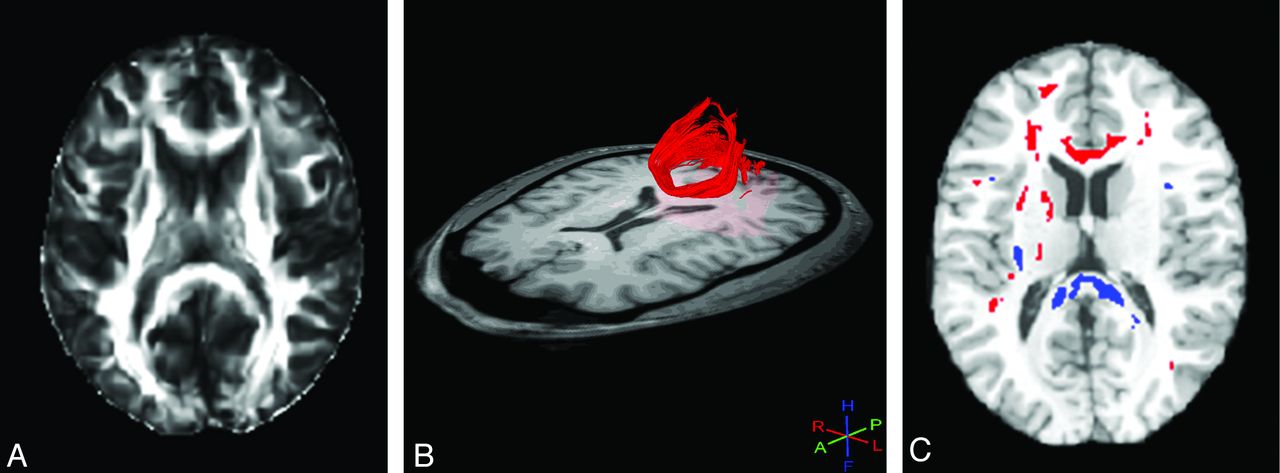
FA image (A) reveals no abnormality in a patient with TBI. Tractography (B) can be used to delineate a region of interest for analysis. In this case, the forceps major (red) appears normal, but quantitative analysis of FA within this tract showed lower FA in the TBI group compared with controls. Whole-brain voxelwise analysis (C) reveals areas of low (blue) and high (red) FA. Low FA, consistent with TAI, is present within the forceps major at the splenium of the corpus callosum, as well as elsewhere.
Most studies of TBI report fractional anisotropy, a summary measure derived from DTI, which describes the directional coherence (anisotropy) of water diffusion within tissue. However, mean diffusivity, axial diffusivity, and radial diffusivity may more specifically describe the direction and magnitude of tissue water diffusion. Animal studies have shown a direct correspondence between even very subtle TAI pathology and decreases in white matter anisotropy that can be imaged in vivo by using DTI (eg, Mac Donald et al2). Numerous clinical studies have assessed TBI by using DTI. Since the earliest research article reporting DTI applied to TBI was published in 2002,3 there has been an overall exponential increase in the number of articles published on this topic (Fig 2).

The number of publications per year reporting DTI in TBI.
The purpose of this review was to systematically summarize and detail the landscape of DTI applied to the study of TBI and to highlight both the salient conclusions to be drawn from this large literature and its limitations, which can serve as important considerations for future research. We summarize a number of different aspects of the articles, including the demographics of TBI subjects and controls, the timing and severity of TBI, technical factors related to image acquisition and analysis, the nature and location of abnormalities, and findings relating DTI to outcome measures. We also note that a valid meta-analysis of this literature is not feasible due to the great diversity in study design and measurement approaches used across the articles.
A structured search was performed by using PubMed to include all relevant articles through 2011. The search used the following key word combinations: “diffusion tensor imaging and traumatic brain injury,” “DTI and TBI,” and “DTI and concussion.” The total results included 391 articles with 293 unique articles. We further examined the references cited by these articles to identify additional relevant articles. After we eliminated articles on the basis of our exclusion criteria (below), 100 articles3⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–102 remained and were systematically analyzed and included in this review. Exclusion criteria included the following: language other than English (n = 7); animal or in vitro studies (n = 30); studies of diseases other than TBI (eg, spinal cord injury, brain tumors) (n = 57); case reports (n = 37), reviews (n = 48), editorials (n = 3), posters (n = 1), or abstracts (n = 1); and use of diffusion-weighted imaging or other MR imaging measures, but not DTI (n = 8).
Subjects with TBI
The population studied or substrate of injury is perhaps as important as the TBI itself in determining the nature and extent of consequent pathology.103 An important consideration in the study of TBI is thus the choice of the study sample and the feasibility of attaining a homogeneous cohort. A total of 2337 subjects was studied across all 100 articles. The average number of patients per study was 23 (range, 5–83 subjects). Our review identified several articles that described patient samples with extremely similar or identical demographic characteristics (eg, McCauley et al55 and Wilde et al,87,88,90) but reported either different abnormal brain regions or different analyses of DTI in relation to outcome. Thus, some of the subjects may have been reported in multiple studies published by the same group of researchers. Our best estimate is that the number of subjects reported in multiple studies may be up to 140 individuals. All except 8 articles reported sex breakdown; 65% of reported subjects were male.6,30,41,46,52,77,81,83
Most commonly, abnormalities on DTI are defined on the basis of comparison with a control group because universal thresholds for abnormality have not yet been established. All studies, except 5, compared subjects with TBI with a control group.17,18,24,83,85 Three of these exceptions used a longitudinal within-subjects design.24,83,85 In all except 7 studies, control subjects were healthy individuals.28,43,49,53,55,81,90 In 3 of the studies that did not use healthy individuals as control subjects, 2 groups of subjects with TBI were compared (eg, with and without major depressive disorders53). In 3 pediatric studies, the control groups were children who were hospitalized for orthopedic injury but had no evidence of head injury.43,55,90 The average number of control subjects per study was 18 (range, 6–47). Several articles, in addition to comparing patients with TBI with controls by using DTI, looked at subgroups of patients with TBI, including patients with TBI with major depressive disorders,53,99 with raised intracranial pressures,81 with spinal cord injuries,86 or veterans with blast injuries.41,49,53,79,99 An important consideration in the selection of control subjects, particularly when studying symptom endorsement, is that comparison of subjects with TBI with healthy controls fails to eliminate the potential confound of morbidity due to the experience of trauma itself, rather than adverse outcomes specifically due to physical injury to the brain. At the same time, it is unclear whether a purportedly non-head-injured patient sustained neurologic trauma during the course of an injury, even if not reported by the patient or witnesses of the event or detected by clinical assessment of the patient.
The ages of subjects studied across all articles ranged from 2 through 70 years, with each individual article reporting on a more limited age range. Children were studied exclusively in 29 of 72 articles.4,5,11⇓⇓–14,17,19⇓⇓–22,25,27,42,43,55,66,75,81,87⇓⇓⇓⇓⇓⇓–94,96,98 The total number of children studied across all 29 articles was 564. In addition, 20 studies included adults and children (younger than 19 years).8⇓⇓–11,26,31,49,50,56,59,60,62,64,65,67,70,83,84,97,99 However, varied age thresholds were used to define the pediatric population. Most studies defined the pediatric population as individuals younger than 17 years of age, but other studies included children up to 18 years,4,5,92 19 years,75 20 years,12⇓–14 or 22.5 years of age.81 White matter changes associated with normal development might confound detection of white matter injury; moreover, because developmental changes can occur at different rates even in children of the same chronologic age, use of DTI in the pediatric population is a challenging undertaking.
Many studies reported the mechanism of injury of patients with TBI such as motor vehicle collisions, falls, and assaults. However, because patients with different mechanisms were almost always consolidated into a single patient group, it is impossible to draw conclusions about imaging findings as they relate to different mechanisms of injury.
Because age, sex, anthropometrics, and injury mechanism can greatly influence outcomes, it is important that these issues be considered in study design and interpretation of results. Two major issues therefore emerge in consideration of the demographics of a TBI population. First, it is important to frame the comparison of results from multiple studies in the context of demographic differences between the studied samples. Second, within a single study, a group analysis involving a demographically diverse sample might mask important findings unique to a particular demographic subset or lead to spurious group differences.
Severity, Chronicity, and Study Design
Traumatic injury to the brain can result in a spectrum of injuries. There is a lack of consensus regarding whether they represent subsets of a single-entity or distinct pathologic processes. We found a wide variation in the injury severity studied, ranging from mild, in which there is a complete absence of abnormalities on conventional imaging, to severe, in which subjects remain in a vegetative state. While some studies were restricted to patients of a specific injury severity, many studies included patients of varying severities. For studies reporting the GCS, we defined severity as mild (GCS, 13–15), moderate (GCS, 9–12), or severe (GCS, 3–8). For articles that did not report the GCS but characterized severity as mild, moderate, or severe, we accepted the authors' report of severity. Four studies did not report injury severity.26,33,53,60 Several articles distinguished between mild-complicated and mild-uncomplicated TBI. While both groups of patients exhibited GCS in the mild range (>13), patients with mild-complicated TBI had findings of TBI on conventional imaging (CT and structural MR imaging), whereas patients with “true” mild or mild-uncomplicated TBI did not. Some articles specifically reported a distinction between patients with mild-complicated and mild-uncomplicated TBI. Many articles, though not making the mild-complicated versus mild-uncomplicated distinction, specifically noted that subjects with mild TBI lacked significant findings on conventional imaging. However, other articles simply reported “mild” severity without mentioning the results of conventional brain imaging. There has been an increasing trend toward differentiating mild-complicated versus mild-uncomplicated injury beginning in 2009. The earlier literature did not make the distinction, referring to the injury as “mild” without qualification. This likely represents an increasing awareness of the distinction between mild-complicated and mild-uncomplicated, because studies have demonstrated that the clinical features of mild-complicated injuries often bear closer resemblance to those of moderate TBI than they do to mild-uncomplicated TBI.104 Finally, some articles did not differentiate moderate and severe TBI but, rather, grouped all such patients into 1 category.
Similar to severity, chronicity (Fig 3) is an important factor in the development of the study design. Primary injury and secondary injury play different roles in the evolution of pathology as a function of time postinjury. Similarly, microstructural pathology, as detected with DTI, may change with time. We found a wide variation among studies as to the timing of DTI relative to TBI, ranging from days to years. To systematically assess the timing of DTI after injury, which we termed “injury chronicity,” we divided subjects into 3 generally accepted categories. Acute injury included patients imaged within 2 weeks of TBI, while chronic injury included patients imaged at least 1 year following injury. The subacute period included imaging performed between 2 weeks and 1 year after TBI. All articles reported the timing of DTI after TBI.

The number of articles that studied patients at each timeframe and level of injury severity. Articles were only included if there was sufficient information to determine both the severity and the chronicity of individual patient injuries. Articles may be included multiple times if they studied subjects with multiple severities and/or multiple chronicities. A fully referenced version of this figure is available in On-line Table I.
Figure 3 details the total number of articles reporting DTI for the study of TBI within a given timeframe and of a particular injury severity and includes articles that report mixed severities, mixed chronicities, or both. Most subjects were studied in the subacute setting (Fig 3), most commonly having severe TBI followed by mild TBI. This trend might be attributable to the greater ease of subject enrollment during the subacute period, rather than to the clinical importance of this timeframe for the study. Patients are more easily enrolled from rehabilitation centers, where they were actively seeking treatment for their injuries. In the acute setting, patients with mild TBI might not even seek medical treatment and patients with severe TBI were too involved in urgent treatment to participate in a research study. Unless identified retrospectively, patients are easily lost to follow-up at chronic time points. When categorized according to severity, independent of chronicity, the total number of patients with moderate TBI represented approximately half the total number of patients with mild TBI and half the total number of patients with severe TBI (Fig 3). Although the minority of patients studied across all severities was examined in the acute setting, use of DTI as a prognostic tool is dependent on the identification of early biomarkers; therefore, the acute setting is an important area for future research, as are longitudinal studies examining patients at both the acute and chronic time points.
Most articles used cross-sectional designs. Eighteen articles reported multiple groups of subjects who were imaged at various times postinjury,3,5,8,24,25,31,32,34,39,54,56,65,68,72,76,85,93,102 whereas 79 articles reported a single homogeneous group of patients all within a 1-injury chronicity timeframe. Only 13 articles, reporting a total of 283 patients, used longitudinal designs and imaged the same group of patients at 2 different time points (Fig 4).3,24,29,39,47,49,54,56,67,83,85,93,102 One additional article reported imaging of the same group of patients acutely and again at least 1 year following injury but used a cross-sectional analysis at each of these time points and did not report change with time within subjects.85

Thirteen studies used a longitudinal design. Numbers represent patients from all studies imaged at 2 time points. Nine studies assessed patients at both acute and subacute time points.3,29,39,47,54,56,67,83,85 One study assessed patients at both acute and chronic time points.102 Two studies assessed patients at both subacute and chronic time points.24,93 One study (n = 47) assessed patients twice during the subacute period and, therefore, was omitted from the figure.49
A prospective study of patients with TBI is difficult; attrition during follow-up is a significant challenge. Of those studies that used a longitudinal design, only 8 reported attrition. The average attrition rate across these studies was 0.32 (range, 0.11–0.60).3,24,29,49,54,56,83,85 Despite the challenge of attrition, longitudinal studies are integral to the understanding the natural history of TBI and for early prognostication.
Data Acquisition Parameters
Important considerations in the use of DTI are the strength of the magnetic field, the number of diffusion-sensitizing gradient magnetic field directions, and the choice of b-values. Use of greater magnetic field strengths has advantages and disadvantages; greater signal-to-noise ratio, improved spatial resolution, and faster scanning times commonly achieved at stronger magnetic field strengths come at the cost of increased magnetic field inhomogeneity. In the setting of clinical DTI, most facilities will choose a b-value between 750 and 1000, whereas b-values of up to 3000 are used experimentally.105,106 Increasing the b-value increases the sensitivity to diffusion, but with a decrease in signal-to-noise ratio. Encoding the direction of diffusion requires a minimum of 6 diffusion-sensitizing directions; greater resolution can be achieved by introducing additional directions, but this adds time to image acquisition. We summarize the acquisition parameters used in DTI studies of TBI as follows.
Nearly equal numbers of articles reported performing DTI at 1.5T and 3T (483⇓–5,8,15⇓⇓–18,24,26⇓–28,30⇓⇓⇓–34,38,39,42⇓–44,47⇓–49,52,55⇓⇓–58,66⇓–68,70,72,73,76,77,79,80,82,87,88,91,93,97,101,102 and 52,6,7,9⇓⇓⇓⇓–14,19⇓⇓⇓–23,25,29,35⇓–37,40,41,45,46,50,51,53,54,59⇓⇓⇓⇓⇓–65,69,71,74,75,78,81,83⇓⇓–86,89,90,92,94⇓–96,98⇓–100 respectively). The number of diffusion-sensitizing directions used ranged from 6 to 64, with an average of 27 but a mode of 12. In 2011 alone, the mode increased to 64. The b-value was reported in all except 6 articles.24,53,74,96,99,100 All articles except 7 used a single b-value in addition to zero.25,59⇓⇓⇓–63,81 The 7 articles using multiple b-values each used 5 unique b-values. The average b-value was 947, the range of b-values was 300–1590, and the median and the mode were 1000.
Spatial resolution is an additional important consideration. Assessments of anisotropy, which are central to studies of TBI, measure the aggregate range of diffusivities across the tissues composing the voxel. Partial volume effects that may spuriously reduce anisotropy will be more likely when larger voxel volumes are examined. Voxel sizes varied among the articles we reviewed, with an average voxel size of 11.3 mL3 (range, 1.83–31.25 mL3). Average section thickness was 3.08 mm (range, 1.72–6 mm).
Data Analysis Methods
DTI can be used to study brain structure either on a regional or a whole-brain level. Regional analyses include both those in which an a priori region of interest is chosen for study and tractography, in which an a priori region of interest is used to define a white matter tract for study. In both approaches, average diffusion values such as FA are extracted from voxels within the ROIs or tracts for subsequent analysis. Whole-brain analyses include voxelwise analyses, tract-based spatial statistics, a specialized type of voxelwise analysis, and histogram analyses of all brain or all white matter voxels.
In our review of the literature, we found that among those studies using regional analyses, 60 studies3⇓⇓–6,10,12⇓⇓⇓⇓⇓⇓–19,22⇓⇓⇓⇓⇓–28,30,33⇓–35,37⇓⇓⇓–41,43,46,48,49,51,52,54,55,57⇓⇓⇓⇓⇓⇓⇓⇓–66,76,81,82,86,92,93,95⇓⇓⇓⇓–100,102 used a region-of-interest approach and 30 studies9,11,17⇓–19,21,31,41,42,46,47,50,55,58,63,67,69,72,73,75,77,79,80,83,84,87,88,91,95,101 used tractography. Fewer studies used whole-brain analyses, of which 17 studies7,11,20,21,29,44,45,50,53,56,58,71,74,80,95,98,101 were based on a voxelwise approach, 7 studies14,32,36,68,78,86,100 used TBSS, and 4 studies8,34,44,50 used histogram analysis. Cross-validation of approaches can be achieved by using multiple analytic strategies. For instance, 1 article that used both a voxelwise analysis and TBSS found abnormalities in the same areas by using both techniques.70 In our review of the literature, we found that 18 articles reported using >1 type of analysis.6,14,17⇓–19,27,34,41,46,50,55,58,63,80,86,95,98,100 Tables 1⇓–3 show the most commonly identified areas of abnormal FA in region-of-interest, tractography, and whole-brain analyses; the most commonly implicated regions are generally similar across approaches. However, they are not entirely consistent. For example, the centrum semiovale and the brain stem are locations where abnormal FA has commonly been identified by using region-of-interest analysis, but these locations are not commonly identified by using either tractography or whole-brain analysis. Additionally, the superior longitudinal fasciculus is the most commonly identified location with abnormal FA by using whole-brain analysis, but this region does not appear as a common location by using either region-of-interest analysis or tractography. This discrepancy may be due to the fact that the superior longitudinal fasciculus was examined infrequently and does not necessarily indicate that it is an uncommon site of TAI. Tables 4⇓–6 show the most commonly identified areas of abnormal MD in each of the region-of-interest, tractography, and whole-brain analyses. The corpus callosum is the most commonly identified region of abnormal FA and MD, perhaps because it is the largest white matter tract in the brain and an important site of TBI pathology. For both reasons, the corpus callosum is commonly chosen as a target of regional analyses, a choice that may bias the net findings of the literature.
Most common locations of abnormal FA by ROI analysisa
Most common locations of abnormal FA by tractographya
Most common locations of abnormal FA by whole-brain analysisa
Most common locations of abnormal mean diffusivity by ROI analysisa
Most common locations of abnormal mean diffusivity by tractography analysisa
Most common locations of abnormal mean diffusivity by whole-brain analysisa
The reliability of regional analyses depends on accurate and reproducible spatial localization of ROIs or tracts across subjects. Approaches to ensuring reliability may include specific reliability and reproducibility testing when expert observers perform placement of ROIs. Alternatively, subject images may be spatially normalized to a standard template, with placement of ROIs based on the template. This latter approach ensures that region-of-interest placement is consistent among subjects; however, it depends on the robustness of the registration of the subject brains to a standard space. Fourteen articles used spatial normalization to ensure standardization of region-of-interest/tract location.5,13,14,35,54,61⇓–63,72,73,77,86,92,100 Sixty-three articles used expert manual placement of regions of interest.3,4,6,9⇓–11,15,16,19,22⇓⇓⇓⇓⇓–28,30,31,33,34,37⇓⇓⇓⇓⇓–43,46⇓⇓⇓⇓–51,55,57,59,60,63⇓⇓⇓–67,69,72,75,76,80⇓⇓⇓⇓–85,87⇓–89,91,93⇓–95,97⇓–99,102 However, only 35 of 63 studies reported that they performed reliability assessments, such as inter-/intraobserver reliability.6,9⇓–11,19,25,40⇓⇓–43,46,47,49,53,55,59,60,64⇓⇓–67,75,76,81,83⇓–85,87⇓–89,91,93,94,98,99 The studies that did report reliability testing included 63% (18/30) of articles using tractography9,11,19,41,42,46,47,55,67,75,83⇓–85,87⇓–89,91,94 but only 31% (19/61) of articles using region-of-interest analyses.6,10,19,25,40,41,43,46,55,59,60,64⇓–66,76,81,93,98,99
In comparing articles using whole-brain approaches, 5/8 of the TBSS studies found significant abnormalities,14,32,36,68,78 whereas all of the articles using voxelwise approaches identified significant differences. The greater likelihood of identifying abnormalities through voxelwise approaches as opposed to TBSS might be indicative of spurious group differences between patients and controls due to misalignment between subjects and the standard template, an issue that may be minimized by the TBSS approach.107 On the other hand, TBSS may be inherently less sensitive because the analyses are restricted to a limited white matter skeleton.
Specific Diffusion Measures Studied
Diffusion tensor imaging yields multiple measures at each voxel. FA describes the directional coherence of water diffusion in tissue. MD is the scalar measure of the total direction-independent diffusion within a voxel. Axial diffusivity describes diffusion along the principal axis of the diffusion ellipsoid, while radial diffusivity is an average of diffusion along its 2 minor axes. FA was the most commonly studied parameter across the studies we reviewed. Abnormally low FA is widely held to represent alterations of white matter microstructure consistent with TAI.108 Elevations of FA have been much less frequently reported (see below). Although some authors have hypothesized that abnormally high FA represents cytotoxic edema,54 the mechanistic basis of abnormally high FA remains uncertain.
FA was examined in all studies. All 100 articles, except for 46,54,89,96 (which showed elevated FA), described findings of low FA in subjects with TBI, regardless of the time of injury and across the spectrum of injury severity. MD is the next most commonly reported parameter (n = 51).3,9,10,13⇓⇓⇓–17,19,21,22,25,28,29,33⇓⇓⇓⇓⇓⇓–40,42,43,48⇓–50,55,56,59⇓⇓⇓–63,66,67,69,71,72,76,77,81,83,90,91,93,95,96,100⇓–102 Articles that examined parameters other than FA almost always identified areas of abnormal FA and then assessed other parameters within these regions. One article initially identified loci of abnormal MD and then assessed FA in the regions of abnormal MD.20 Axial diffusivity and radial diffusivity were much less commonly assessed (n = 18).3,8,11,13,14,20,22,36⇓–38,49,54,56,63,66,76,81,89 Only 2 articles reported radial diffusivity and not axial diffusivity.29,66 One article used a predictive model in which all 4 measures were incorporated.65
While FA is a useful summary measure, more detailed information regarding diffusional uniformity, potentially obtainable through study of eigenvalue measures, may be important for diagnosis and outcome prediction and especially for understanding pathologic mechanisms of TBI in humans. Eigenvalue measures implicate specific pathologic mechanisms in animal models of TBI and other types of brain injury.2 Including eigenvalue measures in a future study would facilitate a transitional bridge from animal to human studies and enable more informed targeting of novel interventions in a patient group with few therapeutic options.
Brain Regions
Brain regions examined varied greatly among the articles. We systematically tabulated the location of abnormal DTI measures (FA and MD separately) across all articles (Tables 1⇑⇑⇑⇑–6). To effectively summarize a large number of regions, we list only the top 10 most commonly identified regions of abnormal FA and the top 5 most commonly identified regions of abnormal MD via region-of-interest, tractography, and whole-brain analyses. When tabulating abnormal regions, it is important to recognize the relationship between study design and detection—that is, regional analyses can only detect a region as abnormal if the study design specifically examines that region. Whole-brain analyses, on the other hand, are positioned to detect all abnormal areas in the brain. Thus, the number of studies reporting an area as abnormal is influenced by the study design. Nonetheless, overall we found a large degree of consistency between studies regardless of the method of analysis. The corpus callosum, frontal lobe, internal capsule, and cingulum are among the most commonly identified regions of abnormality in DTI studies of TBI, perhaps because these structures are particularly vulnerable to injury due to their anatomic relationship to the skull and other structures such as the falx cerebri. These findings are almost entirely based on group comparisons and, therefore, do not necessarily reflect the distribution of injuries in the individual.
Functional Outcomes after TBI
Seventy-two of 100 articles examined outcomes associated with TBI in addition to the imaging findings,4⇓⇓⇓⇓–9,11,13,14,16⇓⇓⇓⇓⇓⇓–23,25,27,30,33,36⇓⇓⇓⇓⇓⇓–43,45⇓–47,49⇓⇓⇓⇓⇓⇓⇓⇓⇓–59,61,62,64⇓⇓⇓–68,70,71,74⇓–76,78,80⇓–82,84,87⇓⇓⇓⇓⇓⇓–94,96,98,101,102 and almost all of these 72 articles reported specifically on the association of DTI findings with the outcomes. Most surprising however, 3 articles, though they reported outcomes, did not report analysis of the relationship between the outcome measures and DTI.27,35,56 Fifty-one of the 72 articles assessed neuropsychological outcomes.5⇓–7,9⇓⇓⇓⇓–14,16⇓⇓–19,22,23,25,27,30,36⇓⇓–39,41⇓–43,45,46,50⇓–52,54,57⇓⇓–60,64,65,67,68,74,75,80,81,88,90⇓⇓⇓–94,96,102 Eighteen of 72 used a global outcome measure (eg, Glasgow Outcomes Scale, Coma Recovery Scale, Mini-Mental Status Examination),4,16,22,33,42,50,57⇓–59,63,66,70,76,80⇓–82,84,88 14 articles reported correlation with the GCS,4,5,7,8,22,33,38,42,61,62,66,87,91,98 8 articles correlated FA with intelligence quotient,5,14,16,22,54,58,80,92 and 12 articles examined the relationship between DTI and postconcussive symptoms (eg, headaches, visual disturbances, cognitive symptoms) and/or mood disorders.6,20,23,40,53,54,78,80,81,89,92,99 Several articles reported the association of DTI with other patient assessments as surrogate outcome measures. These measures included electroencephalography,79 fMRI,10,63,69,75,90,100 MR spectroscopy,5,82 regional brain volumes,85 and motor-evoked potentials.97
Of the articles that correlated DTI metrics with outcome, we found considerable heterogeneity among studies with respect to the specific outcome measures used. Choice of specific neuropsychological tests was most variable, with only a few articles reporting the same measure (range, 1–19; mean, 1.8; median, 1.5). To summarize the data from these studies, we divided the various outcome measures into domains, including the following: attention, executive function, memory, motor function, psychomotor/processing speed, visuospatial function, global outcome, GCS, intelligence quotient, and postconcussive symptoms. Tables 7 and 8 summarize the significant associations reported between DTI metrics and these outcome categories.
Relationship of DTI metrics to cognitive outcome measuresa
Relationship of DTI metrics to general clinical assessmentsa
In addition to heterogeneity of the outcome measures used, additional variability (eg, brain region examined, analysis type, and DTI metric assessed) among studies examining the same outcome domain further complicated summary of the literature. The average number of studies examining the same outcome domain was 15 (range, 6–29; Tables 7 and 8). However, even among articles examining the same domain, results are inconsistent.
Discordance in the results of outcome studies can, perhaps, be attributed to several issues. Although studies may examine the same domain, they typically vary in the choice of the specific measure/instrument used. Because the sensitivity and specificity of any 2 measures, though designed to test the same cognitive domain, for instance, will differ,109 results of studies relating imaging to these differing outcome measures will potentially differ between the 2 studies as well. Moreover, the severity of TBI might determine the extent to which a patient experiences impairment in cognition or other adverse outcomes. As a result, comparison between studies including different injury severities might not be appropriate. Finally, impairment secondary to TBI, particularly mild TBI, can be subtle and, therefore, escape detection by using some formal testing tools. Perhaps the most salient message to be derived from this segment of the literature is that standardization of outcome measures and study design is essential to future meaningful study of TBI.110
Assessment of Individual Patients with TBI
The heterogeneity of injury mechanisms that cause TBI is likely best captured in studies assessing individual patients with TBI; group comparisons are inherently insensitive to interindividual variation, which is a hallmark of TBI. All of the articles included in this review report group analyses of patients with TBI. However, >35 additional articles report the use of DTI in individual TBI cases (eg, Gold and Lipton111). Several of the articles included in this review reported assessment of individual patients in addition to their group analyses. Two articles examined whole-brain white matter histograms of individual patients,8,50 but only 1 reported results at the single-subject level, finding the distribution of FA in patients with TBI to be skewed toward lower FA in comparison with controls.8 Three articles applied a tractography approach to individual subjects,31,58,63 while 2 articles applied the whole-brain approach to individuals.44,50 Assessment of individual patients with TBI is important to the characterization of outliers, who might differ from the group in terms of extent and spatial distribution of injury, and is a prerequisite to clinical use of DTI in evaluating patients with TBI.
Implications, Limitations, and Possibilities
DTI has been studied extensively as a tool for identification of brain abnormalities related to TBI and to understand the relationship of these brain abnormalities to other clinical features of the disorder. During the past decade, the number of such studies has risen exponentially and continues to increase with no sign of abatement. A unifying theme can be deduced from this large body of research: DTI is an extremely useful and robust tool for the detection of TBI-related brain abnormalities. The overwhelming consensus of these studies is that low white matter FA is characteristic of TBI. This finding is consistent across almost all the articles we reviewed, despite significant variability in patient demographics, modest differences in data acquisition parameters, and a multiplicity of data analysis techniques. This consistency across studies attests to the robustness of DTI as a measure of brain injury in TBI. The finding of significant differences in FA histograms that pool all white matter voxels across the whole brain is particularly compelling, indicating that a substantial portion of the hundreds of thousands of voxels in the image datasets are abnormal.
We also found an overwhelming consensus that imaging abnormalities detected with DTI are associated with important clinical outcomes. This further validates DTI as a meaningful measure of clinically important brain injury. However, heterogeneity among the outcome measures that have been reported limits our ability to draw direct generalizable connections between DTI abnormalities at specific brain locations and specific outcomes. The greatest degree of variability among the studies we reviewed was in the choice of outcome measures. As others have suggested, an important priority for future studies of TBI should be the use of standardized approaches, particularly standardization of outcome measures.112 Additionally, more high-quality longitudinal studies are needed to extend the power of DTI, from identifying patients with TBI at cross-section to accurately predicting future clinical status.
By far, FA was the DTI measure used most commonly across the studies we reviewed. Too few articles reported analyses of eigenvalues to permit meaningful inferences regarding the role of eigenvalue findings in the assessment of TBI at this time. This is an important area of deficiency because preclinical studies indicate that differential effects on eigenvalue measures can separate pathologic mechanisms. Thus, more detailed study of the full palette of metrics available from DTI is a great area for future study.
The variety of data analysis approaches applied across the studies we reviewed presents a significant obstacle to summary of the data and limits the inferences that can be made on the basis of the literature as a whole. It is primarily on the basis of this factor that we determined that meta-analysis methods would not be appropriate for assessment of this literature. Studies reporting regional analyses might be considered comparable on the basis of similarity of brain regions tested across multiple studies. However, the precise spatial location represented by a given region-of-interest, tract, or brain structure descriptors may vary significantly among studies on the basis of the methods, criteria, and raters used to define ROIs. Intra- and inter-rater variability can confound inferences based on these studies. While reliability testing can and should be performed to verify the reproducibility of region-of-interest placement, only a minority of studies did so.
Whole-brain analyses perhaps offer the greatest promise for pooling of results across studies, provided that the studies normalize their image data to the same brain template. Variability in the brain atlases used for spatial normalization and inconsistent reporting of coordinates for abnormalities in the studies we reviewed limit such cross-study comparison at this time.
All articles captured by our review used group analyses, though several also incorporated assessments of individual patients with TBI. Group-analysis approaches are powerful means for improving statistical power. However, the use of a group analysis limits the study to detection of abnormalities that occur in the same location in all patients. The fact that robust group effects have been reproduced in studies of DTI in patients with TBI is consistent with long-standing concepts that identify certain brain regions as particularly susceptible to TAI. Intersubject differences in the mechanism of injury as well as other biomechanical factors such as head and body composition make it highly probable that despite some commonalities, many areas of injury will differ among patients. Further application of individualized assessments of regional brain injury is thus needed to realize the full potential of DTI as a research and clinical tool.
On the basis of our analysis of the current literature, we suggest that important focus areas for future study should include larger longitudinal studies, incorporation of multiple outcome measures in statistical models that account for the complexity inherent in TBI populations, and assessment of interindividual differences. Standardization across centers, specifically with regard to data acquisition parameters, data analysis techniques, and the specific outcome measures assessed, promises to greatly increase the yield of such studies.
In summary, DTI provides a robust measure of clinically important TAI at cross-section, despite the variability inherent in characteristics of patients with TBI and injury mechanisms as well as study differences in data acquisition and analysis methods. Larger longitudinal studies will be essential for the evaluation of DTI as a prognostic biomarker in TBI. More detailed assessment of DTI metrics and translational imaging studies should be undertaken to link pathophysiologic mechanisms in animal models to important clinical outcomes in patients. Together, these approaches promise to realize the full potential of DTI to improve diagnosis and treatment of patients with TBI.
Acknowledgments
We thank Tova M. Gardin for graphic arts assistance.
Footnotes
Disclosures: Molly E. Zimmerman—UNRELATED: Grants/Grants Pending: National Institutes of Health (NIH)/National Institute on Aging,* Alzheimer's Association,* Bristol-Myers Squibb.* Michael L. Lipton—UNRELATED: Grants/Grants Pending: NIH,* Dana Foundation,* Resurrecting Lives Foundation,* Patents (planned, pending, or issued): Einstein patent pending,* Comments: for data analysis techniques. *Money paid to the institution.
Indicates open access to non-subscribers at www.ajnr.org
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- © 2013 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- ABBREVIATIONS:
- Subjects with TBI
- Severity, Chronicity, and Study Design
- Data Acquisition Parameters
- Data Analysis Methods
- Specific Diffusion Measures Studied
- Brain Regions
- Functional Outcomes after TBI
- Assessment of Individual Patients with TBI
- Implications, Limitations, and Possibilities
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Supplemental
- References
- Info & Metrics
Related Articles
Cited By...
- Brain volume changes following blast-related mild TBI in service members and veterans: a LIMBIC-CENC study
- Disrupted maturation of white matter microstructure after concussion contributes to internalizing behavior problems in female children
- Automated detection of axonal damage along white matter tracts in acute severe traumatic brain injury
- Towards Understanding Comprehensive Morphometric Changes and Its Correlation with Cognition and Exposure to Fighting in Active Professional Boxers
- Abnormal Neurite Density and Orientation Dispersion in Frontal Lobe Link to Elevated Hyperactive/Impulsive Behaviors in Young Adults with Traumatic Brain Injury
- White Matter Disruption in Pediatric Traumatic Brain Injury: Results From ENIGMA Pediatric Moderate to Severe Traumatic Brain Injury
- Multi-tract multi-symptom relationships in pediatric concussion
- Traumatic Cerebral Microbleeds in the Subacute Phase Are Practical and Early Predictors of Abnormality of the Normal-Appearing White Matter in the Chronic Phase
- Connectomic Assessment of Injury Burden and Longitudinal Structural Network Alterations in Moderate-to-severe Traumatic Brain Injury
- White matter and concussion: Are we on the right tract?
- Neurofilament light as a biomarker in traumatic brain injury
- Time course and diagnostic utility of NfL, tau, GFAP, and UCH-L1 in subacute and chronic TBI
- Tractography-Pathology Correlations in Traumatic Brain Injury: A TRACK-TBI Study
- Neuropsychological outcomes following traumatic brain injury
- Randomised controlled clinical trial of a structured cognitive rehabilitation in patients with attention deficit following mild traumatic brain injury: study protocol
- Structural abnormalities in thalamo-prefrontal tracks revealed by high angular resolution diffusion imaging predict working memory scores in concussed children
- Relationship between white matter integrity and post-traumatic cognitive deficits: a systematic review and meta-analysis
- Defining an Analytic Framework to Evaluate Quantitative MRI Markers of Traumatic Axonal Injury: Preliminary Results in a Mouse Closed Head Injury Model
- Diverging white matter trajectories in children after traumatic brain injury: The RAPBI study
- Trauma Imaging: A Literature Review
- Analysis of head impact exposure and brain microstructure response in a season-long application of a jugular vein compression collar: a prospective, neuroimaging investigation in American football
- Principal Component Analysis of Diffusion Tensor Images to Determine White Matter Injury Patterns Underlying Postconcussive Headache
- Imaging assessment of traumatic brain injury
- Callosal Function in Pediatric Traumatic Brain Injury Linked to Disrupted White Matter Integrity
- Imaging Evidence and Recommendations for Traumatic Brain Injury: Advanced Neuro- and Neurovascular Imaging Techniques
- Classification algorithms using multiple MRI features in mild traumatic brain injury
- Single-Neuron NMDA Receptor Phenotype Influences Neuronal Rewiring and Reintegration following Traumatic Injury