
Abstract
BACKGROUND AND PURPOSE: Imaging self-referral is increasingly cited as a contributor to diagnostic imaging overuse. The purpose of this study was to determine whether ownership of MR imaging equipment by ordering physicians influences the frequency of negative cervical spine MR imaging findings.
MATERIALS AND METHODS: A retrospective review was performed of 500 consecutive cervical spine MRIs ordered by 2 separate referring-physician groups serving the same geographic community. The first group owned the scanners used and received technical fees for their use, while the second group did not. Final reports were reviewed, and for each group, the percentage of negative study findings and the frequency of abnormalities were calculated. The number of concomitant shoulder MRIs was recorded.
RESULTS: Five hundred MRIs meeting inclusion criteria were reviewed (250 with financial interest, 250 with no financial interest). Three hundred fifty-two had negative findings (190 with financial interest, 162 with no financial interest); there were 17.3% more scans with negative findings in the financial interest group (P = .006). Among scans with positive findings, there was no significant difference in the mean number of lesions per scan, controlled for age (1.90 with financial interest, 2.19 with no financial interest; P = .23). Patients in the financial interest group were more likely to undergo concomitant shoulder MR imaging (24 with financial interest, 11 with no financial interest; P = .02).
CONCLUSIONS: Cervical spine MRIs referred by physicians with a financial interest in the imaging equipment used were significantly more likely to have negative findings. There was otherwise a highly similar distribution and severity of disease between the 2 patient samples. Patients in the financial interest group were more likely to undergo concomitant shoulder MR imaging.
ABBREVIATIONS:
- FI
- financial interest
- NFI
- no financial interest
- OEDS
- order entry decision support
United States health care expenditures grew 3.9% in 2011, reaching $2.7 trillion or an estimated 17.9% of the gross domestic product.1 Health care spending is projected to continue to grow in 2012 and 2013 at 4.2% and 3.8%, respectively.2 Diagnostic imaging costs remain a large component of annual health care expenditures and have, therefore, been targeted in an effort to contain costs. While the proportion of growth in health care expenditures attributable to diagnostic imaging use has decreased considerably in recent years, medical imaging use among nonradiologist physicians continues to increase at a growth rate twice that of radiologists and remains a significant contributor to higher imaging use and cost.3
Imaging self-referral is defined as physicians referring their own patients for imaging to facilities in which they or their partners have financial interests.4⇓–6 In 1991, Medicare fraud-and-abuse legislation was passed in an effort to curb the rising tide of medical imaging self-referral. Commonly referred to as the “Stark II law” after the primary author Representative Fortney “Pete” Stark (Democrat, California), the legislation bans physician referrals to entities in which they have a financial relationship.7 However, the inclusion of an in-office ancillary services exception (created with patient convenience in mind) permits physicians to both order and provide advanced imaging services for patients in their office. As a result, despite the presence of the Stark law, physician self-referral of medical imaging has continued to grow substantially.8
Critics of the practice of self-referral have asserted that it leads to overuse of diagnostic imaging and is, therefore, an important contributor to rising health care costs. In support of this argument, several previously published studies have demonstrated that the practice of imaging self-referral is increasing, that physicians who own diagnostic imaging equipment are more likely to refer their patients for imaging at facilities in which they have a financial interest, and that self-referral by nonradiologist physicians leads to higher overall imaging use.9⇓⇓⇓⇓⇓⇓⇓⇓–18 However, despite the growing body of literature documenting these findings, the conclusion that self-referral leads to inappropriate medical imaging use, or overuse, remains a topic of debate. This is, in part, secondary to the inherent challenges researchers face in demonstrating the similarity between 2 compared groups of patients, particularly with regard to rates and severity of disease, insurance status, and clearly discerning the financial arrangements of imaging equipment ownership.
Criticisms of prior studies linking imaging self-referral to overuse have focused on their inadequate consideration of use appropriateness. Determining the appropriateness of medical imaging use is a complex and challenging task confounded by multiple factors, including patient population (payer and insurance status and regional geographic differences), clinical setting (hospital versus outpatient practice), disease prevalence (young versus elderly), referral biases (eg, specialist versus primary care), diagnostic interpretation inhomogeneity (discordant “grading” of lesions) and terminology, or skill differences among interpreting radiologists. In many scenarios, these factors become uncontrollable variables that complicate attempts to compare the appropriateness of referrals for medical imaging between groups of physicians, including between groups with and without financial relationships to the medical imaging equipment. Prior effort has evaluated differences in the volume of patients referred for medical imaging between the 2 groups based on International Classification of Diseases-9 diagnosis codes and use per patient encounter. This approach has flaws because both the proportion of examinations with normal findings and the differences in prevalence and severity of disease between the 2 compared groups are not evaluated. Without this additional information, comparisons of relative use may be feasible, but not the appropriateness of imaging use.
Comparing the proportion of imaging examinations with negative findings, after controlling for potential confounding variables, would allow an accurate assessment of the differences in imaging referral patterns between the 2 physician groups (financially incentivized and nonfinancially incentivized). This would not only validate previously published studies on imaging appropriateness but also add to the existing body of literature addressing the issue of self-referral. Furthermore, an analysis of the prevalence and severity of imaging-confirmed pathology between these groups may serve as a surrogate for disease prevalence and overall severity within the 2 different patient populations, because groups with equal disease prevalence and severity should manifest an equivalent number of positive imaging findings.
The purpose of this study was to determine whether ownership of MR imaging equipment by an ordering physician group affects the use of cervical spine MR imaging. This was accomplished by comparing the likelihood of negative cervical spine MR imaging findings and the cervical spine MR imaging pathology rates between the 2 groups. We wished to test the null hypothesis that no such difference exists and that usage patterns are the same. This was accomplished via evaluation of 2 subordinate hypotheses: 1) There is no difference in the rate of examinations with negative findings between self-referred and non-self-referred MR imaging examinations, and 2) among examinations with positive findings, there are no differences in the prevalence of individual pathology subtypes between the 2 groups. We considered that no difference in the first would indicate that no excess ordering of examinations occurred in either group and that no difference in the second would mean that the 2 patient groups were highly similar with regard to the rate and type of pathology.
Materials and Methods
This retrospective Health Insurance Portability and Accountability Act–compliant study was approved by the institutional review board of the appropriate medical center, and a waiver of informed consent was granted. Chronologically consecutive cervical spine MR imaging reports were reviewed from February to September of 2009 in 1 academic musculoskeletal imaging practice, consisting of 5 attending radiologists. Each interpreting radiologist was a subspecialty-trained musculoskeletal imager, with a mean of 14 years (range, 5–23 years) of experience exclusively in musculoskeletal radiology. MR imaging examinations that met the inclusion criteria were analyzed from each of 2 groups in tandem so that each cohort would, by design, have the same number of studies. The first group was ordered by orthopedists who had imaging performed on MR imaging equipment owned by that same orthopedic group (financial interest [FI]). The second group of scans was ordered by a different group of orthopedists in the same community who did not own or have other financial interest in the MR imaging equipment used (no financial interest [NFI]). The physical locations of the referring physician group outpatient clinical practices were recorded. The residency training institution and years in practice of the referring physicians were also recorded for each group. The source of the data base, all physician groups, and identifying details including locations are purposely kept anonymous.
All cervical spine MR imaging examinations from both referring physician groups (FI and NFI) were performed at 1.5T field strength using identical protocols and were interpreted by the same subspecialty musculoskeletal radiology practice. The interpreting radiology practice had no financial interest in the imaging equipment used for either patient group. Patients with prior cervical spine surgery or prior cervical spine MR imaging examinations were excluded to help eliminate the potential confounding effects of prior surgery and postoperative changes and to control for any differences in the follow-up practice patterns between the 2 groups. Inclusion criteria were first-time cervical spine MR imaging examinations performed as an outpatient. Final reports were reviewed and examinations with the following findings were considered positive: “moderate-to-severe” or “severe” spinal canal stenosis, moderate-to-severe or severe neuroforaminal narrowing, moderate-to-severe or severe facet degenerative changes, moderate-to-severe or severe disk herniation contacting the cord, and osseous abnormalities (the most common being fracture). These findings were chosen because they represent significant pathology that is more likely to be an etiology of neck pain for which treatment may be considered. The number of disk interspace levels exhibiting ≥1 of the above findings was recorded. Patient age and sex were recorded, as was the acquisition of concomitant shoulder MR imaging examinations.
The percentage of scans with negative findings was tabulated for each group. Because it was possible for scans with positive findings to contain multiple lesions and that each of these lesions could represent an etiology for neck pain or radicular symptoms, the total number of lesions per scan was calculated for each of the examinations with positive findings in each group.
Statistical Analysis
Using a significance threshold of α = .05, 2-tailed, we performed a power analysis that showed that we would have >90% power to detect a difference in rates of scans with negative findings of 50% (n = 250) and 35% (n = 250) in conditions comparing financial interest with no financial interest.
In 2-sample comparisons when covarying for age was not needed, χ2 tests were used for the binomial variables; Fisher exact tests, for comparisons with fewer than 5 observations in a cell; and t tests, for the continuous variables. Logistic regression was used to predict negative scan outcomes by using age as a covariate. ANCOVA was used to identify mean differences in characteristics of scans with positive findings with age as a covariate. χ2 and t test P values reported in this article are 2-tailed, and statistical significance was considered at a threshold of P < .05. All statistical analyses were conducted by using SPSS 21 and 22 (IBM, Armonk, New York).
Results
Five hundred examinations (250 in the FI group and 250 in the NFI group) that met the inclusion criteria during the study period were evaluated. There was no statistically significant difference in the distribution of sex between the 2 groups (P = .14) (Table). There was a statistically significant difference in mean patient age between the 2 groups, 48.4 years (range, 13–78 years) for FI and 54.3 years (range, 15–86 years) for NFI (P < .001). Given this difference and the known propensity for increased frequency and severity of degenerative changes with increased age, ANCOVA subanalyses were conducted by using age as a covariate.
Distribution of sex
Negative Examination Findings
Among the 500 examinations, 352 had negative findings (190 in FI and 162 in NFI). There were 17.3% more scans with negative findings in the FI group, a difference that was statistically significant (P = .006) (Fig 1).

Negative cervical spine MR imaging rates (with 95% CIs). There was a 17.3% increase in the negative examination rate in the FI group (P = .006).
Positive Examination Findings
Among examinations with positive findings, there was no statistically significant difference in the mean number of lesions per scan between the NFI (n = 2.19) and FI (n = 1.90) groups (P = .23) or in the mean number of positive levels per scan between the 2 groups (NFI = 1.59, FI = 1.56, P = .80), adjusted for age. If one compared the frequencies of the evaluated abnormality subtypes, there was no significant difference in the mean number of neuroforaminal stenoses (NFI = 1.09, FI = 0.87; P = .32), disk abnormalities (NFI = 0.75, FI = 0.81; P = .68), or facet degenerative changes (NFI = 0.26, FI = 0.23; P = .81) per scan, adjusted for age. The number of examinations containing descriptors of canal stenosis was too small for meaningful analysis (NFI = 5, FI = 1).
Concurrent Shoulder MR Imaging
Patients in the FI group were significantly more likely to undergo concurrent shoulder MR imaging while undergoing cervical spine MR imaging than those in the NFI group: 24 and 11, respectively (P = .02) (Fig 2). Among patients undergoing concomitant shoulder MRI, there was a proportionally greater number of patients with cervical spine MRIs with normal findings in the FI group (23 of 24, 95.8%) in comparison with the NFI group (8 of 11, 72.7%) (P = .08). A greater percentage of concurrent shoulder MRIs obtained in the FI group had negative findings (FI: 8 of 24, 33.3%; NFI: 1 of 11, 9.1%) (P = .22). When patients underwent concurrent shoulder and cervical spine MR imaging and the cervical spine MR imaging findings were negative, all of the NFI group shoulder scans had positive findings (8 of 8), while only 14 of the 23 FI cases had positive findings (P = .003).
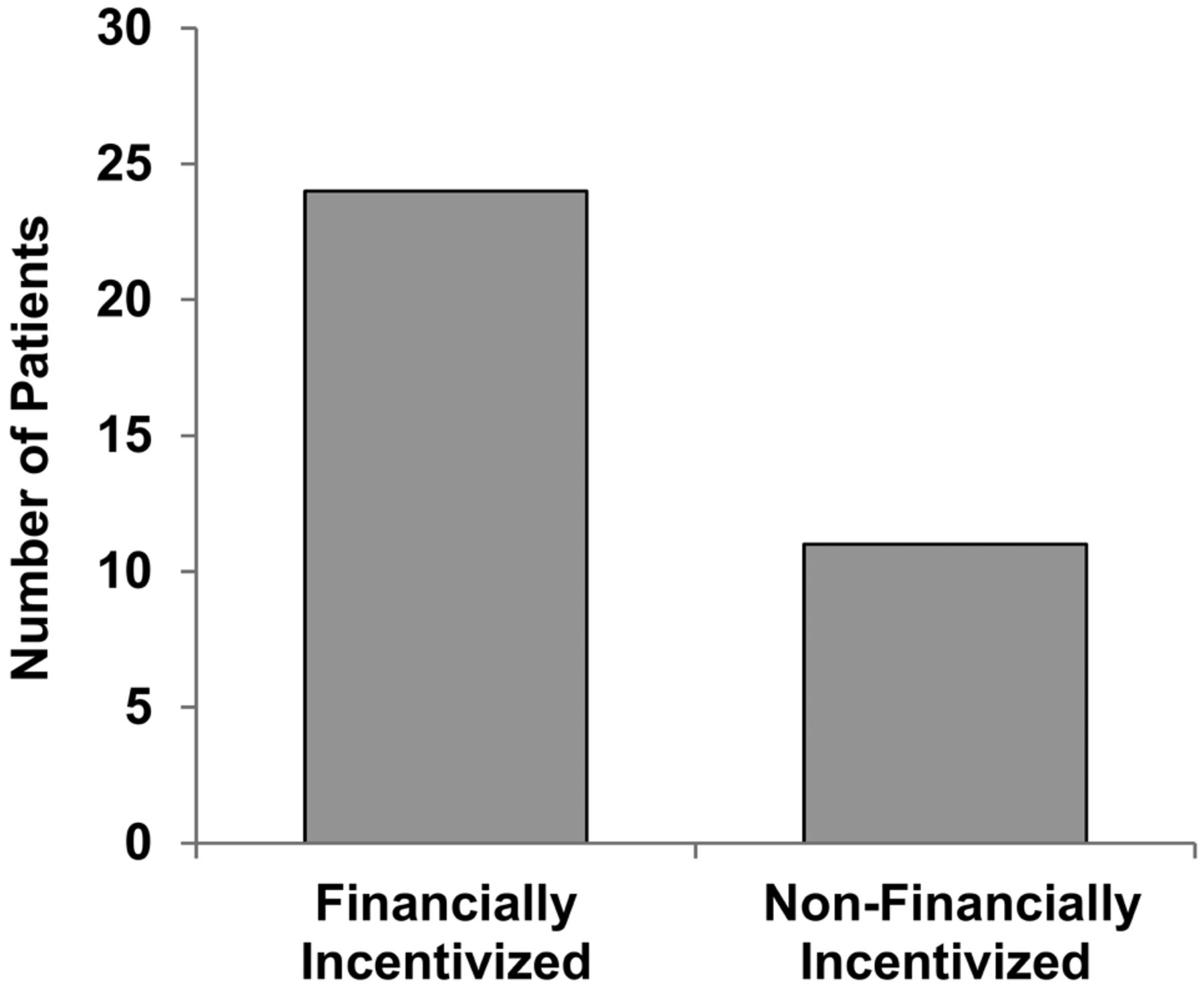
The number of concurrent shoulder MR imaging scans obtained. Patients in the FI group were significantly more likely to undergo concurrent shoulder MR imaging (P = .02).
Referring Physician Characteristics
Most orthopedic clinics for the FI and NFI groups were within close geographic proximity to each other, because all were located within the same 50-mile radius. Nearly equal percentages of the referring clinicians from each group (54% FI, 53% NFI) trained at a single common orthopedic residency program (P = 1.0). Both groups had similar proportions of physicians with subspecialty or fellowship training (P = .076), and both were similar in size. Finally, there were comparable mean years of practice between both groups (14.2 years for NFI, 14.1 years for FI; P = .526).
Discussion
The purpose of this study was to evaluate the differences in the use of cervical spine MR imaging between 2 groups of physicians, 1 with a financial interest in the imaging equipment used and 1 without. Our results demonstrate a 17.3% increased negative examination rate among patients referred by the physician group with a financial interest in the imaging equipment used (P = .006). Therefore, we reject the null hypothesis number 1. This suggests that there may be a reduced threshold for obtaining cervical spine MR imaging in the presence of a financial incentive, whether conscious or unconscious.
A wealth of literature exists on the topic of physician imaging self-referral. Many of these prior studies have attempted to compare use between 2 physician groups based on Medicare billing data.19,20 Criticism of this method has often centered on an inability to adequately assess the appropriateness of imaging use and on the failure of the method to account for the many complexities driving use, such as differences in disease severity between patient groups. Indeed, accurately evaluating the relationship between imaging self-referral and financial incentive is extremely challenging and would require consideration of a multitude of factors including patient populations, referral biases (specialist versus primary care), clinical setting (outpatient versus hospital), disease prevalence, variations in diagnostic standards (discordant “grading” of severity), differences in imaging protocols and equipment, and differences in terminology used by interpreting radiologists.
Our study used a recently developed method to examine imaging self-referral that is focused on use appropriateness rather than a simple count of use per patient. Rather than reviewing billing data or imaging indications, we analyzed the final diagnoses on imaging examinations, thereby helping to control for differences in the severity of disease between different referring physician groups (FI and NFI). This method for comparing patient cohort similarity was used in several prior publications.21⇓–23 Furthermore, a single small academic radiology group interpreted all examinations from both referring physician groups; this helps to control for radiologist interreader variation. Additionally, because this radiology group did not own any of the imaging equipment, there was no confounding financial interest.
We found no statistically significant difference in the average number of abnormalities per study with positive findings or in the number of positive levels per scan between the NFI and FI groups. Additionally, there was no significant difference in the rates of neuroforaminal stenosis, disk bulge, or facet degenerative change. This similarity in the abnormality rate per positive scan confirms the null hypothesis number 2 and suggests that the 2 patient groups had a comparable prevalence of pathology. Assuming that abnormalities found on studies with positive findings act as surrogates for the disease prevalence within both patient populations, the 2 groups appear to significantly differ only in their rates of cervical spine MR imaging studies with negative findings. We suspect that the divergent negative examination rate may reflect differences in decision-making in patients presenting with cervicalgia, particularly in regard to the threshold for acquiring imaging.
It is of particular interest that the FI group patients were more likely to receive concomitant shoulder MR imaging (P = .02). Because it is often challenging to differentiate between a cervicogenic and rotator cuff etiology for upper extremity pain, this clinical challenge was likely present in both patient populations.24 If patients in the FI group had a larger prevalence of shoulder pathology than the NFI group, this might lead to an increased rate of positive concomitant shoulder MR imaging findings. However, this was not the case. In fact, patients in the FI group were more likely to have normal findings on shoulder MRI (33.3% for FI versus 9.1% for NFI, P = .22). Furthermore, comparing the subgroups of patients that underwent both cervical spine and shoulder MR imaging revealed that FI patients were also more likely to have negative cervical spine MR imaging findings. Finally, 9 patients in the FI group had negative findings on both examinations versus no patients in the NFI group. These findings, while somewhat limited by the small sample size, demonstrate increased use of concomitant shoulder MR imaging in the FI group and suggest a trend toward considerably increased negative examination rates in keeping with the cervical spine MR imaging data.
There were several limitations to this investigation. First, the inherent complexities of both cervicalgia and cervical spine degenerative changes make it difficult to define a “true-positive” examination. This challenge is pervasive throughout daily clinical practice. For instance, confirming a causal relationship between suspected imaging findings and a patient's pain often requires feedback in the form of targeted treatment. While even “mild” degenerative changes can be symptomatic, an objective demarcation for positive examination findings was a prerequisite to investigation. It is possible that establishing a different threshold for positive examination findings or considering alternative pathologies could have led to different results. However, we chose to define severe degenerative change as positive because these findings are more likely to be causes of pain that are clinically important and result in therapy, such as steroid injections or surgery. A second limitation is the relatively limited number of concurrent shoulder MR imaging examinations, hindering the ability to achieve statistical significance in the analysis of components of this subset of our data. Additionally, we did not compare insurance status, ethnicity, or socioeconomic status between the 2 groups because these data were not available for review. Finally, there was a statistically significant difference in age between the 2 groups (54.3 for NFI, 48.4 for FI). This required the use of ANCOVA with age as a covariate to account for the known increased prevalence of spine degenerative changes with advanced age.
Despite these limitations, this study clearly demonstrates an increased negative examination rate in the physician group that collected technical fees for the imaging equipment used. We believe that this apparent bias, whether conscious or unconscious, is an important consideration when health care costs, more specifically medical imaging costs, are analyzed. An excessive negative scan rate on the order of 15%–20% is a considerable financial burden when extrapolated nationally. To date, the across-the-board cuts to imaging reimbursements have done nothing to address this bias and have, instead, placed future access to advanced imaging in jeopardy. Similar findings have previously been reported in the lumbar spine, shoulder, and knee.21⇓–23 These findings require validation across other geographic regions and medical practices.
The observed bias toward increased use of cervical spine MR imaging does not, by itself, prove intended overuse for profit. It is possible that other factors are at play influencing 1 physician group to image more frequently. Such considerations might include an imaging-intensive practice pattern less reliant on physical examination findings, perhaps secondary to differences in training. Similarly, one might purport that younger physicians may be more familiar with the use of MR imaging in diagnostic evaluations because it was part of their training, while more senior physicians may be more comfortable with alternative diagnostic methodologies (physical examination, myelography). Many of these physician-related considerations may not be significant factors in this study because the 2 groups were highly similar in terms of mean years of practice and number of trained subspecialists and had nearly equal percentages of physicians who trained at the same residency program.
Physician order entry decision support (OEDS) software has been proposed as a mechanism for decreasing the incidence of unnecessary imaging examinations. OEDS has proved success and could potentially reduce the rate of negative examination findings in both referral groups by providing recommendations according to the American College of Radiology appropriateness criteria for cervical spine MR imaging.25 However, in most cases, OEDS software does not include “hard stops” but rather allows referring physicians to override recommendations. Therefore, the FI and NFI groups would be able to continue to order examinations as they think appropriate. Furthermore, if practice patterns for either group involve order placement by clinic office staff, the appropriateness recommendations may be blindly overridden to follow attending physician requests.26 For these reasons, it is difficult to discern how the addition of OEDS would influence the ordering practice patterns of our referral groups.
Conclusions
This study demonstrates a significantly increased negative cervical spine MR imaging rate in patients referred by physicians with a financial interest in the imaging equipment used in comparison with those patients referred by physicians without such an interest. This increased negative examination rate occurred despite similar referring physician characteristics, patient demographics, and cervical spine pathology burden. Further study is warranted among a larger sample of physician practices and in different geographic regions to ascertain the extent of the issue and to further investigate the utility of comparing pathology frequencies between practices as a metric for imaging use appropriateness.
References
- Received April 21, 2014.
- Accepted after revision June 2, 2014.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.